General examination for gi system in Peadeatrics for case presentation
Reading File
Finding Sources
Finding Sources
Searching the Web
general examination GI system pediatrics case presentation clinical findings
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Now I have enough information from multiple sources to compile a comprehensive, well-structured answer. Let me deliver the full response:
General Examination for the GI System in Paediatrics (Case Presentation)
The "general examination" component is performed before the abdominal examination and covers systemic signs that give clues about GI disease. Present findings in this sequence for a structured case presentation.
1. First Impressions (End of Bed)
- General appearance: Well/ill-looking, comfortable or in distress, alert or irritable
- Posture: Lying still (peritonitis), knees drawn up (colic/intussusception), restless (renal colic vs. peritonitis)
- Nutritional status: Thin/wasted (malabsorption, IBD, chronic liver disease), obese
- Growth: Note if the child appears small for age (failure to thrive is a key GI sign)
- Dysmorphic features: Down syndrome (duodenal atresia, Hirschsprung's), Turner syndrome
2. Vital Signs
| Parameter | GI Relevance |
|---|---|
| Temperature | Fever - infection, peritonitis, IBD |
| Pulse rate | Tachycardia - dehydration, hemorrhage, sepsis, pain |
| Blood pressure | Hypotension - significant dehydration, shock, hemorrhage |
| Respiratory rate | Tachypnea - metabolic acidosis (e.g., from diarrhea), peritonitis |
| Weight/Height | Malnutrition, failure to thrive, growth faltering |
3. Hydration Status (Particularly Important in Paediatrics)
Assess systematically:
- Eyes: Sunken (dehydration)
- Mouth/lips: Dry mucous membranes
- Skin: Reduced turgor (pinch test - abdomen or inner thigh)
- Anterior fontanelle (infants <18 months): Sunken = dehydration; Bulging = raised ICP (but can be seen in liver disease with raised ammonia)
- Capillary refill time: >2 seconds = poor perfusion
- Urine output: History of decreased wet nappies
Classify dehydration:
- Mild (<5%): Slightly dry mouth, normal eyes
- Moderate (5-10%): Sunken eyes, dry mucosa, reduced skin turgor, tachycardia
- Severe (>10%): All of above + sunken fontanelle, capillary refill >3 s, hypotension, lethargy
4. Hands
- Clubbing: Chronic liver disease (biliary atresia, cirrhosis), Crohn's disease, celiac disease
- Leukonychia (white nails): Hypoalbuminemia - liver disease, protein-losing enteropathy
- Koilonychia (spoon nails): Iron deficiency (celiac disease, GI blood loss)
- Palmar erythema: Chronic liver disease
- Dupuytren's contracture: Liver disease (less common in children)
- Tremor/asterixis (flapping tremor): Hepatic encephalopathy (test in older children)
- Peripheral cyanosis: Poor perfusion
5. Arms/Upper Limbs
- Scratch marks: Pruritus from cholestasis (biliary atresia, primary sclerosing cholangitis)
- Bruising: Coagulopathy from liver failure (decreased clotting factor synthesis)
- Spider naevi (>5 is significant): Chronic liver disease (>5 above the nipple line)
- IV access / lines: Note presence (already receiving treatment)
6. Face
- Eyes:
- Jaundice in sclerae (yellow sclera) - easiest site to detect jaundice early
- Pallor in conjunctivae - anemia (GI blood loss, malabsorption, chronic disease)
- Kayser-Fleischer rings (if suspected Wilson's disease - use slit lamp)
- Periorbital edema - hypoalbuminemia
- Parotid enlargement: Celiac disease, bulimia, malnutrition
- Facies: Cushingoid (steroid treatment for IBD), moon face
7. Mouth & Oral Cavity
"The oral cavity is the window to the GI system"
- Angular cheilitis (stomatitis): Iron, B12, or folate deficiency (celiac disease, IBD)
- Aphthous ulcers: Crohn's disease, celiac disease
- Tongue:
- Glossitis - B12/folate/iron deficiency
- Macroglossia - Beckwith-Wiedemann syndrome
- Teeth: Enamel erosion - GERD, bulimia
- Gum hypertrophy: Phenytoin (used for seizures in hepatic encephalopathy)
- Fetor hepaticus: Characteristic sweet musty breath of hepatic failure
- Halitosis: GERD, H. pylori
8. Neck
- Lymphadenopathy:
- Cervical nodes - mesenteric adenitis, lymphoma
- Virchow's node (left supraclavicular) - rarely in children, GI malignancy (older teens)
- JVD (jugular venous distension): Right heart failure causing hepatic congestion
9. Chest
- Spider naevi (count - >5 above nipple line is significant): Chronic liver disease
- Gynecomastia: Chronic liver disease (increased estrogen)
- Loss of axillary hair: Chronic liver disease
- Chest wall collateral veins: Portal hypertension
10. Skin (General)
| Finding | GI Association |
|---|---|
| Jaundice | Liver disease, biliary obstruction, hemolysis |
| Pallor | Anemia (GI blood loss, malabsorption) |
| Pigmentation (diffuse) | Addison's disease, celiac disease, hemochromatosis |
| Erythema nodosum | Crohn's disease, UC |
| Pyoderma gangrenosum | IBD (especially UC) |
| Dermatitis herpetiformis | Celiac disease (IgA-mediated) |
| Petechiae/purpura | Coagulopathy (liver failure), Henoch-Schonlein Purpura (GI involvement) |
| Xanthomas/xanthelasma | Chronic cholestasis |
| Acanthosis nigricans | Obesity, insulin resistance (NAFLD) |
11. Lower Limbs
- Pitting edema (ankle/sacral): Hypoalbuminemia (liver disease, protein-losing enteropathy, malnutrition)
- Peripheral neuropathy: B12 deficiency (celiac disease, terminal ileum disease in Crohn's)
- Wasted muscles: Chronic malnutrition, malabsorption
12. Anthropometric Assessment (Unique to Paediatrics)
Always include in GI case presentation:
- Weight and height: Plot on growth chart; note percentile/centile
- BMI for age: Overweight (NAFLD, GERD) or underweight (malabsorption, IBD)
