What are the different strategies of weaning from mechanical ventilator for md Anaesthesia exam long question .
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, high-quality content from multiple authoritative textbooks. I have everything needed to write an exhaustive MD Anaesthesia exam long answer. Let me now compose the complete answer.
Strategies of Weaning from Mechanical Ventilation
(MD Anaesthesia Long Question Answer)
INTRODUCTION
Weaning (also called "liberation") from mechanical ventilation is the process of gradually or abruptly withdrawing ventilatory support and transitioning a patient back to spontaneous breathing. It accounts for 40-50% of total mechanical ventilation time and prolonged unnecessary ventilation increases the risks of ventilator-associated pneumonia (VAP), respiratory muscle atrophy, barotrauma, and ICU complications. Approaching this as an active "liberation" process rather than passive weaning reduces unnecessary ventilator time by up to 40%.
Weaning has two distinct phases:
- Readiness Testing - determining if the patient can tolerate withdrawal of support
- Weaning / Liberation - the method by which ventilatory support is actually removed
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 2539)
PHASE 1: READINESS ASSESSMENT
A. Clinical Criteria for Weaning Readiness
Before any weaning attempt, the following must be satisfied:
| Parameter | Criterion |
|---|---|
| Underlying cause | Reversed or controlled |
| Consciousness | Awake, alert, cooperative |
| FiO₂ | ≤ 0.40-0.50 |
| PEEP | ≤ 5-8 cmH₂O |
| SpO₂ / SaO₂ | > 88-90% |
| Arterial pH | > 7.25 |
| Minute ventilation | < 10 L/min |
| Respiratory rate | < 30 breaths/min |
| Hemodynamics | Stable; no vasopressors or minimal support |
| Secretions | Thin, scanty; suctioning < every 4 hrs |
| Cough | Strong; able to lift head for > 5 seconds |
| Spontaneous VT | > 5 mL/kg IBW |
(Washington Manual of Medical Therapeutics, p. 292; Harrison's Principles of Internal Medicine 22E, p. 2352)
B. Mechanical Weaning Parameters (Weaning Indices)
| Index | Criterion for Weaning |
|---|---|
| Maximal inspiratory pressure (MIP / NIF) | < -25 cmH₂O (more negative = better strength) |
| Tidal volume (VT) | > 5 mL/kg |
| Vital capacity | > 10-15 mL/kg |
| Minute ventilation | < 10 L/min |
| Rapid Shallow Breathing Index (RSBI) | < 100-105 breaths/min/L |
(Morgan & Mikhail's Clinical Anesthesiology, 7e - Table 58-5, p. 2540)
C. Rapid Shallow Breathing Index (RSBI) - Yang-Tobin Index
The RSBI is the best single predictor of weaning outcome (Tobin Index):
RSBI = f (breaths/min) / VT (in litres)
