Types of incision clip ligature and sutures
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive material from multiple textbooks. Let me compile a thorough answer covering all three topics: incisions, clip ligatures, and sutures.
Types of Surgical Incisions, Clip Ligatures, and Sutures
1. SURGICAL INCISIONS
Principles for Planning a Skin Incision
Before making any incision, the surgeon must consider three key factors (Bailey & Love's Short Practice of Surgery, 28th ed.):
- Skin tension lines and cosmesis - Langer's lines (orientation of dermal collagen fibres) and, more practically, Relaxed Skin Tension Lines (RSTLs) - creases formed when skin is pinched and relaxed - guide incision placement to reduce scarring, particularly in head and neck surgery.
- Anatomical structures - Incisions should avoid bony prominences and respect underlying nerves, vessels, previous scars, and body habitus.
- Adequate surgical access - Cosmetic compromise must never render the operation ineffective or dangerous.
An elliptical incision must be at least three times as long as it is wide for wound healing without tension.
Technique: The blade is pressed firmly at right angles to the skin - oblique incisions cause undercutting, leading to edge necrosis. Tension is applied across the incision line by the non-dominant hand.
Types of Abdominal Incisions
Here is the surgical incisions diagram from Bailey & Love's (Fig. 7.6):
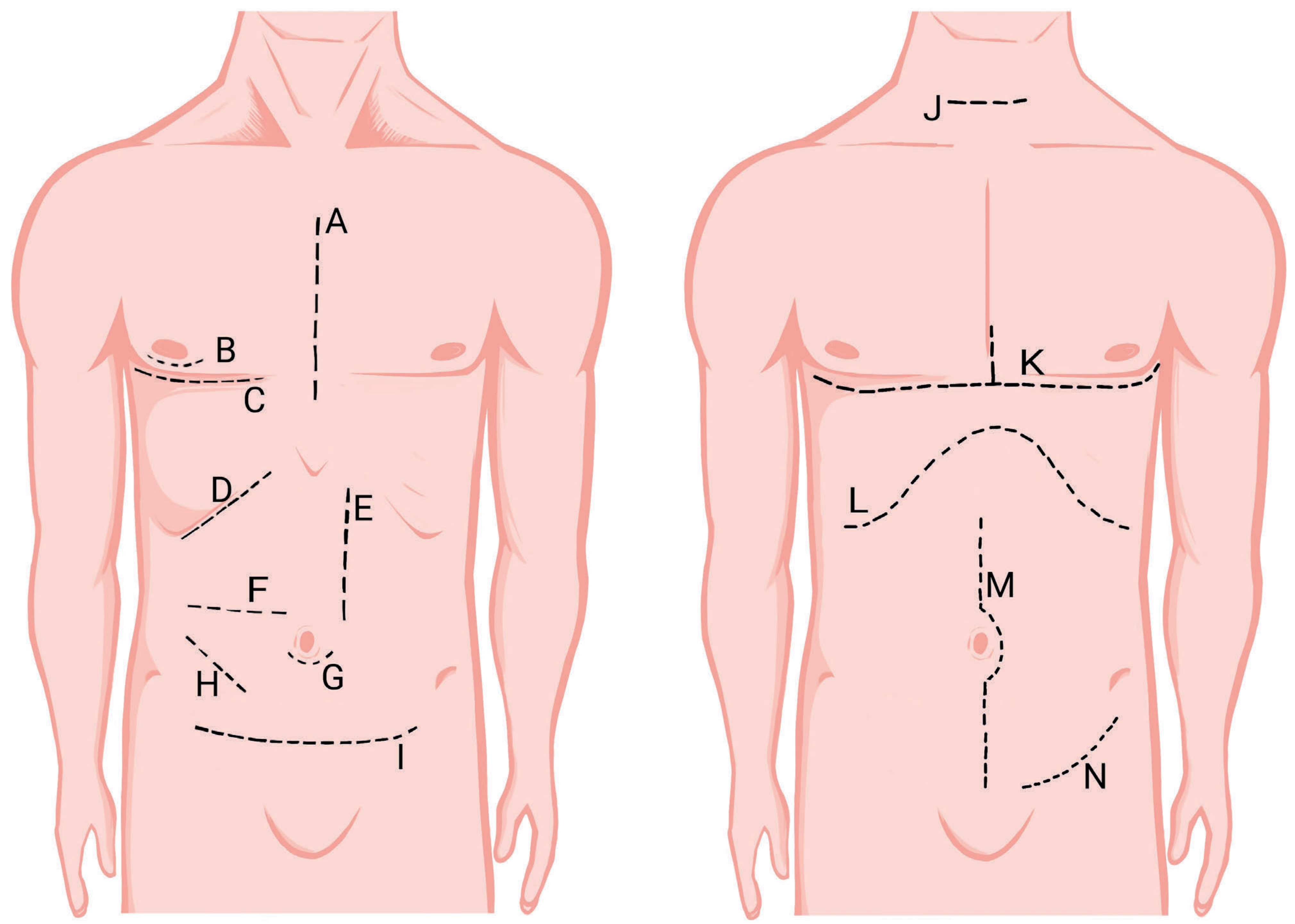
A. Longitudinal / Vertical Incisions
| Incision | Location | Use |
|---|---|---|
| Midline | Along linea alba (xiphisternum to pubis) | Most emergency laparotomies; quick and versatile |
| Paramedian | 2-3 cm lateral to midline, through rectus | Better blood supply, lower hernia rate |
| Sternotomy | Midline through sternum | Cardiac, thoracic surgery |
B. Transverse / Oblique Incisions
| Incision | Location | Use |
|---|---|---|
| Pfannenstiel | Low transverse, above pubis | Gynaecological, obstetric |
| Kocher's | Right subcostal oblique | Cholecystectomy, thyroidectomy |
| Subcostal | Below costal margin | Liver, spleen surgery |