- Weight-for-height/length: Wasting (acute malnutrition)
- Mid-upper arm circumference (MUAC): Useful in infants to assess nutritional status
- Head circumference (infants): Impact of chronic malnutrition on brain growth
- Serial weight charts: Downward crossing of centile lines = failure to thrive
Summary: Presenting the General Examination
For a case presentation, structure it as:
"On general examination, [patient name] is a [age]-year-old [sex] who appears [well/ill], is [comfortable/in distress], and is [appropriately/poorly] nourished. Growth parameters reveal a weight on the [Xth] centile and height on the [Xth] centile. Vitals: T [X]°C, HR [X], RR [X], BP [X], SpO2 [X]%. [He/She] appears [mildly/moderately/severely] dehydrated with [findings]. On examining the hands, there is [clubbing/pallor/koilonychia/nil]. The eyes show [jaundice/pallor/nil]. The mouth reveals [aphthous ulcers/angular cheilitis/nil]. There are [no/X] spider naevi. The skin shows [jaundice/erythema nodosum/nil]. The lower limbs show [pitting edema/nil]. I would like to proceed to the abdominal examination."
Key Paediatric-Specific Priorities:
- Hydration assessment is paramount (dehydration is rapidly life-threatening in children)
- Growth and nutritional status are core findings, not optional
- Skin manifestations of IBD and celiac disease are more commonly tested
- The oral cavity examination carries more weight in paediatric GI than in adult medicine
- Always plot growth parameters on a centile chart and comment on trajectory
Sources: Yamada's Textbook of Gastroenterology 7th Ed; S Das Manual on Clinical Surgery 13th Ed; The Harriet Lane Handbook 23rd Ed; Bailey & Love's Short Practice of Surgery 28th Ed
Abdomen examination in Peadeatrics
Finding Sources
Finding Sources
Searching the Web
abdominal examination pediatrics inspection palpation percussion auscultation clinical findings case presentation
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
I now have sufficient material from the textbooks combined with my clinical knowledge to deliver a complete, paediatrics-focused abdominal examination guide. Let me compile the full answer.
Abdominal Examination in Paediatrics (Case Presentation Format)
Preparation
Before starting, always:
- Position: Child lies flat and supine, arms at sides, legs extended. In infants, the caregiver may hold the child in a comfortable position or examine on the parent's lap to reduce crying (which causes tensing of abdominal muscles).
- Expose: Nipples to groin (include inguinal regions and genitalia).
- Warm hands before touching - cold hands cause involuntary guarding, especially in children.
- Approach from the child's right side.
- Gain trust first - talk to the child, let them see your hands, distract with a toy or light.
- Examine painful areas last.
- Sequence: Inspection → Auscultation → Percussion → Palpation (note: auscultation before percussion/palpation in the undisturbed abdomen).
STEP 1: INSPECTION
a) Surface Anatomy - Know Your Regions
The abdomen is divided into 9 regions by two horizontal and two vertical lines:
- Right hypochondrium | 2. Epigastrium | 3. Left hypochondrium
- Right lumbar | 5. Umbilical | 6. Left lumbar
- Right iliac fossa | 8. Hypogastrium | 9. Left iliac fossa
Alternatively, 4 quadrants (RUQ, LUQ, RLQ, LLQ) - simpler for presentation.
b) What to Inspect
Shape/Contour of the abdomen:
- Normal: Mildly protuberant (scaphoid) in infants and toddlers - this is NORMAL up to age ~3-4 years due to relatively large liver and weak abdominal muscles
- Distension (generalised): 6 Fs - Fat, Fluid (ascites), Flatus, Feces, Fetus (older adolescents), Fatal mass
- Central distension - small bowel obstruction
- Peripheral/flank distension - large bowel obstruction, ascites
- Massive distension filling whole abdomen - ascites, gross organomegaly
- Scaphoid (sunken): Severe malnutrition, dehydration
Skin:
- Jaundice (yellow tinge)
- Prominent/dilated veins:
- Caput medusae (radiating from umbilicus) = portal hypertension (recanalized umbilical vein)
- Caval obstruction pattern = veins run upward above umbilicus, downward below
- Grey-Turner's sign (flank ecchymosis) - hemorrhagic pancreatitis
- Cullen's sign (periumbilical ecchymosis) - retroperitoneal hemorrhage
- Striae - rapid weight gain/loss, Cushing's syndrome
- Rashes: Henoch-Schonlein Purpura (palpable purpura over buttocks/lower limbs, may have GI involvement)
Umbilicus:
- Position (normally central; displaced by masses)
- Everted - ascites, large mass
- Umbilical hernia - common in neonates/infants; note size of defect
- Inflamed/discharge - omphalitis (neonates)
- Patent vitello-intestinal duct - fecal discharge from umbilicus
Respiratory movements:
- Normally the abdomen moves with breathing (abdominal breathing predominates in children)
- Absent/restricted movement = peritonitis ("board-like" rigidity, child lies still and avoids movement)
- Localised restriction = underlying local peritoneal irritation (appendicitis, cholecystitis)
Visible peristalsis:
- "Ladder pattern" = small bowel obstruction
- Left-to-right peristalsis in epigastrium = pyloric stenosis (classic - seen best after feeding, in a hungry infant)
- Pathological in children; never present in a normal abdomen
Visible masses/swellings:
- Describe: region, size, shape, whether it moves with respiration
- Note hernial sites: umbilical, inguinal, femoral (check for impulse on coughing/crying)
Genitalia (always include in paediatric examination):
- Inguinal hernias, hydroceles, undescended testes in boys
- Labial masses in girls
STEP 2: AUSCULTATION
Always before percussion and palpation to avoid altering bowel sounds.