- RSBI < 105: ~70% chance of successful extubation
- RSBI > 120: ~80% chance of weaning failure - retain ventilator support
- RSBI > 105 accurately predicts weaning failure; RSBI ≤ 105 is less accurate at predicting success
Other indices (NIF, minute ventilation, respiratory rate) individually have no better predictive value than RSBI.
(Schwartz's Principles of Surgery, 11e, p. 2346; Washington Manual, p. 292)
PHASE 2: WEANING STRATEGIES
OVERVIEW ALGORITHM (Harrison's, 22E)
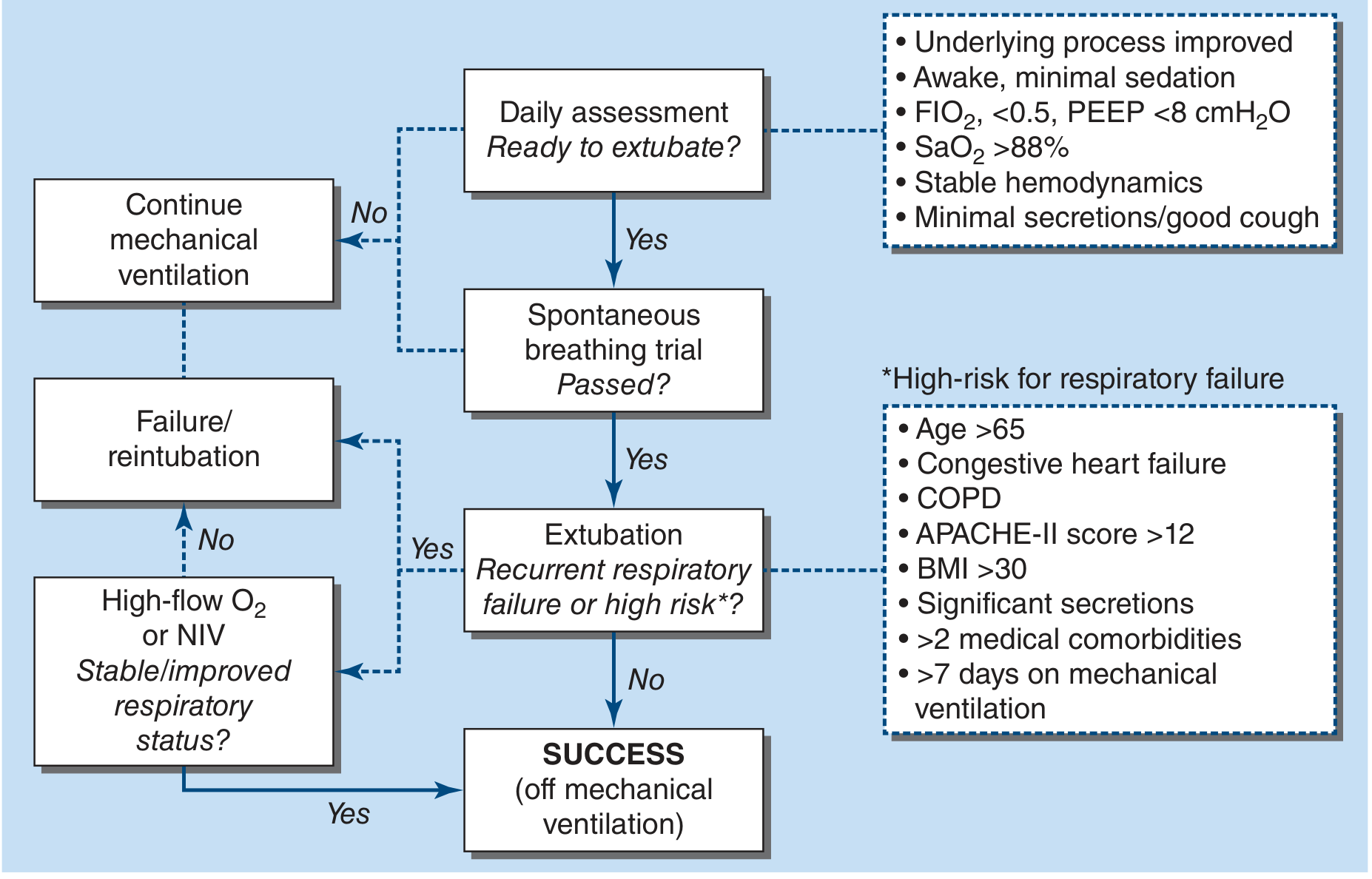
Strategy 1: Spontaneous Breathing Trial (SBT)
The SBT is the cornerstone of modern weaning and the most important single predictor of successful liberation. Daily sedation interruption + SBT should be routine in all ICU patients.
How to perform:
- Positive pressure is set to a minimum (PSV 5-7 cmH₂O) to compensate for ETT resistance, or the patient is placed on a T-piece
- Trial duration: 30 to 120 minutes
- If CPAP is used, set at 5 cmH₂O
SBT is "PASSED" if the patient shows:
- No marked anxiety or dyspnea
- Respiratory rate < 35 breaths/min
- SaO₂ > 90%
- Systolic BP between 90-180 mmHg
- Heart rate change < 20% from baseline
- RSBI < 105
SBT is "FAILED" if the patient develops:
- Tachypnea (RR > 35), accessory muscle use, paradoxical breathing
- SpO₂ < 90%
- Tachycardia, hypertension, arrhythmias
- Diaphoresis, agitation, altered mentation
If the patient passes the SBT, proceed to extubation assessment.
(Harrison's Principles of Internal Medicine 22E, p. 2352; Washington Manual, p. 292)
Strategy 2: T-Piece / Spontaneous Breathing Trial
Mechanism: Patient is removed from the ventilator but remains intubated. The ETT is connected to a heated, humidified circuit. No ventilator support is given.
Technique:
- T-piece attaches directly to the ETT or tracheostomy tube
- Humidified oxygen-air mixture flows into the proximal limb; exits distally
- Gas flow must be sufficient to prevent inspired air from recirculating
- End-tidal CO₂ monitoring may be used for additional safety
Monitoring for failure signs:
- Tachypnea, tachycardia, arrhythmias
- Chest retractions, use of accessory muscles
- Hypertension or hypotension
- Diaphoresis, anxiety
Sequential T-piece trials (for prolonged intubation or severe lung disease):
- Start with 10-30 min trials; progressively increase by 5-10 min
- Increase only if patient is comfortable, SpO₂ acceptable, no hypercarbia
Limitation: Patients may develop progressive atelectasis during prolonged T-piece trials because bypassing the larynx removes physiological PEEP. In this situation, CPAP at 5 cmH₂O is preferable to maintain FRC.
