Methotretate
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information to write a thorough response on methotrexate. Let me compile this into a well-organized answer.
Methotrexate (MTX)
Classification & Overview
Methotrexate is an antifolate antimetabolite — a synthetic analog of folic acid. Discovered in 1948, it was initially developed as a chemotherapeutic agent for hematologic malignancies and has since become a cornerstone drug in oncology, rheumatology, and dermatology.
Mechanism of Action
MTX enters cells via an active transport process and competitively and irreversibly inhibits dihydrofolate reductase (DHFR) — the enzyme that converts dihydrofolate (FH₂) → tetrahydrofolate (FH₄). This blocks the folate cycle and starves rapidly dividing cells of:
- Thymidylate (via blockade of thymidylate synthase)
- Purines (adenine, guanine) — by inhibiting glycinamide ribonucleotide transformylase (GART) and aminoimidazole carboxamide transformylase (AICA-T)
The net result is blockade of DNA and RNA synthesis, making MTX S-phase specific.
Additionally, MTX accumulates intracellularly as polyglutamate derivatives, which prolong its inhibitory activity on multiple folate-dependent enzymes and also inhibit DNA methylation via reduction of S-adenosylmethionine levels.
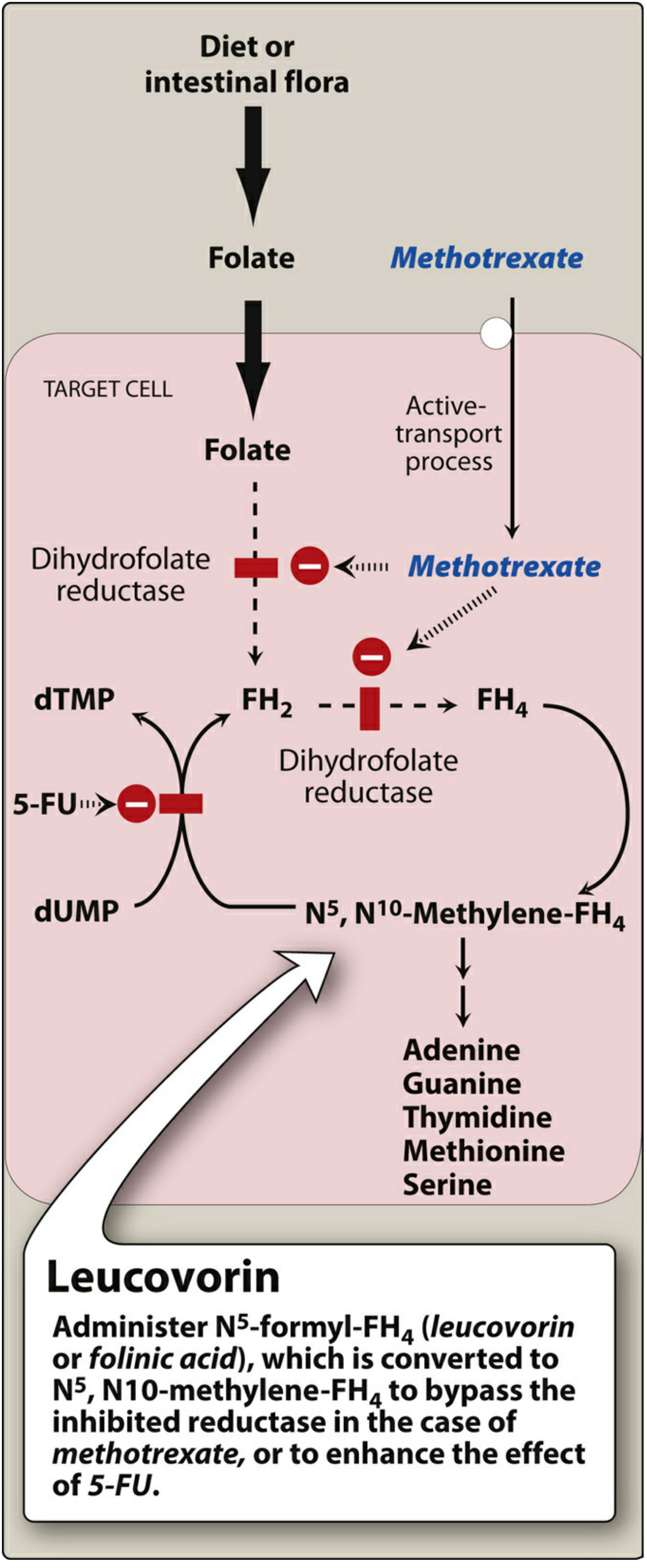
Inhibition can be reversed only by a 1000-fold excess of the natural substrate (FH₂) or by administration of leucovorin (folinic acid, N⁵-formyl-FH₄), which bypasses DHFR entirely.
Pharmacokinetics
| Parameter | Detail |
|---|---|
| Absorption | Oral bioavailability ~67%; variable at low doses; SC preferred for doses >20 mg/week (14–40% higher bioavailability vs. oral) |
| Distribution | High concentrations in intestinal epithelium, liver, kidney; distributes into skin, ascites, pleural effusions; does not readily cross blood-brain barrier |
| Protein binding | ~50% plasma protein bound |
| Metabolism | Minor: 7-hydroxylation → 7-OH-MTX (less water-soluble; risk of crystalluria) |
| Excretion | 60–95% excreted unchanged in urine (renal tubular secretion + GFR); triphasic kinetics — rapid distribution, then renal clearance t½ 2–3 h, then slow t½ 8–10 h |
| Routes | Oral, IM, IV, SC, intrathecal (for CNS sanctuary disease) |
Renal impairment significantly slows elimination and markedly increases toxicity risk. Alkalinizing the urine and ensuring adequate hydration are essential when using high doses to prevent MTX/7-OH-MTX precipitation in tubules.