Bowel sounds:
- Listen in the right iliac fossa (ileocaecal valve - best site)
- Listen for at least 15-20 seconds before declaring absent
| Finding | Interpretation |
|---|---|
| Normal (gurgling, 5-35/min) | Normal gut motility |
| High-pitched, tinkling, rushing | Intestinal obstruction (synchronous with colicky pain) |
| Absent bowel sounds (silent abdomen) | Paralytic ileus, peritonitis, late obstruction |
| Hyperactive | Gastroenteritis, early obstruction |
Bruits:
- Aortic bruit (epigastrium/umbilicus) - vascular malformation, renal artery stenosis
- Hepatic bruit - hepatocellular carcinoma, acute alcoholic hepatitis (rare in children), AV malformation of liver
Venous hum:
- Over epigastrium/umbilicus = portal hypertension (Cruveilhier-Baumgarten syndrome - recanalized umbilical vein)
Hepatic friction rub:
- Over RUQ = hepatic abscess, perihepatic inflammation
STEP 3: PERCUSSION
General Percussion
Technique: Use middle finger of non-dominant hand placed flat, percuss with tip of dominant middle finger. Use gentle, light percussion - children are more sensitive.
Tympany vs. Dullness:
- Tympany = air-filled bowel (normal over most of abdomen)
- Dullness = solid organ or fluid
Specific Percussion Points in Paediatrics
Liver:
- Percuss the upper border from the right midclavicular line (MCL) downward from the chest - normally dull from the 5th intercostal space
- Percuss the lower border upward from below the umbilicus
- Liver span (at MCL):
- Neonate: 4-5 cm
- 1 year: 5-6 cm
- 5 years: 6-7 cm
- 10 years: 7-9 cm
- Adult: 6-12 cm
- Liver dullness obliterated = perforation of hollow viscus (free air under diaphragm)
- Raised upper border = subphrenic abscess, liver abscess, hepatomegaly
Spleen:
- Percuss in left midaxillary line between the 9th and 11th ribs
- Normally resonant (splenic dullness only if enlarged)
- Traube's space (normally tympanic): Left lower anterior chest bordered by diaphragm above, midaxillary line laterally, left costal margin below - dullness = splenomegaly or fluid (full stomach)
Ascites - Shifting Dullness (most reliable clinical test):
Technique:
- Percuss from umbilicus toward right flank - note where tympany changes to dullness
- Keep finger at that point, ask child to roll toward you (left lateral position)
- Wait 15-30 seconds for fluid to redistribute
- Percuss same point again - if now tympanic, shifting dullness = positive (ascites confirmed)
- Repeat on both sides
Note: Shifting dullness is present but may be difficult to elicit in small children - need at least 500 mL fluid in adults (less in children due to smaller abdomen).
Fluid Thrill (for massive ascites):
- Helper places the medial edge of their hand/wrist firmly along the midline (prevents transmission through abdominal wall)
- Examiner flicks/taps one flank sharply
- A thrill (impulse) felt on the opposite flank = positive fluid thrill = massive ascites
Bladder:
- Percuss suprapubically - dull if distended (urinary retention, neurogenic bladder)
Kidneys:
- Renal swelling is resonant (colon overlies) - differentiates from liver/spleen dullness
- Exception: massively enlarged kidney may be dull when colon is displaced
STEP 4: PALPATION
General Principles in Children
- Warm hands, approach slowly, use flat of the hand (not fingertips)
- Start furthest from the area of pain
- Ask child "where does it hurt?" and start in the opposite quadrant
- Watch the child's face, not your hands - look for grimacing
- Superficial palpation first (light pressure, ~1 cm depth), then deep palpation (4-5 cm depth)
- Use a distracting technique: "breathe in and out through your mouth"
- In an uncooperative infant, palpate during sleep or use a pacifier/feeding
A) Superficial (Light) Palpation
- Tenderness: Note site, severity (does child wince/pull away/guard?)