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 2541-2542)
Strategy 3: Pressure Support Ventilation (PSV) Weaning
Mechanism: No time-triggered machine breaths. Patient triggers all breaths; the ventilator provides a set inspiratory pressure boost to overcome ETT resistance and reduce work of breathing.
Technique:
- Initial PSV typically set at 15-20 cmH₂O; PEEP at 5 cmH₂O
- Gradually decrease PSV by 2-3 cmH₂O at a time
- Monitor VT (target 4-6 mL/kg), RR (target < 30 breaths/min), ABG
- When PSV reaches 5-8 cmH₂O, patient is considered weaned - proceed to extubation
Advantages:
- Reduces work of breathing imposed by the ETT
- Patient-triggered - maintains respiratory muscle activity and prevents disuse atrophy
- More comfortable; less sedation needed
- Better patient-ventilator synchrony
PSV for SBT: Low PSV (5-10 cmH₂O) + PEEP 5 cmH₂O is one of the two most widely accepted SBT methods (the other being T-piece).
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 2541; Washington Manual, p. 292)
Strategy 4: SIMV (Synchronized Intermittent Mandatory Ventilation) Weaning
Mechanism: A set number of mandatory mechanical breaths is delivered each minute, synchronized with patient's own inspiratory effort. In between mandatory breaths, the patient breathes spontaneously.
Technique:
- Mandatory rate is progressively decreased by 1-2 breaths/min
- Reduce only when ABG is acceptable: PaCO₂ < 45-50 mmHg, RR < 30 breaths/min
- Recheck ABG after minimum 15-30 min at each new setting
- When IMV rate reaches 2-4 breaths/min, discontinue if oxygenation remains acceptable
- If PSV is added to SIMV, reduce PSV to 5-8 cmH₂O before discontinuing
Monitoring targets (in pH/CO₂ retention patients): Use arterial pH > 7.35 rather than absolute PaCO₂
Key limitation:
- SIMV has the poorest weaning outcomes of all three techniques
- Mandatory breaths may impose excessive work if not well-synchronized
- Gradual step-down takes longer, prolonging ICU stay
- Still used most frequently in surgical and neurosurgical patients due to familiarity and ability to provide backup breaths
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 2540-2541; Washington Manual, p. 292)
Strategy 5: CPAP (Continuous Positive Airway Pressure) Weaning
Mechanism: Patient breathes spontaneously against a constant low level of positive airway pressure throughout the respiratory cycle. No inspiratory assist is provided.
Role in weaning:
- Applied at low levels (5 cmH₂O) to maintain FRC and prevent atelectasis when bypassing the larynx with an ETT
- Can serve as an SBT method, especially post-cardiac surgery patients
- Prevents the loss of physiological glottic PEEP
Advantage over T-piece: Maintains alveolar recruitment, especially in patients prone to atelectasis.
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 2542)
Strategy 6: Automated Weaning Strategies
Modern ventilators offer algorithms to automate weaning. These reduce clinician workload and respond in real-time to patient status.
a. Volume Support Ventilation (VSV)
- Delivers pressure-controlled breaths targeted to a set volume
- As patient effort increases and mechanics improve, PSV automatically decreases
- If effort diminishes or mechanics worsen, PSV automatically increases
- Risk: If set volume is excessive, a recovering patient may not take over the work of breathing; if set volume is inadequate, patient performs excessive work
b. Adaptive Support Ventilation (ASV)
- Uses a sophisticated algorithm to adjust the ventilatory pattern during machine-triggered breaths
- Small clinical studies show ASV can automatically wean ventilatory support safely
- Limitation: No large RCTs comparing ASV weaning to regular daily SBT strategies yet
c. PAV+ (Proportional Assist Ventilation Plus)
- Delivers support proportional to patient-generated flow and volume
- No set pressure, flow, or volume - the "gain" on patient effort is boosted
- Uses transient end-inspiratory occlusions to measure elastance and resistance, then calculates work of breathing
- Conceptually improves flow and cycle synchrony versus conventional PSV
Common caveat for automated strategies: The underlying premise is that gradual support reductions between SBTs facilitate weaning - but there is little clinical evidence supporting this in patients recovering from acute respiratory failure.
