chronic diarrhea consultant approach easy to understand and get refference only from harrison 2026
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the content I need from Harrison's. Let me compile the comprehensive, easy-to-understand response.
Chronic Diarrhea: Consultant Approach
Reference: Harrison's Principles of Internal Medicine, 22nd Edition (2025)
1. Definition
Diarrhea lasting >4 weeks warrants evaluation to exclude serious underlying pathology. Unlike acute diarrhea, most causes of chronic diarrhea are non-infectious. Classification by pathophysiologic mechanism gives a rational framework for management.
Harrison's, p. 350
2. Pathophysiologic Classification (The "WHY" of Diarrhea)
Harrison's organizes chronic diarrhea into 6 mechanism-based categories. Think of this as your core mental model:
A. Secretory Diarrhea
Key feature: Watery, large-volume, persists with fasting, no osmotic gap in stool.
The gut is actively secreting too much fluid - or not absorbing enough - due to a derangement in electrolyte transport.
| Cause | Examples |
|---|---|
| Medications/toxins | Stimulant laxatives (senna, bisacodyl), ethanol, arsenic, olmesartan (sprue-like), GLP-1 agonists (semaglutide) |
| Bowel resection/fistula | Short bowel; worsens with eating (unlike other secretory causes) |
| Bile acid diarrhea (BAD) | Accounts for ~40% of unexplained chronic diarrhea; ileal dysfunction/resection <100 cm |
| Hormone-secreting tumors | Carcinoid (serotonin, VIP), VIPoma ("pancreatic cholera" - stool up to 20 L/d), Gastrinoma, Medullary thyroid cancer |
| Addison's disease | Mineralocorticoid deficiency |
Harrison's, pp. 350-352
B. Osmotic Diarrhea
Key feature: Watery, stops with fasting, elevated fecal osmotic gap (>50 mOsm/kg).
Unabsorbed solutes drag water into the gut lumen.
| Cause | Examples |
|---|---|
| Osmotic laxatives | Mg²⁺, phosphate, sulfate (antacids, bowel preps) |
| Disaccharide deficiency | Lactase deficiency (most common) |
| Non-absorbable carbohydrates | Fructose, sorbitol, lactulose, polyethylene glycol, FODMAPs |
Harrison's, p. 350
C. Steatorrheal (Fatty) Diarrhea
Key feature: Bulky, greasy, foul-smelling stool; weight loss; fat-soluble vitamin deficiency (A, D, E, K).
Three sub-levels of fat malabsorption:
| Level | Mechanism | Causes |
|---|---|---|
| Intraluminal maldigestion | Not enough digestive enzymes or bile | Chronic pancreatitis, pancreatic cancer, bile salt deficiency |
| Mucosal malabsorption | Damaged absorptive surface | Celiac disease, Whipple's disease, infections, drug-induced enteropathy |
| Post-mucosal obstruction | Lymphatic blockage | Primary/secondary lymphatic obstruction, amyloidosis |
Harrison's, p. 350
D. Inflammatory Diarrhea
Key feature: Blood or leukocytes in stool, fever, abdominal pain, elevated CRP/ESR.
Mucosal damage disrupts both absorption and barrier function.
| Cause |
|---|
| Idiopathic IBD (Crohn's disease, ulcerative colitis) |
| Microscopic colitis (lymphocytic & collagenous) |
| Immune-mediated (food allergy, eosinophilic gastroenteritis, graft-vs-host disease) |
| Infections (invasive bacteria, viruses, parasites) |
| Radiation injury |
| GI malignancies |
Harrison's, p. 350
E. Dysmotility Diarrhea
Key feature: Associated with abdominal cramping, bloating, urgency; often IBS pattern.
