Non alcoholic hepatitis b and c negative causes of cld
"chronic liver disease" AND etiology AND "non-alcoholic" AND "hepatitis B negative"
Non-Alcoholic, Hepatitis B & C Negative Causes of Chronic Liver Disease (CLD)
1. Metabolic/Steatotic Liver Disease
- NAFLD/NASH (Non-alcoholic fatty liver disease / Non-alcoholic steatohepatitis) - now the most common cause of CLD globally, strongly linked to obesity, type 2 diabetes, dyslipidemia, and metabolic syndrome. Approximately 1 in 10 NASH patients progress to cirrhosis. Many cases of previously labeled "cryptogenic cirrhosis" are now recognised as undetected NASH.
2. Genetic/Inherited Metabolic Disorders
| Condition | Mechanism |
|---|---|
| Hereditary Hemochromatosis | Iron overload (HFE gene mutations - C282Y, H63D; also HJV, HAMP, TFR2, ferroportin) |
| Wilson's Disease | Copper overload (ATP7B gene mutation) |
| Alpha-1 Antitrypsin Deficiency | Misfolded protein accumulates in hepatocytes |
| Glycogen Storage Disease | Types IA, III, and IV |
| Tyrosinemia | Toxic metabolite accumulation |
| Galactosemia | Galactose-1-phosphate uridyltransferase deficiency |
3. Autoimmune Liver Diseases
- Autoimmune Hepatitis (AIH) - Immune-mediated destruction of hepatocytes; often responds to immunosuppression
- Primary Biliary Cholangitis (PBC) - Autoimmune destruction of small intrahepatic bile ducts; presents with malaise, pruritus, and cholestasis; mainly affects middle-aged women
- Primary Sclerosing Cholangitis (PSC) - Progressive inflammation and fibrosis of intra- and extra-hepatic biliary tree; strongly associated with ulcerative colitis; mainly affects young men; high risk of cholangiocarcinoma
4. Vascular/Outflow Disorders
- Budd-Chiari Syndrome - Hepatic vein thrombosis causing outflow obstruction; presents with ascites, hepatomegaly, and pain
- Cardiac cirrhosis / Chronic congestive heart failure - Right-sided heart failure causing chronic hepatic venous congestion
- Sinusoidal obstruction syndrome (veno-occlusive disease)
5. Drug-Induced Liver Injury (DILI) / Toxins
- Methotrexate (long-term use)
- Amiodarone
- Isoniazid, rifampicin
- Herbal supplements and traditional medicines
- Carbon tetrachloride and industrial solvents
6. Parasitic/Infectious (Non-viral)
- Schistosomiasis - Causes periportal (pipestem) fibrosis; major cause in endemic regions (Africa, South America, South/East Asia)
7. Biliary Causes
- Biliary atresia (neonatal/pediatric)
- Caroli's disease - Congenital cystic dilation of intrahepatic bile ducts
- Chronic biliary obstruction (stones, strictures)
8. Inflammatory / Granulomatous
- Sarcoidosis - Hepatic granulomata leading to fibrosis
9. Miscellaneous / Rare
- Neonatal/congenital alloimmune hepatitis
- Aceruloplasminemia
- Congenital atransferrinemia
- Reye's syndrome (children - following viral illness + aspirin)
- Acute/chronic fatty liver of pregnancy (rare)
10. Cryptogenic CLD
- No identifiable cause despite full work-up. The proportion has declined significantly as NASH is increasingly recognised as the underlying etiology in many of these patients.
Key point: NASH/NAFLD is now the leading non-alcoholic, non-viral cause of CLD worldwide and is projected to overtake all other etiologies for liver transplantation indications in the near future.
Create a diagnostic flowchart or decision tree for CLD workup
A detailed medical diagnostic flowchart / decision tree for Chronic Liver Disease (CLD) workup. The flowchart should be clean, professional, and use a white background with color-coded boxes. Structure it as follows: START at the top: "Suspected Chronic Liver Disease" (symptoms: fatigue, jaundice, hepatomegaly, ascites, abnormal LFTs) STEP 1 - Initial Assessment box: History (alcohol use, drug history, family history, metabolic risk factors) + Physical Exam + Basic Labs (LFTs, CBC, coagulation, albumin, bilirubin) STEP 2 - Imaging box: Ultrasound abdomen (assess liver size, echogenicity, portal hypertension, splenomegaly) STEP 3 - First branching decision: "Alcohol History Significant?" → YES → Alcoholic Liver Disease (confirm with biopsy if needed) | NO → continue STEP 4 - Next branch: "HBsAg positive?" → YES → Hepatitis B CLD | NO → continue STEP 5 - Next branch: "Anti-HCV positive + HCV RNA?" → YES → Hepatitis C CLD | NO → continue STEP 6 - "Metabolic Risk Factors? (Obesity, DM, Dyslipidemia, Metabolic Syndrome)" → YES → NAFLD/NASH workup (liver biopsy or FibroScan) | NO → continue STEP 7 - Autoimmune Panel branch: ANA, ASMA, AMA, IgG, IgM - AMA positive + high IgM → Primary Biliary Cholangitis (PBC) - ASMA/ANA positive + high IgG → Autoimmune Hepatitis (AIH) - MRCP/ERCP changes → Primary Sclerosing Cholangitis (PSC) STEP 8 - Metabolic/Genetic workup: - Serum ferritin + transferrin saturation high → HFE gene mutation → Hereditary Hemochromatosis - Serum ceruloplasmin low + urine copper high → Wilson's Disease - Alpha-1 antitrypsin level low → Alpha-1 Antitrypsin Deficiency STEP 9 - Vascular causes: Doppler USS / CT venography - Hepatic vein obstruction → Budd-Chiari Syndrome - Right heart failure → Cardiac Cirrhosis STEP 10 - Drug/Toxin box: Review medication history → DILI STEP 11 - If all above negative → Liver Biopsy → Cryptogenic Cirrhosis Final boxes at bottom for ALL confirmed diagnoses: "Assess Severity - Child-Pugh Score / MELD Score" → "Manage Complications" → "Consider Liver Transplant if End-Stage" Use color coding: Blue for decision diamonds, green for confirmed diagnoses, orange for investigation boxes, red for end-stage/transplant. Add small icons where appropriate. Make it tall and detailed with clear arrows.