- Guarding:
- Voluntary guarding - child tenses muscles on your approach; relaxes during expiration; due to fear/ticklishness
- Involuntary/Reflex guarding (muscle rigidity) - persists even during expiration; indicates underlying parietal peritoneal irritation; more sinister
- Board-like rigidity: Extreme involuntary rigidity = generalised peritonitis (surgical emergency)
- Masses: Note any obvious superficial swelling
B) Deep Palpation
Liver:
- Start in the right iliac fossa (so you don't miss a massively enlarged liver) and move upward
- Place hand flat, ask child to breathe in - feel for liver edge descending on inspiration
- Normal: In infants up to 2 cm below right costal margin is normal (liver is relatively larger in children)
- Report: Size in cm below right costal margin (RCM) in the MCL
| Liver edge characteristics | Interpretation |
|---|---|
| Smooth, soft, slightly tender | Hepatitis (viral, metabolic), heart failure, early congestion |
| Smooth, firm, non-tender | Normal, early cirrhosis |
| Hard, irregular, nodular | Cirrhosis, malignancy (hepatoblastoma, metastases) |
| Tender, enlarged | Hepatitis, abscess, liver congestion (right heart failure) |
| Pulsatile | Tricuspid regurgitation |
- Note if liver moves with respiration (liver, gallbladder, stomach, spleen move well with respiration)
Spleen:
- Start in the right iliac fossa (can miss a massively enlarged spleen if you start near the left costal margin)
- Move diagonally toward the left costal margin, asking child to breathe in
- Feel for a notched medial edge descending on inspiration
- The spleen enlarges toward the right iliac fossa in direction of the right iliac fossa
- Report: Size in cm below left costal margin in the MCL
- Differentiate spleen from left kidney:
- Spleen: Cannot get above it, notch palpable on medial edge, moves diagonally with respiration, dull to percussion, not ballotable
- Kidney: Can get above it, no notch, moves vertically, resonant (colon in front), ballotable (bimanual)
Kidneys (Bimanual/Ballottement):
- Left hand behind loin, right hand anteriorly
- Push up with posterior hand - feel kidney "float up" to anterior hand
- Ballottement: Quick upward push posteriorly - kidney bounces against anterior hand
- Normal: Not palpable in children >5 years; may be felt in neonates/infants (normal)
- If enlarged: Measure size, note surface, tenderness
Spleen vs. Kidney - Key Distinguishing Features:
| Feature | Spleen | Kidney |
|---|---|---|
| Upper margin palpable? | No | Yes (can "get above") |
| Notch | Yes (medial) | No |
| Movement | Diagonal (toward RIF) | Vertical |
| Percussion | Dull | Resonant (colon in front) |
| Ballottable | No | Yes |
| Bimanual palpable | No | Yes |
Gallbladder:
- Palpable at tip of right 9th costal cartilage (intersection of MCL and costal margin)
- Murphy's sign: Press at gallbladder point and ask child to take a deep breath - sharp pain/arrest of inspiration = positive = acute cholecystitis
Urinary Bladder:
- Palpable as a smooth, rounded, dull suprapubic mass when distended
Other Masses:
Describe any mass in terms of:
- Site (which region?)
- Size (cm, two dimensions)
- Shape
- Surface (smooth/nodular/irregular)
- Consistency (soft/firm/hard/cystic)
- Edge (well-defined/ill-defined)
- Tenderness
- Movement with respiration (yes/no)
- Mobility (in which direction?)
- Pulsatility (transmitted vs. expansile)
- Plane (superficial vs. deep to abdominal wall - ask child to raise head/tense muscles)
C) Special Tests
Rovsing's Sign (appendicitis):
- Palpate left iliac fossa - pain referred to right iliac fossa = positive = peritoneal irritation at appendix
Psoas Sign (retrocaecal appendicitis):
- With child lying on left side, extend the right hip - pain in RIF = inflamed appendix lying on psoas
Obturator Sign (pelvic appendicitis):
- Flex right hip and knee, then internally rotate hip - pain in RIF/hypogastrium = positive
Rebound Tenderness (Blumberg's Sign):
- Deep pressure then sudden release causes sharp pain = peritoneal irritation
- Note: Not recommended as a routine test in children - painful and distressing. Percussion tenderness is preferred.
Guarding vs. Rigidity: Already described above.
STEP 5: SPECIAL PAEDIATRIC EXAMINATIONS
Pyloric Stenosis (Infants, ~3-8 weeks)
- Position: Examine during or just after a feed
- Palpate in the epigastrium - feel for olive-shaped mass (hypertrophied pylorus) just to the right of midline
- Watch for visible gastric peristalsis (left to right across epigastrium)
Intussusception (~3 months - 2 years)
- Dance's sign: Empty right iliac fossa (intussusceptum has moved away)
- Sausage-shaped mass may be felt in RUQ or across the upper abdomen
- PR: Currant jelly stools (blood and mucus) on examination glove
Hirschsprung's Disease (Neonates/Infants)
- Abdominal distension
- PR: Explosive discharge of gas and stool on rectal examination (squirt sign)
STEP 6: DIGITAL RECTAL EXAMINATION (DRE)
Always mention this in case presentation - even if not performed clinically:
"I would like to complete the abdominal examination with a digital rectal examination, with appropriate consent and a chaperone present."
Indications in paediatrics:
- Constipation (assess for fecal loading, anal tone, rectal mass)
- GI bleeding (note blood on glove, test for occult blood)
- Hirschsprung's (squirt sign)
- Suspected intussusception (currant jelly stool)
- Suspected pelvic mass
STEP 7: COMPLETE THE EXAMINATION
Always state you would also examine/request:
- Hernial orifices (inguinal, femoral, umbilical) - always inspect and palpate
- External genitalia (undescended testes, inguinal hernia, hydrocele)
- Spine (vertebral tenderness, scoliosis affecting abdominal presentation)
- Growth chart (plot current weight and height)
- Urine dipstick
- Stool examination if indicated
HOW TO PRESENT THE ABDOMINAL EXAMINATION
"On abdominal examination, the abdomen was [flat/mildly protuberant/distended/scaphoid], moving with respiration. There were no visible masses, dilated veins, or visible peristalsis. The umbilicus was [central/everted/inverted]. On auscultation, bowel sounds were [present and normal/increased/decreased/absent]. There were no bruits or rubs heard.On percussion, there was no shifting dullness or fluid thrill to suggest ascites. Liver dullness was preserved. On palpation, the abdomen was [soft/firm], [non-tender/tender over X region]. There was [no/mild/moderate] voluntary guarding and [no/involuntary] rigidity. The liver was palpable [X cm below the right costal margin / not palpable], with a [smooth/irregular/nodular] edge. The spleen was [not palpable / palpable X cm below the left costal margin]. Both kidneys were not ballotable. No other masses were felt. Hernial orifices were intact with no impulse on coughing. I would like to complete the examination with a digital rectal examination."
