Hormonal control of menstrual cycle
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Reading File
I now have everything needed for a thorough, well-illustrated answer. Let me compile it.
Hormonal Control of the Menstrual Cycle
The menstrual cycle is a precisely orchestrated interplay between the hypothalamus, the anterior pituitary, and the ovaries - the hypothalamic-pituitary-ovarian (HPO) axis - with the uterine endometrium as the end-organ target. A typical cycle spans 21-35 days (average 28 days). Variability between women is almost entirely due to variability in the follicular phase; the luteal phase is nearly constant at 14 days.
The HPO Axis: Overview
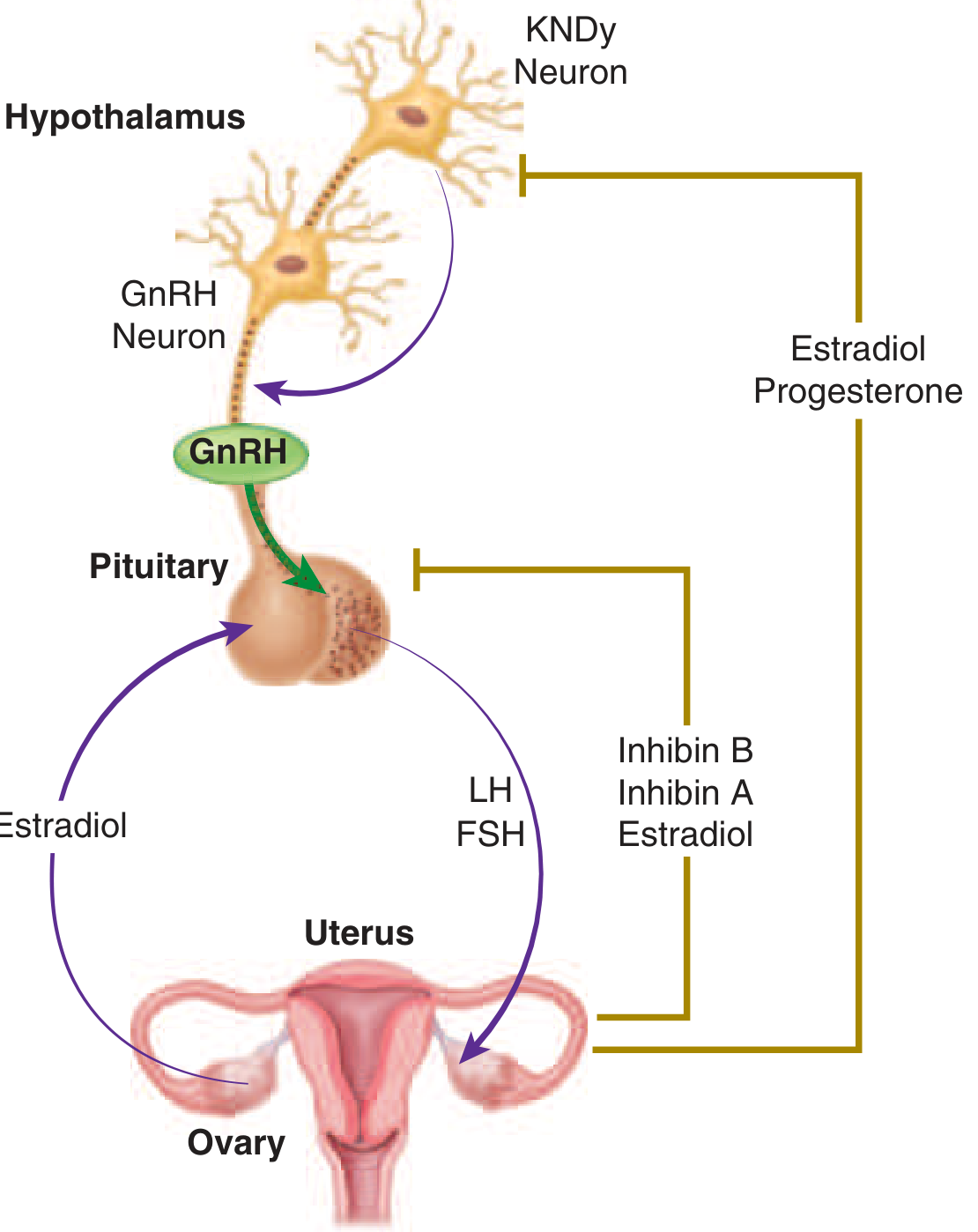
The reproductive system is critically dependent on both negative and positive feedback loops. GnRH pulses drive pituitary gonadotropin release, while gonadal steroids and inhibins feed back to control cycle dynamics - Harrison's Principles of Internal Medicine 22E, p. 3172
The cycle is regulated through a series of negative and positive feedback loops that alter:
- Pulsatile GnRH secretion from the hypothalamic arcuate nucleus
- Pituitary response to GnRH (synthesis and release of LH and FSH)
- Relative secretion of LH vs. FSH
Key principle: slow GnRH pulse frequencies favor FSH synthesis; high frequencies favor LH synthesis. FSH synthesis is further modulated by the activin-inhibin-follistatin system within pituitary folliculostellate cells.
Hormone Dynamics Across the Cycle