| McBurney's | Right iliac fossa (gridiron) | Appendicectomy |
| Lanz | Transverse in right iliac fossa | Appendicectomy (better cosmesis) |
C. Combined / Special Incisions
| Incision | Notes |
|---|---|
| Chevron (rooftop) | Bilateral subcostal - liver transplant, total gastrectomy |
| Clamshell (thoracotomy) | Bilateral thoracotomy joined across sternum - trauma, lung transplant |
| Thoracoabdominal | Extends into both chest and abdomen |
| Periareolar | Around areola - breast surgery |
| Inguinal | Hernia repair, vascular groin access |
Comparison: Transverse vs. Longitudinal
- Transverse: Less pain, better pulmonary function, fewer incisional hernias - but higher wound infection rates
- Midline laparotomy: Preferred for emergencies - quicker, more versatile, easily extended
Scalpel Blades
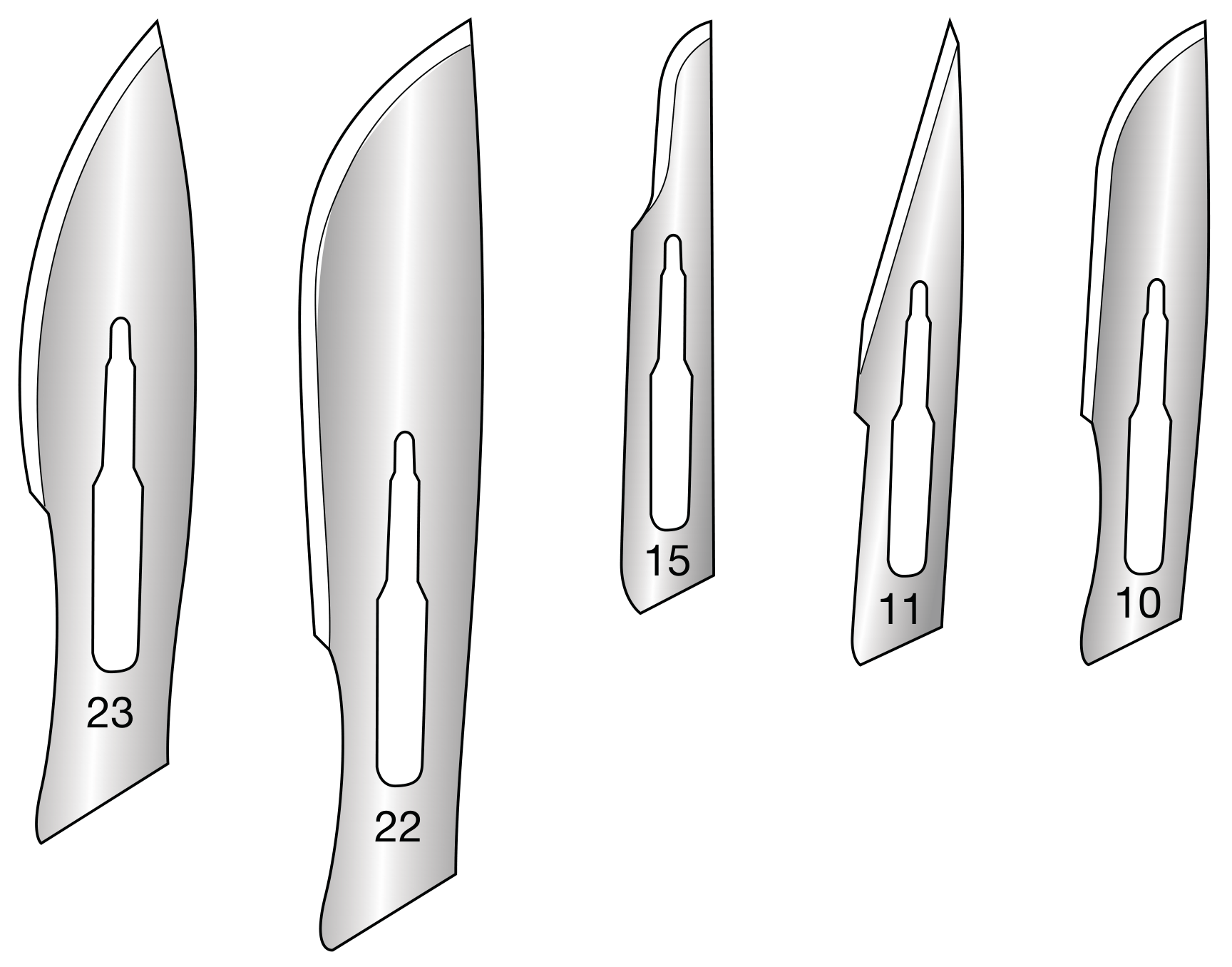
| Blade | Shape | Use |
|---|---|---|
| No. 10 | Curved, large | General skin incisions |
| No. 11 | Sharp pointed tip | Arteriotomy, abscess drainage, drain site insertion |
| No. 15 | Small curved | Minor surgical procedures, fine dissection |
| No. 22 | Curved, large | Abdominal incisions |
| No. 23 | Largest curved | Large skin incisions |
2. CLIP LIGATURES
Clip ligatures (surgical clips) are mechanical devices used to achieve haemostasis or occlude structures without sutures.
Types of Surgical Clips
| Type | Material | Use |
|---|---|---|
| Metal vascular clips (Hemoclip, Weck clip) | Titanium/stainless steel | Ligating small vessels, biliary ducts |
| Absorbable polymer clips | PLA/PGLA polymers | Vessel ligation where metal clips interfere with imaging |
| Laparoscopic clip appliers | Titanium | Cholecystectomy (cystic duct/artery), port-site bleeding |
| Michel clips / skin clips | Stainless steel | Skin closure (Michel = interrupted, Auto-clip = stapler) |
| Aneurysm clips | Titanium | Neurosurgical - intracranial aneurysm occlusion |
Key Clinical Points
- Clips provide rapid haemostasis for small vessels and are preferred in laparoscopic surgery
- Clips are NOT adequate for large vessels or high-pressure structures - suture ligatures are required for these (e.g., lumbar veins avulsed during aortic surgery; clips risk retraction and re-bleeding)