Two scenarios where automated weaning IS useful:
- Patient rapidly recovering from sedatives/anesthesia (alerts clinicians to return of adequate spontaneous effort)
- Patients requiring prolonged MV who have failed multiple SBTs (serves as diagnostic alert to return of respiratory function)
(Murray & Nadel's Textbook of Respiratory Medicine, p. 3185-3186)
POST-EXTUBATION MANAGEMENT
After successful extubation, patients require close monitoring. Options include:
Extubation to NIV (Non-Invasive Ventilation)
- In COPD patients intubated for acute respiratory failure, extubation to NPPV/NIV is associated with a reduction in mortality
- Indicated for patients with hypercapnia after extubation
High-Flow Nasal Oxygen (HFNO)
- For non-hypercapnic patients at high risk of post-extubation respiratory failure
- Similar efficacy to NIV in preventing reintubation; generally better patient comfort
- High-risk criteria for post-extubation failure: Age > 65, CHF, COPD, APACHE-II > 12, BMI > 30, significant secretions, > 2 comorbidities, > 7 days on MV
(Harrison's Principles of Internal Medicine 22E, p. 2352)
Cuff Leak Test
- For patients at risk of laryngeal edema (angioedema, traumatic intubation)
- Absence of cuff leak should generally preclude extubation
- Treat with IV corticosteroids for 12-24 hours before extubation in such patients
(Washington Manual of Medical Therapeutics, p. 292)
CAUSES OF WEANING FAILURE
Weaning failure occurs in up to 23.5% of patients who appear ready by objective criteria. Common causes include:
| Category | Causes |
|---|---|
| Respiratory | Bronchospasm, residual lung disease, atelectasis, secretions, pleural effusion |
| Cardiac | CHF, myocardial ischemia, volume overload |
| Neuromuscular | Critical illness myopathy/polyneuropathy, respiratory muscle fatigue, phrenic nerve palsy |
| Metabolic | Malnutrition, electrolyte deficiencies (hypophosphatemia, hypokalemia, hypomagnesaemia) |
| Neurological | Delirium, altered mental status, impaired cough/gag reflex |
| Endocrine | Hypothyroidism, adrenal insufficiency |
| Miscellaneous | Excess carbohydrate load (increases VCO₂ and drives RQ > 1), sleep deprivation, anemia |
Nutritional note: Excess carbohydrate feeding increases CO₂ production (RQ ≥ 1), increasing minute ventilation demands and precipitating weaning failure. Lipid-based nutrition (RQ ~0.7) is preferable.
(Morgan & Mikhail's, p. 2539; Schwartz's Principles of Surgery, p. 2346-2368)
COMPARISON OF WEANING STRATEGIES
| Feature | T-Piece | PSV | SIMV |
|---|---|---|---|
| Machine support | None | Inspiratory pressure assist | Mandatory backup breaths |
| Work of breathing | Highest | Intermediate (adjustable) | Variable |
| Comfort | Least | Best | Moderate |
| Weaning outcome | Equal to PSV | Equal to T-piece | Poorest |
| Best used in | Short-term ventilation, SBT | Most ICU patients | Surgical/neurosurgical |
| Risk of fatigue | Higher | Lower | Higher (if unsynchronized) |
| Atelectasis risk | Yes (no PEEP) | No | No |
PROTOCOL-DRIVEN WEANING
Protocol-driven weaning strategies are evidence-based standard of care. Benefits include:
- Reduced incidence of VAP
- Shorter duration of mechanical ventilation
- Reduced ICU length of stay
- Consistent daily assessment of weaning readiness
Key components of a standard weaning protocol:
- Daily screening using criteria checklist
- If criteria met → perform SBT (T-piece or low PSV)
- If SBT passed → evaluate for extubation
- If SBT failed → identify and treat reversible causes; repeat daily
- Daily sedation interruption ("spontaneous awakening trial" SAT) combined with SBT
(Schwartz's Principles of Surgery, 11e, p. 2345-2346)
SUMMARY
| Strategy | Mechanism | Key Feature |
|---|---|---|
| SBT (T-piece / low PSV) | Unassisted or minimally assisted breathing for 30-120 min | Gold standard; daily assessment mandatory |
| T-piece | No ventilator; spontaneous breathing through ETT | Risk of atelectasis; use CPAP if prolonged |
| PSV weaning | Decrease PSV by 2-3 cmH₂O; stop at 5-8 cmH₂O | Most comfortable; best synchrony |
| SIMV weaning | Decrease mandatory rate by 1-2 bpm; stop at 2-4 bpm | Poorest outcome; still used in surgical ICU |
| CPAP weaning | Constant low pressure to maintain FRC | Prevents atelectasis; used with T-piece trials |
| Automated (VSV, ASV, PAV+) | Algorithm-driven support reduction | Saves clinician time; limited RCT evidence |
| Extubation to NIV | Post-extubation NPPV | COPD patients; reduces mortality |
Key message for the exam: The combination of daily sedation interruption + daily SBT is the single most evidence-based intervention for timely liberation from mechanical ventilation. SIMV is the weakest weaning strategy. RSBI < 105 is the best single weaning index. Protocol-driven approaches reduce VAP and MV duration.
References (Textbooks):
- Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 2539-2542
- Harrison's Principles of Internal Medicine 22E (2025), pp. 2351-2352
- Washington Manual of Medical Therapeutics, pp. 291-292
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 3185-3186
- Schwartz's Principles of Surgery, 11e, pp. 2345-2346
This is a shared conversation. Sign in to Orris to start your own chat.