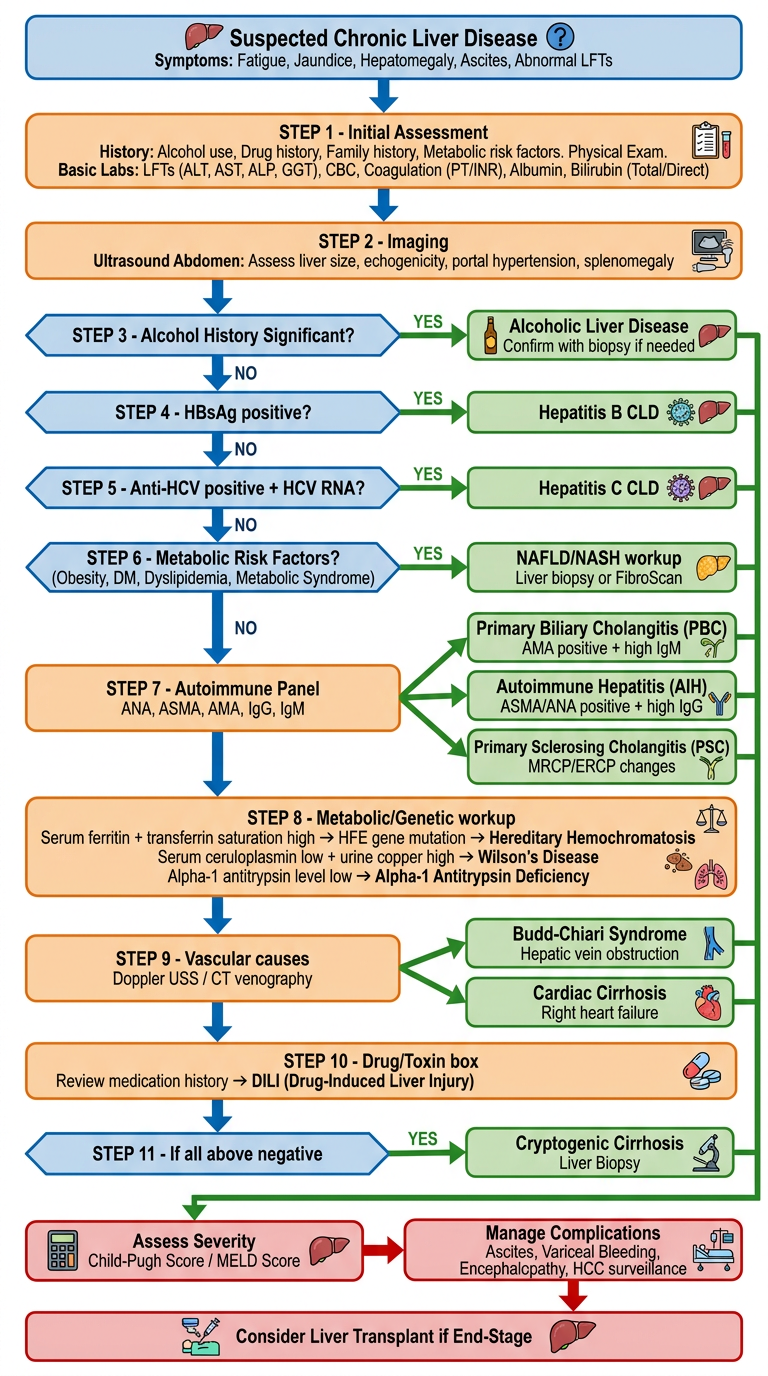
- Initial assessment - history, exam, basic labs, and abdominal ultrasound
- Common causes first - alcohol, then hepatitis B, then hepatitis C (screen-and-exclude approach)
- Metabolic workup - NAFLD/NASH if metabolic risk factors present
- Autoimmune panel - AMA, ANA, ASMA, IgG/IgM to differentiate PBC, AIH, and PSC
- Genetic/metabolic screen - ferritin/transferrin saturation (hemochromatosis), ceruloplasmin/urine copper (Wilson's), alpha-1 antitrypsin level
- Vascular causes - Doppler USS / CT venography for Budd-Chiari and cardiac cirrhosis
- Drug/toxin review - DILI
- Liver biopsy for unresolved cases - cryptogenic cirrhosis
- Final common pathway - all confirmed diagnoses feed into Child-Pugh/MELD scoring, complication management, and transplant evaluation