- For major vessels (e.g., renal artery/vein), a suture ligature (transfixion stitch) is used in addition to a tie to prevent slip-off
- Titanium clips are MRI-safe and do not significantly degrade imaging
Traditional Ligature
A ligature is a suture material tied around a vessel to occlude it:
- Free tie (simple ligature): Passed around vessel with forceps and tied
- Suture ligature (transfixion): Needle passed through the vessel, then tied on either side - prevents slipping, used on larger vessels
- Common material: 0 or 2-0 silk, chromic catgut, polyglactin (Vicryl)
3. SUTURES
Classification Overview
Sutures are classified by: (1) absorbability, (2) structure (mono vs. multifilament), (3) origin (natural vs. synthetic), (4) size.
A. By Absorbability
ABSORBABLE SUTURES
Lose >50% tensile strength within 2 months; degraded in tissue.
| Suture | Type | Absorption Time | Tensile Strength Half-Life | Use |
|---|---|---|---|---|
| Plain gut (catgut) | Natural, monofilament | 10-40 days | 7-10 days | Mucosal, rapidly healing wounds |
| Chromic gut | Natural, monofilament (treated with chromic salts) | 90 days | 10-14 days | GI, urological anastomoses |
| Polyglactin (Vicryl) | Synthetic, braided | 56-70 days | 3-4 weeks | Deep dermal, fascial closure |
| Vicryl Rapide | Synthetic, braided, fast-absorbing | 42 days | 5-7 days | Skin, mucosal closure |
| Polyglycolic acid (Dexon) | Synthetic, braided | 60-90 days | 2-3 weeks | Abdominal wall, fascial repair |
| Poliglecaprone (Monocryl) | Synthetic, monofilament | 90-120 days | 1-3 weeks | Subcuticular skin closure |
| Polydioxanone (PDS) | Synthetic, monofilament | 180-210 days | 6+ weeks | Fascial closure, slowly healing structures |
| Polyglyconate (Maxon) | Synthetic, monofilament | ~180 days | 6+ weeks | Fascial closure, laparotomy |
Key principle for midline laparotomy closure: Use a slowly absorbable monofilament (PDS or Maxon) - fast absorbable sutures (Vicryl) break before the fascia regains enough strength, risking dehiscence and incisional hernia (Fischer's Mastery of Surgery, 8th ed.).