Sources: S Das Manual on Clinical Surgery 13th Ed; Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology 7th Ed; Bailey & Love's Short Practice of Surgery 28th Ed
Amoebic Liver in Peadeatrics
Reading File
Finding Sources
Finding Sources
Searching PubMed
"amoebic liver abscess" AND child
Searching the Web
amoebic liver abscess pediatrics children clinical features diagnosis treatment metronidazole
Reading File
Finding Sources
Searching PubMed
"amoebic liver abscess" AND pediatric
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Excellent - I now have all the content needed from textbooks, Red Book (paediatric authority), and clinical sources. Let me now deliver the comprehensive answer.
Amoebic Liver Abscess (ALA) in Paediatrics
Definition
Amoebic Liver Abscess (ALA) is the most common extraintestinal manifestation of infection by Entamoeba histolytica, caused by haematogenous spread of trophozoites from the colon to the liver via the portal circulation, resulting in liquefactive necrosis of hepatic parenchyma.
Epidemiology
- Caused by Entamoeba histolytica - the most common pathogenic amoeba in humans
- Worldwide distribution, highest in tropical/subtropical endemic zones: Indian subcontinent, Sub-Saharan Africa, Central and South America, South East Asia
- Prevalence of E. histolytica in stool in endemic zones averages 10%; ALA incidence can be as high as 21 per 100,000 population
- In endemic areas, prevalence of amebic infection in some communities can reach 50%
- Age in children: ALA is uncommon in children under 3 years but well-recognised in school-age children in endemic areas
- Sex predominance: In adults, invasive disease (especially ALA) is significantly higher in adult males; in children, this sex predominance is less pronounced but males are still more commonly affected
- Disease is more severe in: the very young, malnourished, pregnant women, and those on corticosteroids (immunosuppressed)
- Majority of infected individuals are asymptomatic carriers
Aetiology & Organism
| Feature | Detail |
|---|---|
| Causative organism | Entamoeba histolytica |
| Infectious form | Cyst (infective), Trophozoite (invasive/pathogenic) |
| Route of infection | Faecal-oral (contaminated food/water) |
| Survival of cysts | Weeks to months in environment; resistant to chlorine; single cyst sufficient to cause disease |
| Incubation period | Variable; commonly 2-4 weeks (range: days to months/years) |
| Related non-pathogenic species | E. dispar, E. coli (morphologically identical, do NOT require treatment) |
Life Cycle & Pathogenesis
Ingestion of cysts (contaminated food/water)
↓
Excystation in alkaline small intestine
↓
Trophozoites released → colon
↓
Trophozoites invade colonic submucosa
→ Flask-shaped ulcers in large bowel
↓
Trophozoites enter portal circulation
↓
Trapped in interlobular veins of liver
↓
Multiply in portal triads
→ Focal infarction of hepatocytes
→ Liquefactive necrosis (proteolytic enzymes)
↓
Areas of necrosis coalesce
→ ABSCESS CAVITY
Abscess contents: "Anchovy sauce" or "chocolate-coloured" fluid - a sterile, odourless mixture of necrotic liver tissue and blood. Pus smells only if secondarily infected.
Trophozoites are found in the abscess wall (not the pus) in a minority of cases.
Location of Abscess
| Location | Frequency |
|---|---|
| Right lobe | 80% (most common - straight course of superior mesenteric blood flow) |
| Left lobe | 10% (higher clinical significance - risk of pericardial rupture) |
| Multiple | 10% |
| Diaphragmatic surface of right lobe | Most common specific site - explains pulmonary symptoms |
Clinical Features
A. Symptoms
Early / Non-specific (Insidious onset):
- Fever (most consistent feature - often high grade, swinging/remittent)
- Malaise, lethargy
- Anorexia and weight loss
- Night sweats
- Non-productive cough
- Hiccoughs (diaphragmatic irritation)
Later / More Specific:
- Right upper quadrant (RUQ) pain - aching or pleuritic in nature
- Right shoulder tip pain (referred via phrenic nerve - C3, C4, C5)
- Progressive hepatomegaly with tenderness
Intestinal symptoms (often absent in ALA):
- Bloody mucoid diarrhoea (present in only minority; evidence of recent/concurrent intestinal infection usually absent in extraintestinal disease)
- History of travel to endemic area raises suspicion significantly
B. Signs on Examination
General:
- Toxic, ill-looking child
- Pallor (anaemia)
- Low-grade to high-grade fever
- Tachycardia
- Mild jaundice (occasional, from biliary obstruction or haemolysis)
- Weight loss, malnutrition (chronic cases)
Abdominal:
- Tender hepatomegaly - liver edge firm, smooth, tender; the single most consistent sign
- Right upper abdominal rigidity/guarding (involuntary)
- Tender, bulging intercostal spaces on the right (stretching of liver capsule)
- Overlying skin oedema (right chest wall)
- Rarely, ascites
Chest:
- Right-sided pleural effusion (reactive or from direct extension)
- Basal pneumonitis (late feature, right side)
- Decreased breath sounds right base
- Raised right hemidiaphragm
"The typical patient has upper abdominal rigidity, tender hepatomegaly, often with tender and bulging intercostal spaces and overlying skin oedema, a pleural effusion and basal pneumonitis." - Bailey & Love's Surgery
Complications
Rupture of Abscess (Most serious complication)
| Site of Rupture | Consequence | Features |
|---|---|---|
| Pleural cavity (most common) | Empyema thoracis | Sudden pleuritic chest pain, respiratory distress - right side in 86% |
| Peritoneal cavity | Peritonitis | Sudden severe abdominal pain, board-like rigidity, shock |
| Pericardial cavity | Pericarditis/tamponade | From left lobe abscess; most lethal complication |
| Lung (bronchial) | Hepatobronchial fistula | Cough productive of "chocolate sauce" sputum |
| Skin | Cutaneous fistula | Rare |
| Brain | Cerebral amoebiasis | Haematogenous spread; rare but fatal |
Left lobe abscess - always drains more aggressively due to proximity to pericardium.
