Ameloblastoma in detail and explain in creative ways
Reading File
Finding Sources
Searching the Web
ameloblastoma pathology classification treatment 2024
Searching PubMed
ameloblastoma[MeSH Terms] AND treatment
Reading File
Reading File
Searching Images
ameloblastoma histology microscopy follicular plexiform
Reading File
Reading File
Searching Images
ameloblastoma CT scan jaw radiolucent soap bubble multilocular
I now have rich content from textbooks, images, and recent literature. Let me compile the comprehensive, creative response.
🦷 Ameloblastoma — The Jaw's Most Notorious Trickster
"The tumor that looks harmless but acts like a squatter — it'll move in slowly, refuse to leave, and keep coming back."
🌱 Origin Story: What IS an Ameloblastoma?
Ameloblastoma is the most aggressive benign odontogenic tumor of the jaws. The name comes from the Old French amel (enamel) + Greek blastos (germ) — it arises from the epithelial remnants of the enamel organ, the same tissue that builds your teeth during development. When that tissue goes rogue, it doesn't make enamel — instead, it forms an expanding, infiltrative mass that slowly devours bone.
- Incidence: ~1 in 1 million per year — rare but not negligible
- Most common location: Mandible (~85%), especially the molar-ramus region
- Peak age: Conventional type after age 20; unicystic type in the 2nd–3rd decade
- No sex predilection (affects males and females equally)
🎭 The Four Characters: WHO 2017 Classification
Think of ameloblastoma as a family of four siblings, each with a distinct personality:
| Type | Personality | Key Feature |
|---|---|---|
| Conventional (Solid/Multicystic) | The Classic Bully | Intraosseous, locally aggressive, highest recurrence |
| Unicystic | The Undercover Agent | Mimics a dentigerous cyst radiographically |
| Peripheral (Extraosseous) | The Soft-Tissue Squatter | Lives on the gingiva, no bone invasion |
| Metastasizing | The Surprise Traveller | Benign histology but metastasizes — most often to lung |
The 2017 WHO classification removed "solid/multicystic" from the conventional type name and reclassified metastasizing ameloblastoma OUT of the malignant category — because its histology is benign; it's the behavior that's surprising.
🔬 Microscopy: The Enamel Organ Reborn
Under the microscope, ameloblastoma is a masterpiece of developmental mimicry — it recreates the architecture of a developing tooth germ.
The Hallmark Architecture
Reverse polarity (a.k.a. the "piano key sign"):
- Peripheral columnar cells line the epithelial islands
- Their nuclei are pushed away from the basement membrane (toward the center of the cell) — this is the reverse of normal epithelium
- Central cells are loosely arranged, resembling stellate reticulum of the tooth bud
🎸 Histological Variants — The Band Members
| Variant | Visual Metaphor | Description |
|---|---|---|
| Follicular | 🥚 Nests of eggs | Discrete islands with peripheral palisading and stellate center |
| Plexiform | 🕸️ Spider web | Anastomosing cords and sheets in vascular stroma |
| Acanthomatous | 🧀 Swiss cheese | Squamous metaplasia with keratin pearls in the center |
| Granular cell | 🫙 Jar of marbles | Central cells packed with eosinophilic granules (lysosomes) |
| Desmoplastic | 🪨 Rocky landscape | Dense fibrous (desmoplastic) stroma; mixed lucent-opaque on X-ray |
| Basal cell | 🧱 Brick wall | Basaloid nests with minimal stellate reticulum; classic in peripheral type |
Note: Histological variant does not affect prognosis — it's the tumor type (conventional vs. unicystic vs. peripheral) and surgical margins that matter.