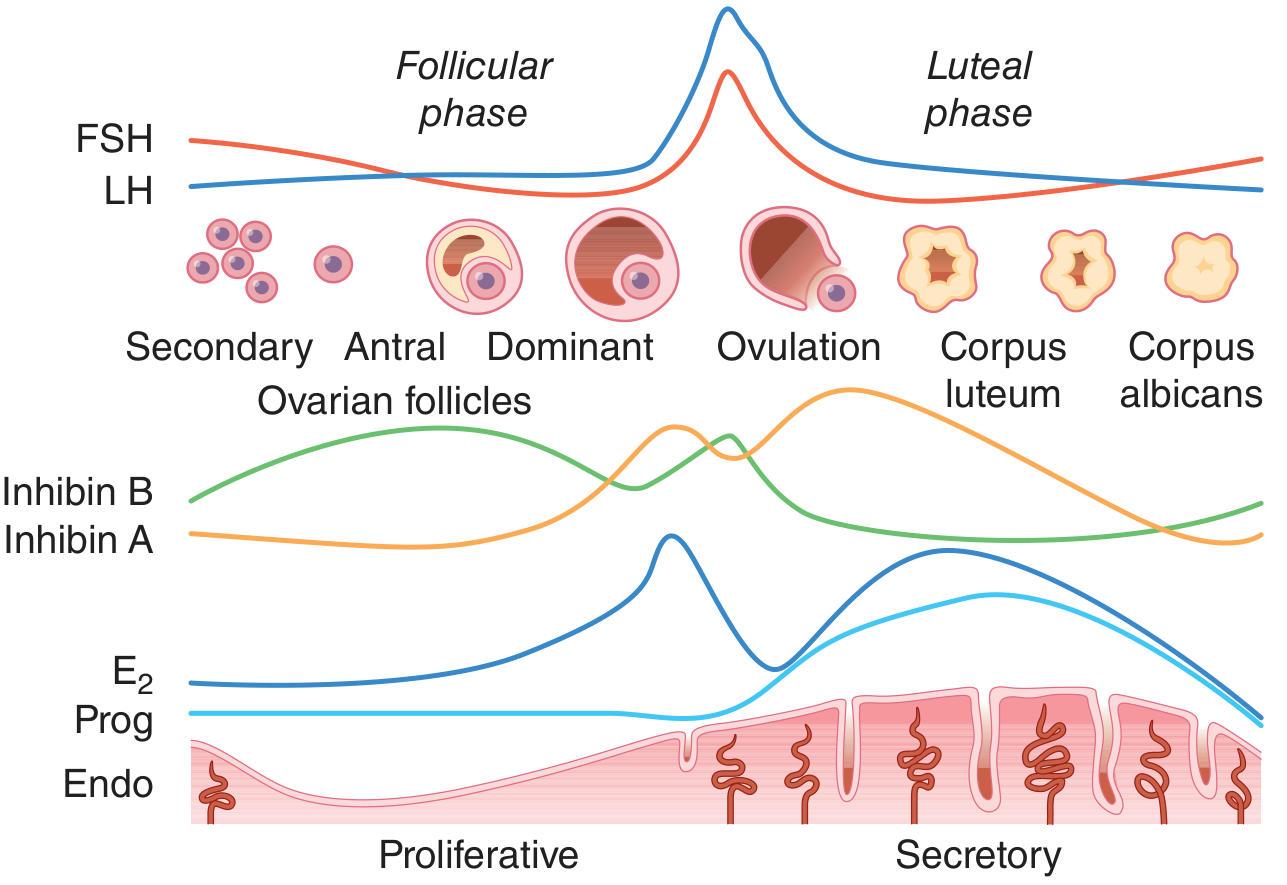
Relationship between gonadotropins, follicle development, gonadal secretion, and endometrial changes during the normal menstrual cycle. - Harrison's Principles 22E, Fig. 404-8
Phase 1: Follicular Phase (Days 1-14)
Initiation - the FSH Rise
The follicular phase begins on day 1 of menstruation, but follicle recruitment is actually triggered in the late luteal phase of the prior cycle as the corpus luteum regresses. Falling progesterone, estradiol, and inhibin A remove negative feedback, allowing an approximately 20% rise in FSH. This modest FSH elevation is sufficient to recruit a cohort of secondary follicles, reflecting the marked sensitivity of resting follicles to FSH.
The Two-Cell, Two-Gonadotropin Model
Follicular steroidogenesis depends on coordinated action of both gonadotropins:
- LH acts on theca cells to stimulate androgen (androstenedione, testosterone) production
- FSH acts on granulosa cells to induce aromatase, converting androgens to estradiol (E2)
This is the "two-cell, two-gonadotropin" theory of estrogen biosynthesis.
Dominant Follicle Selection
As the cohort of follicles grows, they secrete rising estradiol and inhibin B. These together exert negative feedback on pituitary FSH secretion, causing FSH to fall by mid-follicular phase. The follicle destined to ovulate - the dominant follicle - has more FSH receptors and produces more estrogen than its neighbors, allowing it to survive the FSH decline while other follicles undergo atresia.