Other Complications
- Secondary bacterial infection of abscess (pus then smells)
- Jaundice (biliary compression)
- Portal hypertension (chronic)
- Amoeboma (granuloma in colon - caecum most common, can mimic carcinoma)
- Toxic megacolon, colonic perforation (intestinal complications)
Investigations
Haematology & Biochemistry
| Test | Findings |
|---|---|
| FBC | Leucocytosis (neutrophilia), anaemia (normochromic normocytic) |
| ESR | Elevated |
| CRP | Elevated |
| Liver function tests | Elevated alkaline phosphatase (most consistent), mildly elevated transaminases, hypoalbuminaemia |
| Bilirubin | Usually normal; mildly elevated in complicated cases |
| PT/INR | May be prolonged in severe hepatic involvement |
Serology (Specific Tests)
| Test | Notes |
|---|---|
| ELISA | Test of choice - detects anti-E. histolytica antibodies; highly sensitive and specific |
| Indirect Haemagglutination (IHA) | Very high sensitivity in non-endemic areas; elevated even after treatment |
| Indirect Immunofluorescence | Available |
| Complement Fixation Test | Older test |
| Important caveat | Serology unreliable in endemic areas (persistent antibodies in population from prior exposure; high background positivity) |
| Antigen detection (ELISA stool/serum) | Differentiates E. histolytica from non-pathogenic E. dispar |
| PCR (stool/abscess) | Highest sensitivity and specificity; can differentiate species; FDA-approved multiplex PCR panels now being used |
Stool Examination
- Microscopy: trophozoites or cysts (low sensitivity; doesn't differentiate species)
- Stool PCR: preferred when available
- Note: concurrent intestinal infection often absent in ALA
Imaging
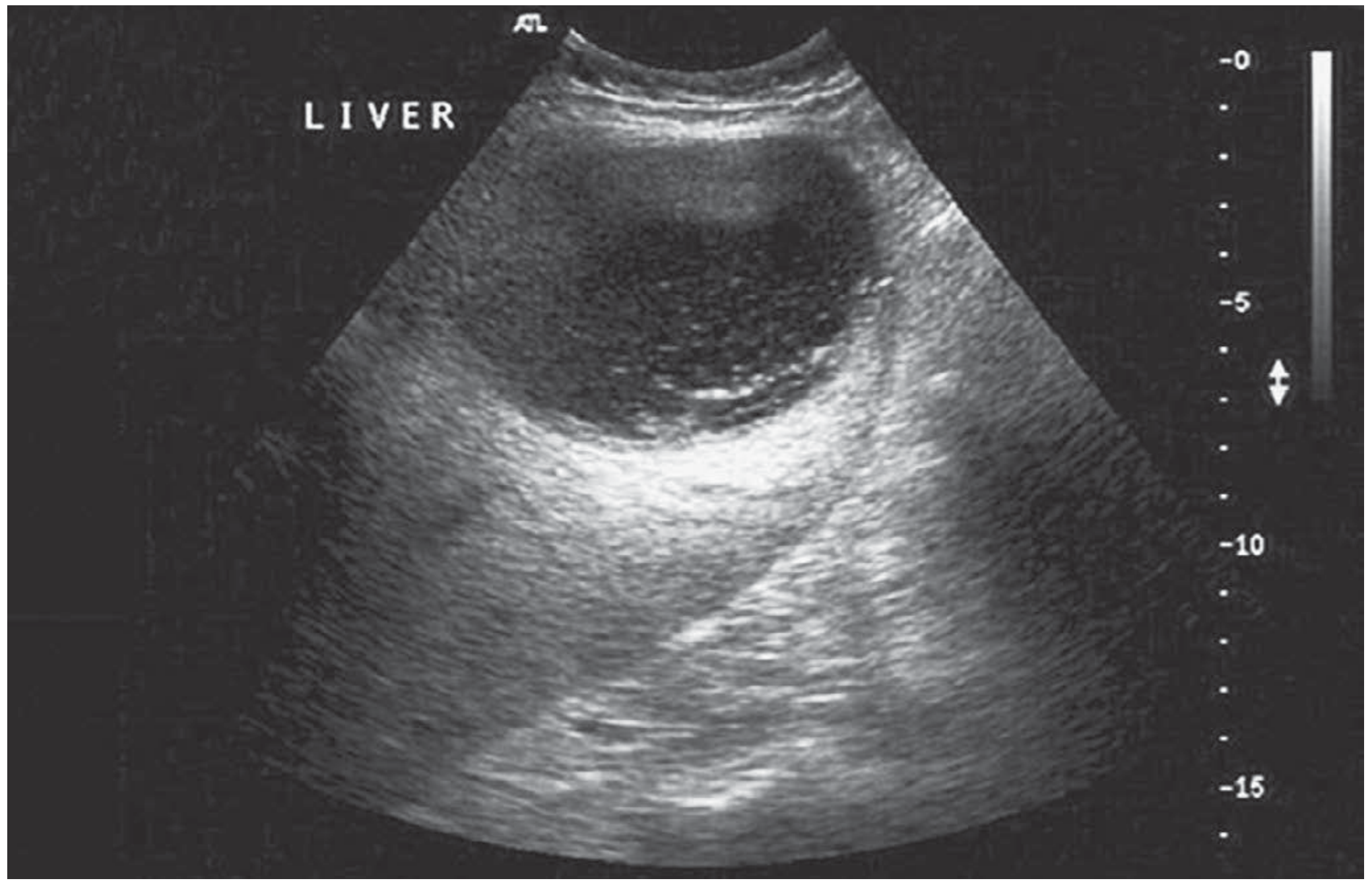
Ultrasound (USG) - First-line investigation:
- Hypoechoic or anechoic lesion with ill-defined borders
- Internal echoes suggest necrotic debris
- Used to guide aspiration (diagnostic and therapeutic)
- Raised right hemidiaphragm
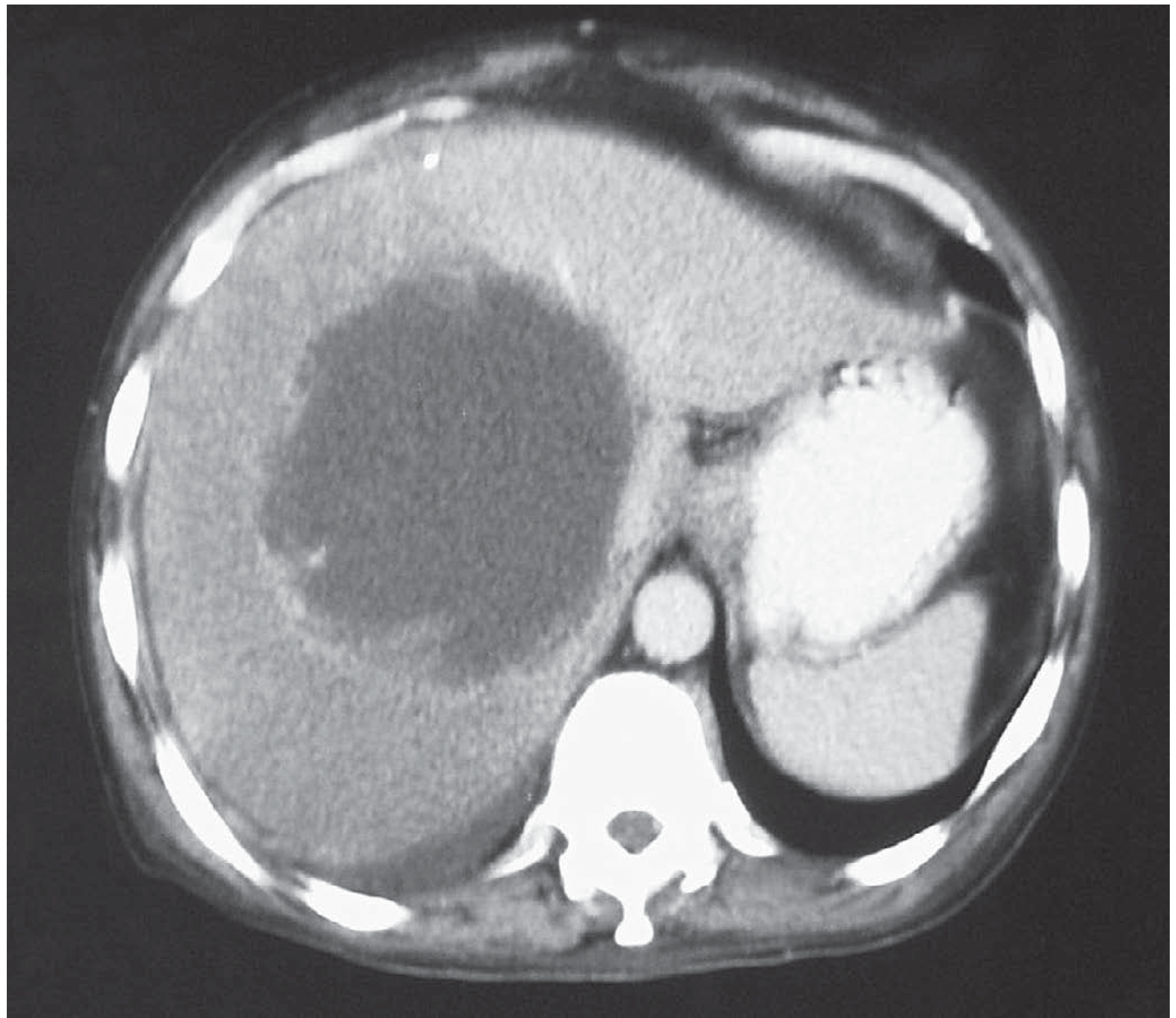
CT Scan (when diagnosis in doubt):
- Hypodense lesion, well-defined rim-enhancing wall on contrast
- Confirms diagnosis, shows size, relationship to structures
- Shows raised right hemidiaphragm, pleural effusion, pulmonary infiltrates
- Better than USG for multiple abscesses and complications
Chest X-ray:
- Elevated right hemidiaphragm
- Right basal consolidation/collapse
- Right pleural effusion
Diagnostic aspiration:
- Limited value for diagnosis
- Useful to confirm "anchovy sauce" (chocolate-coloured, sterile, odourless) aspirate
- Culture usually negative (sterile abscess unless secondarily infected)