Histology Images:
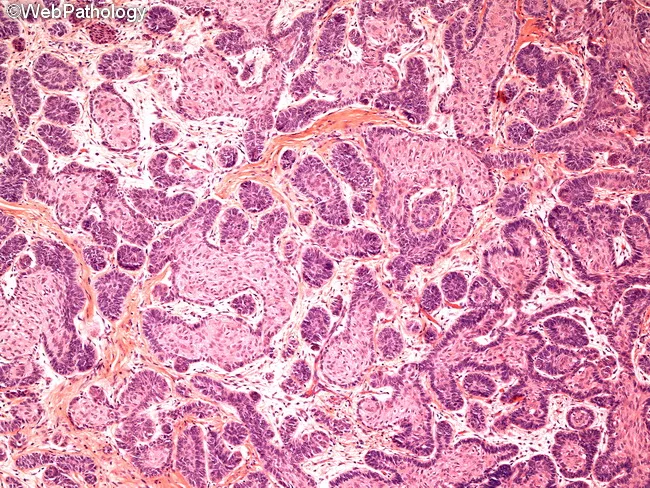
Classic ameloblastoma: follicular pattern with peripheral palisading, reverse nuclear polarity, and stellate reticulum-like center.
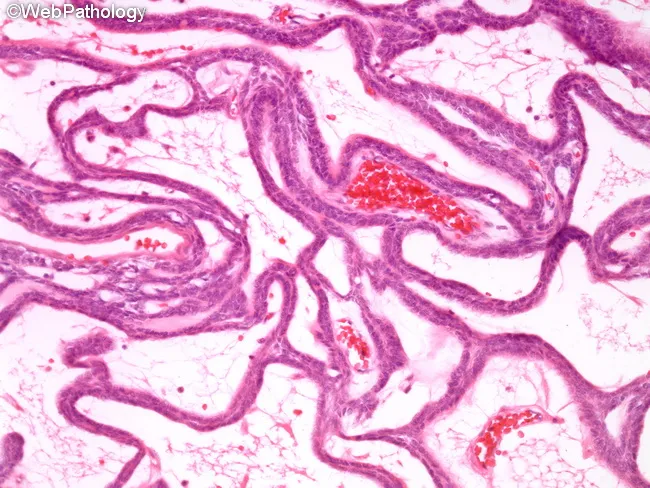
Plexiform variant: interconnected epithelial cords in a loose vascular stroma — the "spider web" pattern.
📡 Radiology: The Soap Bubble Sign
Ameloblastoma has a classic but not pathognomonic radiographic appearance:
- Multilocular radiolucency — the iconic "soap bubble" or "honeycomb" pattern
- May also appear unilocular (especially unicystic type, nearly indistinguishable from a dentigerous cyst)
- Well-demarcated borders with a sclerotic rim
- Root resorption of adjacent teeth
- Cortical expansion — buccal and lingual cortices balloon outward like a blister
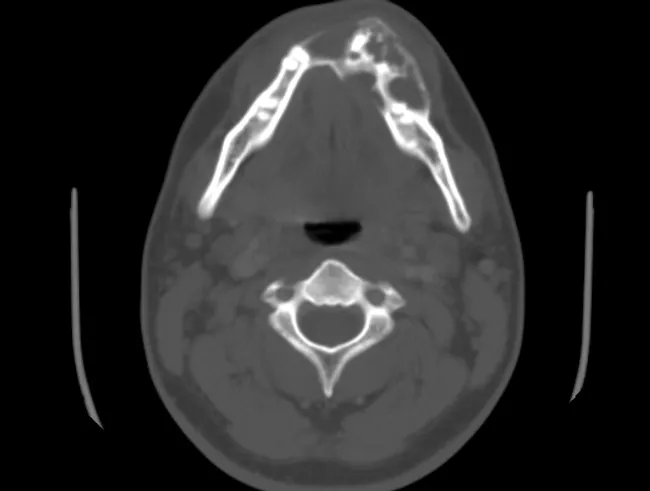
CT showing classic multilocular ameloblastoma of the mandible with cortical expansion — the "soap bubble" at its finest.

Panoramic X-ray: multilocular ameloblastoma with classic scalloped borders and "floating" displaced teeth.
🧬 Molecular Biology: The MAPK Pathway Gone Wild
In approximately 90% of all ameloblastomas, mutations in the MAPK signaling pathway have been identified — making this one of the best-understood molecular signatures in odontogenic tumors.
