Relevance of size and contents of hernia for Anaesthesia
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a comprehensive, textbook-referenced answer on the anaesthetic relevance of hernia size and contents.
Relevance of Size and Contents of Hernia for Anaesthesia
The anaesthetic significance of a hernia depends on what type of hernia it is, how large it is, and what the hernia sac contains. These factors influence aspiration risk, airway management strategy, respiratory mechanics, and the urgency of the procedure.
1. Hiatus (Hiatal) Hernia - The Most Anesthetically Relevant
Why it matters to the anaesthesiologist
Hiatus hernia is the most commonly encountered hernia type in anaesthetic practice and carries the greatest perioperative risk. As stated in Morgan and Mikhail's Clinical Anesthesiology, "Perioperative aspiration of gastric contents (Mendelson syndrome) is a potentially fatal complication of anesthesia. Hiatal hernia is commonly associated with symptomatic GERD, which is considered a predisposing factor for aspiration."
Types and their anaesthetic relevance
| Type | Description | Anaesthetic Significance |
|---|---|---|
| Type I (Sliding) | Esophagogastric junction + fundus herniate axially into thorax; ~90% of cases | Lower esophageal sphincter (LES) above diaphragm - cannot respond to increased abdominal pressure. Reduced barrier pressure during coughing/straining leads to regurgitation. HIGH aspiration risk. |
| Type II (Paraesophageal) | Portion of stomach herniates next to esophagus; esophagogastric junction remains in abdomen | Main complications are blood loss, anaemia, and gastric volvulus. Less reflux risk but mechanical complications. |
- Miller's Anesthesia, 10e, p. 7269-7270
Size matters: Large hiatal hernia
A large hiatal hernia is specifically flagged as a non-reversible risk factor. If the risk factor is irreversible (e.g., large hiatal hernia) or the case is an emergency, proper anaesthetic technique must minimize aspiration risk - this means regional anaesthesia or rapid-sequence induction (RSI) rather than postponing. - Morgan and Mikhail's, 7e, p. 537
The CXR below shows a large hiatus hernia with a dilated intrathoracic stomach and an air-fluid level behind the heart - these patients are at HIGH risk for aspiration on induction:
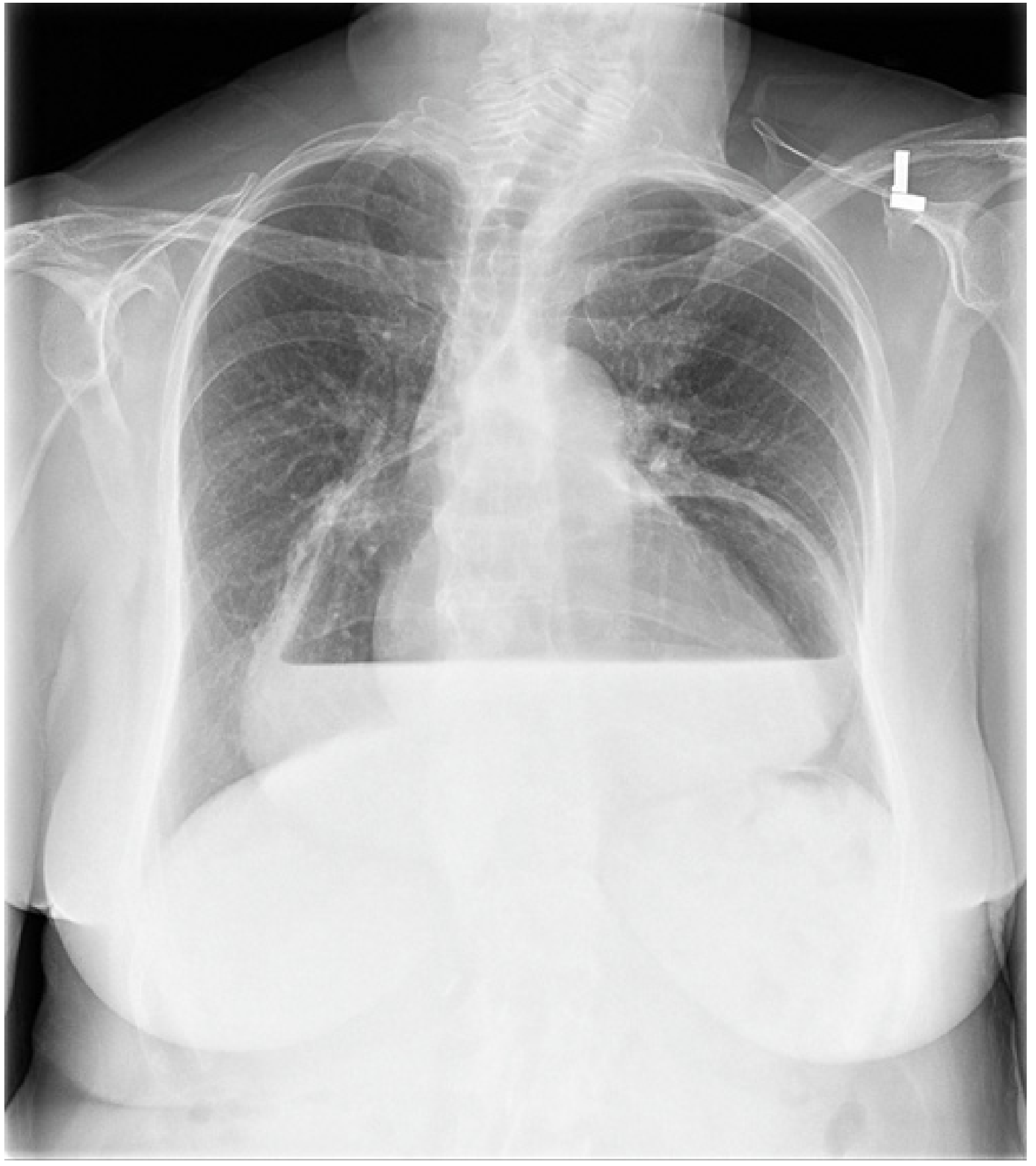
Miller's Anesthesia, 10e - Fig. 49.50
Symptomatic clues that increase aspiration risk
- Passive reflux of gastric fluid (acid taste, sensation of fluid reaching mouth)
- Paroxysms of coughing or wheezing at night or when supine (suggests chronic aspiration)
- Mild or occasional heartburn alone does NOT significantly increase risk
- Morgan and Mikhail's, 7e, p. 535
2. Aspiration Risk - Volume and Contents of Gastric Herniation
The seriousness of aspiration depends on volume and composition of the aspirate:
- Gastric volume > 2.5 mL (0.4 mL/kg) AND pH < 2.5 traditionally defines "at-risk" status
- Some investigators revise this to pH < 3.5 with volume > 50 mL (acidity considered more important)