Too-rapid transit = less time for absorption.
| Cause |
|---|
| IBS (including post-infectious IBS) |
| Visceral neuropathies |
| Hyperthyroidism |
| Prokinetic drugs |
| Post-vagotomy |
Harrison's, p. 350
F. Factitial / Iatrogenic Causes
| Category | Examples |
|---|---|
| Factitial | Munchausen syndrome, eating disorders (laxative abuse) |
| Iatrogenic | Cholecystectomy, ileal resection, bariatric surgery, vagotomy, fundoplication |
Harrison's, p. 350
3. Diagnostic Approach (The "HOW" to Evaluate)
The key principle from Harrison's: "The diagnostic evaluation must be rationally directed by a careful history, including medications, and physical examination."
Step 1: History - Key Questions to Ask
- Onset and duration - exactly when did it start?
- Pattern - constant vs. intermittent, nocturnal episodes (organic > functional)?
- Stool character - watery, fatty, bloody? Bristol Stool Scale
- Volume - large vs. small-volume stools
- Aggravating factors - does it stop with fasting? (osmotic) or persist? (secretory)
- Dietary associations - dairy, wheat, sorbitol-containing foods, FODMAPs
- Travel history - backpacking, tropical regions (think Giardia)
- Medications - every drug, including OTC, supplements, laxatives
- Weight loss, fever, arthralgia, skin changes - alarm/organic features
- Family history - IBD, celiac disease
- Prior surgery - cholecystectomy, ileal resection, bariatric
Harrison's, p. 354
Step 2: Physical Examination - What to Look For
| Finding | Suggests |
|---|---|
| Anemia, edema, clubbing, dermatitis herpetiformis | Malabsorption, IBD |
| Thyroid mass, wheezing, heart murmur, flushing | Carcinoid, hyperthyroidism |
| Orthostasis, pupil abnormalities | Autonomic neuropathy (DM) |
| Abdominal mass or tenderness | Neoplasia, IBD |
| Perianal fistulas, anal sphincter laxity | Crohn's disease, fecal incontinence |
| Oral aphthous ulcers | IBD, celiac disease |
| Erythema nodosum | Ulcerative colitis |
| Lymphadenopathy | Lymphoma, Whipple's |
Harrison's, p. 354
Step 3: Initial Laboratory Screen
"Limited screen for organic disease" (from the algorithm):
- Hematology: CBC (Hb, MCV, MCH) - anemia suggests malabsorption/IBD
- Chemistry: Albumin (low = malabsorption/inflammation), electrolytes (hypokalemia in secretory), LFTs
- Inflammatory markers: CRP, ESR