Key Mutations
| Gene | Frequency | Significance |
|---|---|---|
| BRAF V600E | ~63% of conventional | Most common; targetable with BRAF inhibitors |
| SMO | ~10% | Hedgehog pathway; seen in BRAF-wild type |
| RAS (KRAS/NRAS/HRAS) | ~15% | Alternative MAPK activation |
| FGFR2 | Rare | Receptor tyrosine kinase mutation |
🔑 BRAF V600E is the master key — it keeps the MAPK "gas pedal" permanently pressed, driving uncontrolled cell proliferation. The same mutation drives melanoma, papillary thyroid cancer, and hairy cell leukemia — meaning vemurafenib (a BRAF inhibitor) is now being explored for refractory/recurrent ameloblastoma.
🩺 Clinical Presentation: The Quiet Invader
Ameloblastoma earns its reputation as "the silent tumor":
- Painless jaw swelling — slow, progressive (patients may ignore it for years)
- Facial asymmetry as the tumor expands
- Loose teeth or displaced teeth (from bone destruction)
- Trismus if involving pterygoid muscles
- No paresthesia (unlike odontogenic carcinoma)
The maxillary location (~15% of cases) is particularly dangerous because the tumor can spread into the pterygoid plates, orbital floor, and pterygopalatine fissure — areas where complete surgical access is limited, so persistence there is more a problem of anatomy than tumor aggression.
🏥 Diagnosis: The Triple Approach
Panoramic X-ray ──► CT scan ──► Biopsy (histopathology)
↓ ↓ ↓
First look 3D extent Definitive Dx
Differential diagnosis (what it mimics):
- Odontogenic keratocyst (KCOT) — very similar!
- Dentigerous cyst (especially unicystic type)
- Giant cell tumor
- Ossifying fibroma
- Myxoma
- Central mucoepidermoid carcinoma (for desmoplastic type)
⚔️ Treatment: The Great Debate
Ameloblastoma has no single perfect treatment — it has been debated for decades. Here's the battlefield:
Conservative vs. Radical Surgery
| Approach | Method | Recurrence Rate | Use When |
|---|---|---|---|
| Enucleation/Curettage | Scoop it out | ⚠️ 60–80% | Almost never recommended for conventional type |
| Marginal Resection | Remove tumor + 1 cm clear margin | 10–20% | Small conventional lesions; all unicystic mural |
| Segmental Resection | Remove jaw segment entirely | <5% | Large conventional lesions |
| Hemimandibulectomy | Half the mandible | <5% | Extensive disease |
The 1 cm rule: Most surgeons favor resection extending 1 cm past the radiographic edge of the tumor — because ameloblastoma microscopically infiltrates beyond its visible borders.
Reconstruction After Surgery
After segmental jaw resection, reconstruction is essential:
- Free fibula flap — most common choice; provides vascularized bone
- Iliac crest graft
- Titanium plate + secondary bone graft
- Dental implants can be placed later
Targeted Therapy: The New Frontier
For recurrent/unresectable disease with confirmed BRAF V600E:
- Vemurafenib / Dabrafenib (BRAF inhibitors) — evidence accumulating for jaw preservation before surgery
- Trametinib (MEK inhibitor) — used in combination for melanoma; being explored for ameloblastoma
- Response is slow (weeks to months) due to the tumor's inherent slow growth and bone metabolism — but this allows a jaw-preservation strategy in selected cases
📊 Prognosis: The Long Game
| Type | Recurrence Rate | Notes |
|---|---|---|
| Conventional (after resection) | <5% | With adequate margins |
| Conventional (after curettage) | 60–80% | High — why resection is preferred |
| Unicystic luminal/intraluminal | 10–20% | Conservative treatment acceptable |
| Unicystic mural | ~25% | Behaves like conventional — needs resection |
| Peripheral | 15–20% | After excision |
| Metastasizing | Variable | Slow — may not need aggressive treatment |
Lifelong surveillance is mandatory — recurrences can appear 5, 10, even 20 years after initial surgery. Minimum follow-up: 5 years with annual imaging.