- High-risk populations who are more likely to have large-volume, acidic gastric contents: patients with acute abdomen, peptic ulcer disease, children, elderly, diabetics, pregnant women, and obese patients
- Morgan and Mikhail's, 7e, p. 536
Hernia Contents That Signal Increased Risk
| Hernia Contents / Scenario | Anaesthetic Concern |
|---|---|
| Stomach (hiatus hernia) | Reflux, aspiration of acid, Mendelson syndrome |
| Bowel (incarcerated/strangulated hernia) | Intestinal obstruction = full stomach, always treat as emergency with RSI |
| Gas-filled bowel in chest (congenital diaphragmatic hernia) | Severe respiratory compromise, pulmonary hypoplasia |
| Large abdominal hernia with "loss of domain" | Respiratory failure post-repair due to abdominal compartment syndrome |
3. Incarcerated / Strangulated Hernia - Emergency Anaesthetic Implications
When hernia contents (typically bowel) are incarcerated or strangulated:
- The patient should be treated as having a full stomach regardless of fasting history
- Bowel obstruction is explicitly listed as a patient at risk of aspiration alongside hiatal hernia - Barash Clinical Anesthesia, 9e, Table 23-13
- RSI with tracheal intubation is mandatory
Anaesthetic technique for the high-aspiration-risk patient (full stomach or irreversible hernia risk):
- Consider regional anaesthesia with minimal sedation if practical
- If general anaesthesia is required:
- Confirm suction availability before induction
- Preoxygenation (3-5 min in patients with lung disease)
- Rapid-sequence induction (RSI):
- Propofol or etomidate induction bolus
- Succinylcholine 1.5 mg/kg OR rocuronium 0.9-1.2 mg/kg immediately after induction agent
- Avoid bag-mask ventilation (prevents gastric gas insufflation and risk of emesis)
- Cricoid pressure (Sellick maneuver) - controversial but classically applied
- Intubate as soon as neuromuscular blockade confirmed
- Maintain cricoid pressure until ETT cuff inflated and placement confirmed
- Remain intubated until airway reflexes and consciousness have returned fully
- Morgan and Mikhail's, 7e, p. 537-538; Barash Clinical Anesthesia, 9e
4. Large Abdominal Wall Hernias - Respiratory Mechanics
For large incisional or ventral hernias with loss of domain (LOD) - where hernia contents can no longer be reduced into the abdominal cavity - size has direct intraoperative and postoperative respiratory consequences:
- Hernia size and hernia volume are documented preoperative predictors of respiratory failure following repair
- Patients who develop changes in peak plateau pressures of ≥6 mm Hg after abdominal closure have an 8.6x increased risk of respiratory complications
- If elevated pulmonary plateau pressures are noted during closure, plan for ICU admission with ongoing ventilation for at least 24 hours with muscle relaxation
- CT imaging is essential preoperatively to plan the approach and counsel patients about the need for postoperative ICU care
- Current Surgical Therapy, 14e, p. 750