Late Follicular Phase
The exponential rise in estradiol causes two simultaneous events:
- Continued negative feedback suppression of FSH (and initially LH)
- At a threshold of sustained high estradiol, a switch to positive feedback at the pituitary, upregulating GnRH receptors and gonadotrope responsiveness
FSH-induced LH receptors appear on granulosa cells, and low levels of progesterone and 17-hydroxyprogesterone begin to be secreted by the preovulatory follicle.
Endometrial effect: Rising estradiol drives proliferative changes in the endometrium - growth of glands and stroma, elongation of spiral arteries, and thin watery "ferning" cervical mucus that allows sperm penetration.
Phase 2: Ovulation (Day ~14)
The sustained estradiol surge triggers the LH surge (and a smaller FSH surge), the proximate cause of ovulation. Key timing:
- The LH surge precedes follicle rupture by 24-36 hours
- During this window: the oocyte uncouples from granulosa cells, genes for inflammation and tissue remodeling are induced, and final oocyte maturation (completion of meiosis I) occurs
Low progesterone secreted from the peri-ovulatory follicle contributes to the timing of the surge, though it is not required to generate it. Hypothalamic GnRH secretion plays a permissive role in generating the preovulatory surge in humans (unlike rodents, where a GnRH surge also occurs).
At ovulation, cervical mucus peaks in quantity and becomes maximally watery and sperm-penetrable.