Differential Diagnosis
| Condition | Differentiating Feature |
|---|---|
| Pyogenic liver abscess | Multiple, smaller lesions; bacterial culture positive; no travel history; fever more acute; no anchovy sauce aspirate |
| Hydatid cyst | Cystic, daughter cysts on imaging; Casoni test; serology for Echinococcus |
| Hepatocellular carcinoma | AFP elevated; no fever; firm irregular mass |
| Hepatitis (viral/bacterial) | Diffuse hepatomegaly; transaminases markedly elevated; no cavity on imaging |
| Subphrenic abscess | Post-surgical; above diaphragm; no hepatic cavity |
| Right basal pneumonia | Chest signs predominate; no hepatic lesion on imaging |
| Amoeboma (caecal) | Caecal mass; RIF; no hepatic lesion |
Treatment
Step 1: Tissue Amebicide (Anti-invasive - Kills Trophozoites in Liver)
Metronidazole - Drug of choice
| Patient | Dose |
|---|---|
| Children | 35-50 mg/kg/day in 3 divided doses orally/IV × 7-10 days |
| Adults | 750 mg TDS × 10 days |
| Cure rate | ~90% of uncomplicated ALA |
Tinidazole - Alternative (better tolerated, fewer side effects, shorter course)
- Children: 50-60 mg/kg/day × 5 days (max 2g/day)
- Advantage: once daily dosing, shorter course
Other tissue amebicides (less used now):
- Chloroquine (active only in liver)
- Dehydroemetine / Emetine (cardiotoxic, rarely used)
Step 2: Luminal Amebicide (Eradicates Intestinal Cysts - Prevents Relapse)
ALWAYS follow tissue amebicide with luminal agent to eradicate intestinal reservoir.
- Diloxanide furoate (not effective against hepatic infection; luminal only): 20 mg/kg/day TDS × 10 days
- Paromomycin: 25-35 mg/kg/day TDS × 7 days (alternative)
- Iodoquinol: 30-40 mg/kg/day TDS × 20 days
Step 3: Aspiration / Drainage (Selected Cases)
Medical treatment alone is successful in most cases. Aspiration is indicated when:
- Risk of rupture - abscess >5 cm in diameter
- Left lobe abscess - proximity to pericardium, higher mortality risk
- No clinical response to metronidazole within 5-7 days
- Cannot differentiate from pyogenic abscess (secondarily infected ALA)
- Large symptomatic abscess causing significant distress
- Immunocompromised child
Method: Percutaneous ultrasound-guided aspiration or pigtail catheter drainage. The aspirated "chocolate sauce" confirms diagnosis.
"In most cases of liver abscess, drainage is not required and does not speed recovery. Patients typically improve symptomatically within days, but it may take months for a liver abscess to resolve on ultrasonography." - Red Book 2021 (Johns Hopkins / AAP)
Step 4: Surgery
Reserved for complications only:
| Complication | Surgical Management |