- Nutritional screen: Iron, folate, B12
- Celiac screen: TTG-IgA
- Stool: Fecal calprotectin (inflammation), occult blood
- 7αC4 or serum C4 (bile acid marker): Elevated in bile acid diarrhea
Harrison's, p. 354 - Fig. 49-4
Step 4: Diagnostic Algorithm - The Branching Logic
The Harrison's algorithm (Fig. 49-4) branches based on the dominant stool character:
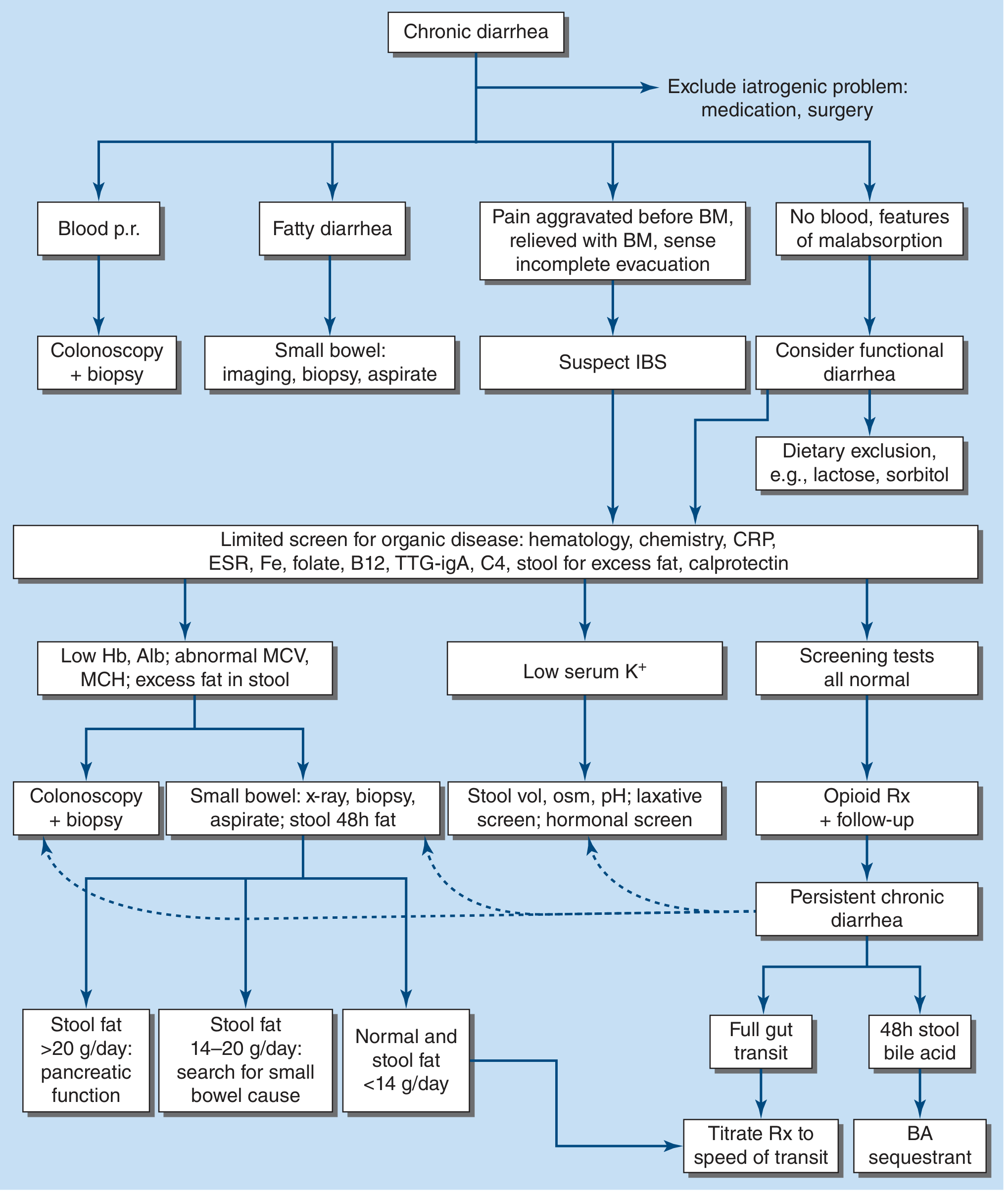
Figure 49-4 from Harrison's - Algorithm for management of chronic diarrhea
Branch 1: Blood per rectum
→ Colonoscopy + biopsy (rule out IBD, malignancy, microscopic colitis)
Branch 2: Fatty diarrhea (steatorrhea)
→ Small bowel: imaging, biopsy, aspirate
- Stool fat >20 g/day → evaluate pancreatic function (exocrine insufficiency)
- Stool fat 14-20 g/day → search for small bowel mucosal cause
- Stool fat <14 g/day → normal range
Branch 3: Pain before BM, relieved with BM, incomplete evacuation
→ Suspect IBS → sigmoidoscopy with biopsies to exclude microscopic colitis
Branch 4: No blood, no malabsorption features
→ Consider functional diarrhea → dietary exclusion (lactose, sorbitol)
When screening tests are abnormal:
- Low Hb/Alb + abnormal MCV/MCH + excess fat in stool → Colonoscopy + biopsy AND small bowel x-ray/biopsy
- Low serum K⁺ → Stool volume, osmolality, pH; laxative screen; hormonal screen (gastrin, VIP, calcitonin, TSH, urinary 5-HIAA, histamine)
- All normal → Empirical opioid (loperamide) + follow-up; if persistent → gut transit test + 48h stool bile acid
Step 5: Targeted Investigation Based on Suspected Mechanism
Secretory diarrhea (normal osmotic gap):
- Stool microbiologic studies (multiplex PCR panel, cultures, ova & parasites, Giardia antigen)
- Breath tests for SIBO (glucose/lactulose - H₂/CH₄)
- Upper endoscopy + colonoscopy with biopsies
- Small bowel imaging (CT enterography or MR enteroclysis)
- Hormonal screens: gastrin, VIP, calcitonin, TSH, urinary 5-HIAA, histamine
Osmotic diarrhea (elevated osmotic gap):
- Lactose breath test or therapeutic trial of lactose exclusion
- Fructose tolerance test
- Fecal Mg²⁺ level (check surreptitious laxative use)
- Stool pH <5.6 suggests carbohydrate malabsorption
Steatorrheal diarrhea:
- Endoscopy + small-bowel biopsy with aspirate for cultures
- Pancreatic function tests (if small bowel unrevealing)
- CT/MRI abdomen for pancreatic pathology