NONABSORBABLE SUTURES
Retain strength indefinitely; may cause sinus formation if buried.
| Suture | Type | Properties | Use |
|---|---|---|---|
| Silk | Natural, braided | Excellent handling, high tissue reactivity | Vascular ties, skin closure; NOT for hernia repair |
| Nylon (Ethilon, Dermalon) | Synthetic, mono or braided | High memory, low reactivity | Skin closure, retention sutures |
| Polypropylene (Prolene) | Synthetic, monofilament | Very high memory, very low reactivity, permanent | Vascular anastomoses, hernia mesh fixation |
| Polyester (Ti-Cron, Mersilene) | Synthetic, braided | Low memory, very good knot strength | Cardiac surgery, tendon repair |
| Polybutester (Novafil) | Synthetic, monofilament | High memory, good knot strength | Skin closure |
| Steel (stainless) | Monofilament or twisted | Highest tensile strength, poor handling | Sternal closure, orthopaedic wire |
| Cotton | Natural, twisted | Very high tissue reactivity | Rarely used today |
B. By Structure
| Structure | Properties |
|---|---|
| Monofilament | Single strand; low capillarity, low infection risk, high memory, lower knot security (needs more throws) |
| Multifilament (braided/twisted) | Multiple strands; higher capillarity (traps bacteria), better handling, better knot security, lower memory |
C. By Suture Technique
| Technique | Description | Advantage |
|---|---|---|
| Interrupted | Individual stitches, each tied separately | If one fails, others hold; good for infected wounds |
| Simple continuous (running) | One long suture running along wound | Fast; evidence shows lower hernia rate for midline closure |
| Mattress (vertical/horizontal) | Deeper bites for tension; everts wound edges | Reduces dead space; good for skin under tension |
| Figure-of-eight | Double loop for extra strength | Fascial closure, vessel ligation |
| Subcuticular (intradermal) | Running suture buried in dermis | Excellent cosmesis, no surface marks |
| Purse-string | Circular suture tightened like a drawstring | Stoma inversion, appendix stump |
| Connell suture | Continuous inverting GI suture through all layers | GI anastomosis (inner layer) |
| Lembert suture | Interrupted inverting seromuscular suture | GI anastomosis (outer seromuscular layer) |
D. Suture Sizing (USP Scale)
- Larger number after "0" = thinner suture (e.g., 6-0 < 5-0 < 4-0)
- Larger number without "0" = thicker (e.g., 1 > 0 > 2-0 > 3-0)
- Dermatological surgery typically uses 3-0 to 6-0 (Fitzpatrick's Dermatology)
| Body site | Typical suture size |
|---|---|
| Face / eyelid | 5-0, 6-0 |
| Scalp, hand | 3-0, 4-0 |
| Trunk, extremities | 3-0, 4-0 |
| Fascia / linea alba | 0, 1 (PDS or Maxon) |
| Vascular anastomosis | 5-0 to 7-0 Prolene |
E. Wound Closure Types
| Type | Description | Indication |
|---|---|---|
| Primary (1st intention) | Wound edges approximated immediately | Clean elective wounds |
| Secondary (2nd intention) | Wound left open to granulate and epithelialise | Heavily contaminated wounds |
| Tertiary / Delayed primary | Fascia closed; skin left open initially, then closed 4-5 days later | Infected/contaminated wounds, abdominal compartment syndrome |
Barbed Sutures
A newer design in which small barbs grip tissue along the entire suture length, distributing tension without requiring a knot. Available in Vicryl, PDS, and Monocryl configurations. Increasingly used for vesico-urethral anastomosis in radical prostatectomy. (Campbell-Walsh-Wein Urology)
Sources: Bailey & Love's Short Practice of Surgery 28th ed.; Fischer's Mastery of Surgery 8th ed.; Roberts & Hedges' Clinical Procedures in Emergency Medicine; Fitzpatrick's Dermatology; Campbell-Walsh-Wein Urology; Hinman's Atlas of Urologic Surgery.
This is a shared conversation. Sign in to Orris to start your own chat.