5. Congenital Diaphragmatic Hernia (CDH) - Neonatal Anaesthesia
Contents: Abdominal viscera (including liver, spleen, bowel) herniate through the diaphragm (most commonly left-sided Bochdalek defect) into the thorax.
Why size and contents matter:
- More viscera in the chest = greater degree of pulmonary hypoplasia on the ipsilateral and contralateral sides
- Associated with pulmonary hypertension (not corrected by surgery alone - may worsen post-repair)
-
50% associated with other congenital anomalies - full organ system evaluation required before surgery
Key anaesthetic points for CDH:
- Avoid bag-mask ventilation before intubation - this inflates GI contents within the chest and worsens compression
- Use permissive ventilation - limit peak inspiratory pressures and PEEP, allow permissive hypercapnia to reduce barotrauma risk
- High-frequency oscillatory ventilation is often required
- Manage pulmonary hypertension by avoiding hypoxemia and excessive hypercapnia
- Deep general anaesthesia to blunt the stress response
- Risk of barotrauma-induced pneumothorax on ipsilateral or contralateral side
- Severely unstable neonates may need ECMO and inhaled nitric oxide preoperatively
- Surgery should NOT be rushed - wait for haemodynamic and respiratory stabilisation
- Miller's Anesthesia, 10e, p. 10639-10640
6. Preoperative Pharmacological Prophylaxis (when aspiration risk is identified)
For patients with hiatus hernia or other hernia-related aspiration risk:
| Drug | Mechanism | Role |
|---|---|---|
| H2-receptor antagonists (ranitidine, famotidine) | Decrease acid secretion | Reduce further acid production; affect both pH and volume; long duration provides recovery room protection |
| Proton pump inhibitors (omeprazole) | Block H+/K+ ATPase | Reduce gastric acidity |
| Metoclopramide | Shortens gastric emptying; increases LES tone | Reduces volume; cannot clear large amounts of food |
| Non-particulate antacids (sodium citrate) | Neutralise existing acid | Acts immediately on gastric contents already present |
- Bailey and Love's Surgery, 28e; Morgan and Mikhail's, 7e
Summary Table
| Hernia Type | Key Anaesthetic Concern | Size/Content Impact |
|---|---|---|
| Hiatal (sliding) | Aspiration / Mendelson syndrome | Larger hernia = lower LES barrier = higher reflux risk |
| Incarcerated bowel hernia | Full stomach / obstruction | Bowel in sac = treat as full stomach, RSI mandatory |
| Large ventral/incisional hernia (LOD) | Respiratory failure post-repair | Larger size = greater intraoperative pressure rise, ICU needed |
| Congenital diaphragmatic hernia | Pulmonary hypoplasia, pulmonary HTN | More visceral content in chest = worse pulmonary development |
| Paraesophageal hernia | Gastric volvulus, haemorrhage | Less reflux risk, but mechanical/haemodynamic concerns |
Sources: Morgan and Mikhail's Clinical Anesthesiology 7e | Miller's Anesthesia 10e | Barash Clinical Anesthesia 9e | Bailey and Love's Surgery 28e | Current Surgical Therapy 14e
This is a shared conversation. Sign in to Orris to start your own chat.