Inflammatory diarrhea:
- Stool pathogen testing
- Colonoscopy with biopsies
- Small bowel imaging
Harrison's, pp. 354-355
4. Treatment
Treatment depends on the etiology - curative, suppressive, or empirical.
| Goal | Examples |
|---|---|
| Curative | Resect colorectal cancer; antibiotics for Whipple's/tropical sprue; stop offending drug |
| Suppressive (mechanism-targeted) | |
| - Lactase deficiency | Lactose-restricted diet |
| - Celiac disease | Gluten-free diet |
| - IBD | Anti-inflammatory agents (mesalamine, steroids, biologics) |
| - Bile acid malabsorption | Bile acid sequestrants (cholestyramine, colestipol, colesevelam) |
| - Gastrinoma | Proton pump inhibitors |
| - Carcinoid syndrome | Octreotide (somatostatin analogue) |
| - Medullary thyroid cancer | Indomethacin (prostaglandin inhibitor) |
| - Pancreatic insufficiency | Pancreatic enzyme replacement |
| Empirical (when cause unknown) | |
| - Mild-moderate watery | Loperamide or diphenoxylate |
| - Severe | Codeine or tincture of opium (avoid in severe IBD - risk of toxic megacolon) |
| - Diabetic diarrhea | Clonidine (α₂-agonist) - skin patch preferred (less orthostasis) |
| - IBS-D | 5-HT3 antagonists (alosetron, ondansetron); Rifaximin; Eluxadoline* |
| - AIDS-associated diarrhea | Crofelemer (antisecretory) |
⚠️ Eluxadoline is contraindicated or risky in patients post-cholecystectomy (sphincter of Oddi spasm → acute pancreatitis)
Always: Fluid and electrolyte repletion + fat-soluble vitamin replacement if steatorrhea present.
Harrison's, p. 355
Summary: The Consultant's Mental Checklist
Chronic diarrhea (>4 weeks)
│
├── 1. HISTORY → mechanism clue + alarm features
├── 2. EXAMINATION → systemic signs
├── 3. BASIC LABS + STOOL SCREEN
├── 4. BRANCH by stool type:
│ Blood → colonoscopy
│ Fatty → small bowel workup
│ IBS pattern → sigmoidoscopy/biopsy
│ Functional pattern → dietary exclusion
├── 5. IF STILL UNCLEAR → quantitative stool analysis
│ Osmotic gap → osmotic/secretory distinction
│ Stool fat → steatorrheal workup
│ Hormonal screen → if secretory + low K⁺
└── 6. TREAT based on mechanism identified
Reference: Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill Medical), Chapter 49 - Diarrhea and Constipation, pp. 350-355.
This is a shared conversation. Sign in to Orris to start your own chat.