Haemorrhoids
Reading File
Finding Sources
Searching PubMed
hemorrhoids management treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
hemorrhoids internal external anatomy classification
I now have comprehensive material. Let me compile the full answer.
Haemorrhoids
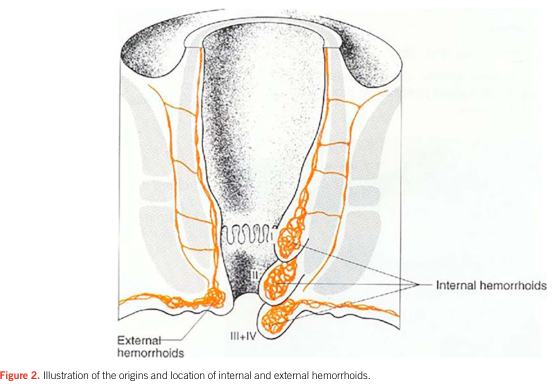
Definition & Anatomy
Haemorrhoids are dilated vascular channels (cushions) between the anal mucosa and the underlying internal anal sphincter. They represent a normal part of anal anatomy; their presence only constitutes disease when symptoms arise. They occur in three consistent positions: left lateral, right posterior, and right anterior. Lesions elsewhere should raise concern for carcinoma, lymphoma, or condyloma.
- Internal haemorrhoids — arise above the dentate line, covered by columnar or transitional mucosa; supplied by the superior rectal vein (portal system)
- External haemorrhoids — distal to the dentate line, covered by squamous epithelium; supplied by the inferior rectal vein (systemic)
Epidemiology
- Affects approximately 10–25% of the adult population; some estimates reach 5% of the general population for symptomatic disease
- Accounts for 1.9–3.5 million physician visits annually in the USA
- Up to 85% of multiparous women develop haemorrhoids, though most partially regress post-delivery
Pathogenesis
Symptoms arise from loss of connective tissue support causing prolapse and susceptibility to trauma from straining or hard stool passage. Elevated circulating matrix metalloproteinases are associated with symptomatic internal haemorrhoids.
Predisposing factors:
| Factor | Mechanism |
|---|---|
| Constipation / straining | ↑ intra-abdominal and venous pressure |
| Prolonged toilet sitting | Sustained venous pressure |
| Low-fibre diet | Hard stool → trauma |
| Pregnancy | Mechanical compression of superior rectal vein + progesterone → venous stasis |
| Obesity | ↑ intra-abdominal pressure |
| Portal hypertension | Dilated portosystemic collaterals |
Histologically: thin-walled, dilated submucosal vessels beneath anal/rectal mucosa.
Classification of Internal Haemorrhoids
| Grade | Features |
|---|---|
| I | Bleed ± enlarged; do not prolapse |
| II | Prolapse with defecation; reduce spontaneously |
| III | Prolapse; require manual reduction |
| IV | Remain prolapsed; irreducible |
External haemorrhoids may become thrombosed (clot under squamous epithelium of the anal verge), causing acute severe pain.
Clinical Features
Internal haemorrhoids:
- Painless bright red rectal bleeding — may coat the stool, drip into the toilet, or appear on tissue paper; occasionally dark blood or clots
- Prolapse — feeling of a lump, mucus/blood on underwear
- Pruritus ani — from perianal moisture
- Pain — only if thrombosis or strangulation occurs
External haemorrhoids:
- Pain is the dominant feature (squamous epithelium is exquisitely sensitive)
- Thrombosed external haemorrhoid: sudden, severe perianal pain with a tender, firm, bluish lump
Important: Most patients attributing symptoms to "haemorrhoids" have a different aetiology (fissure, pruritus ani, warts, etc.). Haemorrhoids may coexist with other pathology.
Diagnosis
- History and perianal inspection
- Digital rectal examination
- Anoscopy (beveled/slotted anoscope) — gold standard for visualising internal haemorrhoids and grading prolapse; exam may be normal between episodes
- Flexible sigmoidoscopy / colonoscopy — retroflexed view in rectum; indicated to exclude proximal colorectal disease when bleeding is the presentation
Treatment
1. Conservative (Medical) — All Grades
- Dietary fibre: 20–30 g/day; fibre diary to assess intake
- Fluid intake: 6–8 glasses of non-alcoholic, non-caffeinated beverage daily
- Avoid straining and prolonged toilet time
- Stool softeners: docusate sodium; polyethylene glycol 3350 if constipation persists
- Warm sitz baths: for comfort and hygiene
- Topical agents: phenylephrine/mineral oil/petrolatum or glucocorticoid-based creams for temporary relief of pain/itch (caution: steroids → candidiasis with prolonged use)
- Phlebotonics (e.g., diosmin/hesperidin — micronised purified flavonoid fraction): improve venous tone, stabilise capillary permeability; superior to placebo for acute symptoms; useful for grades II–III
2. Office-Based Procedures — Grades I–III (non-excisional)
| Procedure | Mechanism | Notes |
|---|---|---|
| Rubber band ligation (RBL) | Band applied proximal to haemorrhoid → ischaemic necrosis and mucosal fixation | Most common office procedure; grade II–III; bands placed above dentate line only — distal placement causes pain |
| Injection sclerotherapy | Sclerosant → fibrosis and fixation | |
| Infrared photocoagulation | Heat → coagulation and fibrosis | |
| Bipolar/direct current electrocoagulation | Electrical coagulation | |
| Cryotherapy | Cold-induced tissue destruction |
RBL detail: Usually 1 band per session (up to 3 if local anaesthesia added); reassess at 4–6 weeks; most patients managed with ≤3 procedures. Do not apply to external haemorrhoids.
3. Surgical — Grade IV / Failed Procedures
- Haemorrhoidectomy (excisional): Milligan-Morgan (open) or Ferguson (closed) — definitive treatment
- Stapled haemorrhoidopexy (procedure for prolapsing haemorrhoids, PPH)
- Doppler-guided haemorrhoidal artery ligation (DGHAL)
4. Thrombosed External Haemorrhoid
- If seen within 72 hours of onset → surgical excision (not simple incision) for rapid relief
- Beyond 72 hours or symptoms improving → conservative (sitz baths, stool softeners, analgesics)
Special Situations
Portal hypertension: Haemorrhoids represent portosystemic collaterals; bleeding can be more significant. Management is similar but with awareness of coagulopathy.
Pregnancy: Conservative management first; rubber band ligation for refractory cases. Haemorrhoidectomy if severely prolapsed, ulcerated, with bleeding, fissure, or fistula.
Differential Diagnosis
- Anal fissure (posterior midline pain, tearing on defecation)
- Rectal prolapse (full-thickness protrusion)
- Rectal polyps / carcinoma
- Condylomata acuminata
- Perianal abscess
- Pruritus ani
- Rectal varices (portal hypertension)
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease, 11e; Robbins & Cotran Pathologic Basis of Disease, 10e; Clinical Gastrointestinal Endoscopy, 3e; Yamada's Textbook of Gastroenterology, 7e; Bailey & Love's Short Practice of Surgery, 28e
This is a shared conversation. Sign in to Orris to start your own chat.