Therapeutic Uses
Oncology
- Acute lymphocytic (lymphoblastic) leukemia (ALL) — including intrathecal for CNS prophylaxis/treatment
- Burkitt lymphoma (children)
- Choriocarcinoma (highly curative as single agent)
- Breast cancer, head and neck carcinomas
- Mycosis fungoides (FDA-approved)
- Non-Hodgkin lymphoma, osteosarcoma (high-dose regimens with leucovorin rescue)
Inflammatory / Non-oncologic
- Psoriasis (severe, recalcitrant) — FDA-approved 1972; considered the "gold standard" DMARD; ~45% of patients reach PASI-75 response; effective across all subtypes (plaque, guttate, pustular, erythrodermic)
- Psoriatic arthritis — first-line DMARD
- Rheumatoid arthritis — anchor DMARD; may be combined with biologics
- Crohn disease — effective SC for induction and maintenance (NOT effective in ulcerative colitis)
- Ectopic pregnancy (single/multi-dose IM protocol)
- Sarcoidosis (10–25 mg/week as steroid-sparing agent)
- Off-label: dermatomyositis, cutaneous lupus, pemphigus, lichen planus, atopic dermatitis, scleroderma, pyoderma gangrenosum
Dosing Summary
| Indication | Typical Dose |
|---|---|
| Psoriasis / PsA | 7.5–25 mg/week PO, IM, SC |
| Rheumatoid arthritis | 7.5–15 mg/week PO; up to 25 mg/week SC/IM |
| Malignancy (standard) | 25 mg/m² IV/IM 1–2×/week |
| High-dose oncology | 1–12 g/m² IV with leucovorin rescue |
| Ectopic pregnancy | 50 mg/m² IM (single-dose protocol) |
Adverse Effects
| System | Effect |
|---|---|
| Hematologic | Leukopenia, thrombocytopenia, anemia (bone marrow suppression) — most serious acute toxicity |
| GI | Nausea, vomiting, stomatitis, glossitis, mucositis, GI ulceration |
| Hepatic | Hepatotoxicity, hepatic fibrosis, cirrhosis (risk rises with cumulative dose >1.5–2 g; also with alcohol, preexisting liver disease) |
| Pulmonary | Methotrexate pneumonitis (hypersensitivity reaction); pulmonary fibrosis (rarer) |
| Renal | Tubular necrosis from MTX/7-OH-MTX precipitation in acidic urine; especially with high-dose IV |
| CNS | Intrathecal use: arachnoiditis, leukoencephalopathy, ↑ CSF pressure |
| Dermatologic | Urticaria, vasculitis, photosensitivity; can cause "radiation recall" |
| Teratogenicity | Category X — causes methotrexate embryopathy (multiple congenital anomalies if exposure during organogenesis at 6–8 weeks) |
Folate co-administration (1 mg/day folic acid) reduces GI and hematologic side effects without significantly reducing efficacy.
Monitoring
Baseline: CBC with differential, LFTs (AST, ALT, alkaline phosphatase), serum creatinine/BUN, urinalysis, chest X-ray, hepatitis B/C serology.
Ongoing:
- CBC and LFTs every 4–8 weeks during therapy
- Renal function monitoring (dose-adjust or hold if GFR falls)
- Liver biopsy consideration after cumulative dose >1.5 g (or procollagen-III peptide testing as alternative)
- Serum MTX levels mandatory with high-dose regimens; leucovorin doses adjusted to keep levels <50 nM post-rescue
| Condition | Target serum level |
|---|---|
| Psoriasis | <10 nM |
| High-dose oncology | Monitored with leucovorin rescue titrated to <50 nM |
Drug Interactions
| Drug | Interaction |
|---|---|
| NSAIDs / Aspirin | Displace MTX from albumin; reduce renal clearance → ↑ toxicity |
| Trimethoprim-sulfamethoxazole | Additive DHFR inhibition → severe pancytopenia |
| Probenecid | Blocks renal tubular secretion of MTX → ↑ levels |
| Penicillins | Reduce renal clearance |
| Alcohol | Potentiates hepatotoxicity |
| Folate antagonists (pyrimethamine, etc.) | Potentiate toxicity |
| Biologics (adalimumab, infliximab) | Combination used intentionally to reduce antidrug antibody formation |
Contraindications
- Pregnancy (absolute) — teratogenic/embryotoxic
- Breastfeeding
- Significant hepatic disease / alcoholism
- Severe renal impairment (GFR <30–40 mL/min)
- Pre-existing bone marrow suppression
- Active serious infections
- Immunodeficiency syndromes
Leucovorin Rescue
High-dose MTX protocols require leucovorin (folinic acid) rescue given 18–36 hours after MTX:
- Leucovorin is N⁵-formyl-FH₄ — it replenishes the tetrahydrofolate pool by bypassing the blocked DHFR enzyme
- Dose is titrated to serum MTX levels (target <50 nM)
- In suspected low-dose overdose, leucovorin should be given immediately
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 1224–1228 | Henry's Clinical Diagnosis & Management by Laboratory Methods, Table 24.7 | Fitzpatrick's Dermatology, Vol. 1–2, p. 3493 | Harrison's Principles of Internal Medicine 22E
This is a shared conversation. Sign in to Orris to start your own chat.