|---|---|
| Rupture into pleural cavity | Resuscitation + pleural drainage + lavage + metronidazole |
| Rupture into peritoneal cavity | Resuscitation + exploratory laparotomy + peritoneal lavage + drainage |
| Pericardial rupture/tamponade | Emergency pericardiocentesis/pericardial window |
| Secondary infection unresponsive | Open surgical drainage |
| Toxic megacolon (intestinal complication) | Subtotal colectomy + terminal ileostomy + rectal stump closure |
Paediatric-Specific Points
- More severe disease in the very young and malnourished children - early diagnosis critical
- Nutritional rehabilitation is important alongside antimicrobial treatment
- Household contacts should have stool examination and treatment if positive
- Children with ALA should not return to school/swimming until luminal treatment complete and diarrhoea resolved
- Corticosteroids (if given for misdiagnosed IBD) can catastrophically worsen amoebic colitis - always exclude E. histolytica before starting steroids for suspected IBD in endemic areas
- PCR multiplex panels (e.g., gastrointestinal panels) are increasingly used for paediatric diagnosis - a 2025 paediatric series (PMID: 41164783) showed utility even for off-label stool PCR diagnosis of ALA
- Follow-up imaging: Resolution of abscess cavity on USG can take weeks to months - do not repeat antibiotics based on imaging alone if child is clinically well
Prognosis
- Uncomplicated ALA treated promptly: excellent prognosis, near 100% recovery
- Complicated ALA (rupture, especially pericardial): mortality significant - fatal cases reported even with treatment
- With metronidazole: cure in ~87-90% of uncomplicated cases
- Abscess cavity may take months to fully resolve on imaging despite clinical cure
- Follow-up stool examination recommended after treatment (no regimen completely eradicates intestinal infection)
Control Measures
- Hand hygiene after defecation
- Safe water (boiling/filtration - chlorine resistance means standard chlorination insufficient)
- Sanitary disposal of faecal material
- Avoid raw vegetables/fruits washed in contaminated water in endemic areas
- Sexual transmission: condom use; avoid activity with those recovering from diarrhoea
- Treat asymptomatic cyst excretors (household contacts)
Sources: Bailey & Love's Short Practice of Surgery 28th Ed; Red Book 2021 - Report of the Committee on Infectious Diseases (AAP/Johns Hopkins Hospital); Goldman-Cecil Medicine; Yamada's Textbook of Gastroenterology 7th Ed; PubMed PMID: 37703554, 41164783
This is a shared conversation. Sign in to Orris to start your own chat.