Phase 3: Luteal Phase (Days 14-28)
Corpus Luteum Formation
The ruptured follicle transforms into the corpus luteum, which secretes:
- Progesterone (dominant hormone)
- 17-hydroxyprogesterone
- Inhibin A
- Estradiol (via continued aromatization of theca-derived androgens by luteinized granulosa cells)
- Relaxin
Endometrial Effects
The combined action of progesterone and estrogen produces secretory transformation of the endometrium:
- Glands become tortuous and glycogen-filled
- Stroma becomes edematous
- Spiral arteries elongate and coil further
- Cervical mucus becomes thick, non-elastic, and non-ferning (hostile to sperm)
- Basal body temperature rises (~0.2-0.5°C) due to progesterone's thermogenic effect on the hypothalamic temperature set point
Negative Feedback and Corpus Luteum Regression
Progesterone, estradiol, and inhibin A suppress GnRH and gonadotropin secretion, maintaining low FSH and LH throughout the luteal phase. The corpus luteum is LH-dependent and has a finite lifespan (~12-16 days). Progesterone-induced decreases in LH pulse frequency and diminished post-receptor signaling both contribute to its demise. As the corpus luteum regresses, estradiol and progesterone fall abruptly, removing support for the endometrium.
Menstruation
The progressive loss of hormonal support causes inflammation, local hypoxia and ischemia, cytokine release, and vascular changes in the endometrium, leading to shedding (menstruation). Simultaneously, the drop in inhibin A and gonadal steroids allows FSH to begin rising again, initiating the next cycle.
If Pregnancy Occurs
If fertilization and implantation take place, the embryonic trophoblast secretes hCG (human chorionic gonadotropin), which mimics LH by binding to LH receptors on luteinized granulosa cells. This rescues the corpus luteum, sustaining progesterone and estradiol production and maintaining the secretory endometrium until the placenta takes over steroidogenesis (luteal-placental shift) at approximately 8-10 weeks.
Key Feedback Summary
| Hormone | Source | Feedback at Hypothalamus | Feedback at Pituitary |
|---|---|---|---|
| Estradiol (low-moderate) | Granulosa cells | Negative (via KNDy neurons) | Negative (more for FSH than LH) |