☠️ When It Turns Bad: Malignant Forms
Two distinct malignant entities:
1. Malignant Ameloblastoma
- Benign histology (no cytological atypia) but metastasizes — classically to the lung and cervical lymph nodes
- Often delayed metastases — decades after the primary
- Treatment: surgical resection (1–2 cm margins); no chemo/radiotherapy generally needed
- Recent WHO 2017 reclassified this into the benign spectrum since histology is benign
2. Ameloblastic Carcinoma
- Malignant histology (high mitoses, nuclear pleomorphism, necrosis, perineural invasion) + aggressive behavior
- SOX2 overexpression — a potential marker for malignant transformation
- Treatment: resection with 2–3 cm margins + concurrent chemoradiotherapy for positive margins
- Worse prognosis — lymph node and distant metastases possible
🔍 Unicystic Ameloblastoma: The Undercover Case
"It comes disguised as a dentigerous cyst. Your radiograph says cyst. Your biopsy says something far more interesting."
Unicystic ameloblastoma accounts for ~15% of all ameloblastomas and is the great mimicker:
Three Subtypes (Vickers and Gorlin criteria):
- Luminal — ameloblastomatous lining on the cyst wall's luminal surface only → conservative treatment
- Intraluminal — nodule projects INTO the cyst lumen → conservative treatment
- Mural — tumor infiltrates the fibrous wall → treat like conventional ameloblastoma (resection!)
Histological hallmarks (Vickers-Gorlin):
- Columnar basal cells
- Palisading of basilar cells
- Reverse nuclear polarity
- Hyperchromatic basal nuclei
- Sub-nuclear vacuolization
- Loosely arranged stellate cells above the basal layer
💡 Creative Memory Tricks
🎯 "SPRAM" — The Ameloblastoma Checklist
- Slow-growing but locally aggressive
- Painless jaw swelling
- Radiolucent (soap bubble/honeycomb)
- Ameloblastic pattern (reverse polarity, stellate reticulum)
- MAPKK pathway mutations (BRAF V600E most common)
🏗️ Visualizing the Histology
Think of a follicular ameloblastoma island as a deviled egg:
- The outer ring = peripheral columnar cells (the egg white border) with nuclei pointing INWARD
- The center = loosely arranged stellate cells (the yolk)
- Multiple deviled eggs embedded in dense fibrous tissue = the classic picture
📚 Textbook Sources
- K.J. Lee's Essential Otolaryngology, p. 758
- Cummings Otolaryngology Head and Neck Surgery, Ch. 88
🔬 Recent Literature
Three recent systematic reviews (2023–2024) highlight emerging areas:
- Adenoid ameloblastoma is a newly recognized entity (PMID: 37540485) — systematic review confirming distinct clinicopathologic features
- Papilliferous keratoameloblastoma — ultra-rare variant reviewed (PMID: 37655071)
- Ameloblastic carcinoma — a 2024 systematic review (PMID: 38368851) confirms its aggressive behavior and need for wide margins
⚡ Quick-Fire Summary
| Feature | Key Point |
|---|---|
| Type | Benign but locally aggressive odontogenic tumor |
| Origin | Enamel organ epithelial remnants |
| Location | 85% mandible, molar-ramus region |
| Radiology | Soap bubble / honeycomb multilocular radiolucency |
| Histology | Peripheral palisading + reverse polarity + stellate reticulum |
| Molecular | BRAF V600E in ~63%, SMO, RAS mutations |
| Treatment | Surgical resection with 1 cm margins (gold standard) |
| Recurrence | 60–80% with curettage; <5% with resection |
| Malignant forms | Malignant ameloblastoma (benign histo + mets) vs. ameloblastic carcinoma (malignant histo) |
| Follow-up | Lifelong — recurrences possible decades later |
This is a shared conversation. Sign in to Orris to start your own chat.