| Estradiol (high, sustained) | Dominant follicle | Permissive/positive | Positive - triggers LH surge |
| Progesterone | Corpus luteum | Negative (via KNDy/dynorphin) | Negative |
| Inhibin B | Early-mid follicular granulosa | - | Suppresses FSH selectively |
| Inhibin A | Dominant follicle, corpus luteum | - | Suppresses FSH selectively |
| Activin | Pituitary (autocrine) | - | Stimulates FSH synthesis |
Menstrual Cycle at a Glance
| Feature | Follicular Phase | Ovulation | Luteal Phase |
|---|---|---|---|
| Duration | 10-14 days (variable) | Day 14 | 14 days (constant) |
| Dominant hormone | Estradiol | LH/FSH surge | Progesterone |
| Endometrium | Proliferative | - | Secretory |
| Cervical mucus | Watery, ferning, sperm-friendly | Peak | Thick, non-ferning |
| BBT | Normal | - | Elevated |
| Key gonadal event | Follicle growth, dominant selection | Ovulation | Corpus luteum function |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), pp. 3172-3175 - primary source for HPO axis and feedback mechanisms
- Berek & Novak's Gynecology - two-cell/two-gonadotropin model, phase summary
- Costanzo Physiology 7th Edition, pp. 478-480 - phase-by-phase hormone events
- Medical Physiology (Boron & Boulpaep) - HPO axis driving the cycle
In flowchart
Generating Image
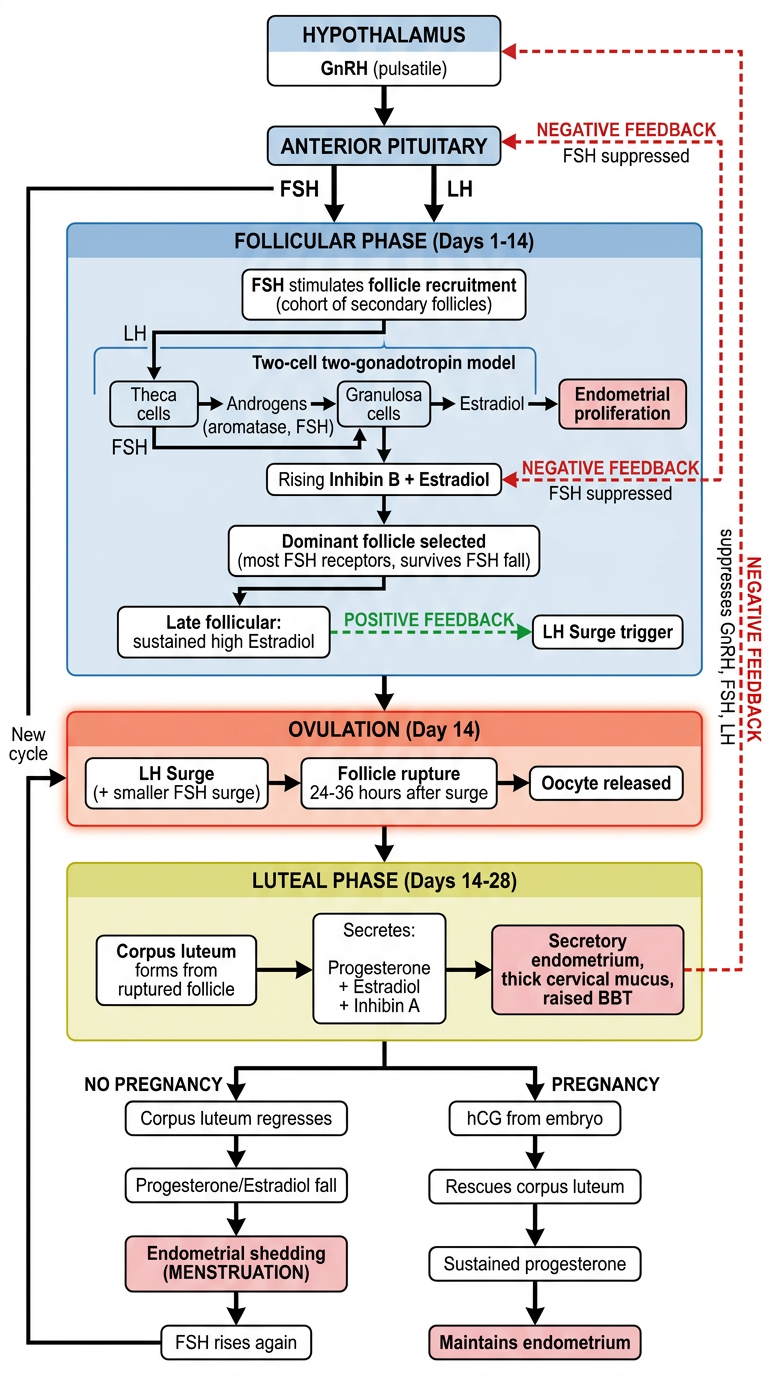
Here's the full flowchart of hormonal control of the menstrual cycle. It covers:
- HPO Axis at the top (Hypothalamus → GnRH → Pituitary → FSH/LH)
- Follicular Phase (Days 1-14): follicle recruitment, the two-cell/two-gonadotropin model, dominant follicle selection, and the negative→positive feedback switch of estradiol
- Ovulation (Day 14): the LH surge triggering follicle rupture 24-36 hours later
- Luteal Phase (Days 14-28): corpus luteum forming and secreting progesterone + estradiol, with negative feedback suppressing FSH/LH
- Two outcome branches: menstruation (if no pregnancy) vs. hCG rescue of corpus luteum (if pregnancy occurs)
Color coding: blue = follicular, orange = ovulation, green = luteal, red dashed = negative feedback, green dashed = positive feedback.
This is a shared conversation. Sign in to Orris to start your own chat.