# HISTOLOGY OF ORGANS ASSOCIATED WITH THE DIGESTIVE TRACT
## A Comprehensive and Detailed Guide
---
# 1. SALIVARY GLANDS
The major salivary glands are three paired organs: the **parotid**, **submandibular (submaxillary)**, and **sublingual** glands. Additionally, numerous **minor salivary glands** are scattered throughout the oral mucosa (labial, buccal, lingual, palatine).
---
## GENERAL STRUCTURAL PLAN OF SALIVARY GLANDS
All major salivary glands share a common organizational pattern:
### Capsule and Stroma
- Each gland is surrounded by a **connective tissue capsule** (dense irregular connective tissue).
- **Septa** extend inward from the capsule, dividing the gland into **lobes** and **lobules**.
- The septa carry **blood vessels, lymphatics, nerves**, and **excretory ducts**.
- The connective tissue stroma contains **fibroblasts, mast cells, macrophages, plasma cells**, and **adipocytes** (especially prominent in the parotid gland with aging).
### Parenchyma
The parenchyma consists of:
1. **Secretory end pieces (acini/tubules)**
2. **Duct system**
---
## SECRETORY END PIECES
### A. Serous Acini
- **Shape**: Spherical, with a small central lumen.
- **Cell shape**: Pyramidal cells arranged around the lumen.
- **Nucleus**: Round, basally located.
- **Cytoplasm**:
- **Basal portion**: Intensely basophilic due to abundant **rough endoplasmic reticulum (rER)** — responsible for protein (enzyme) synthesis.
- **Apical portion**: Filled with **secretory (zymogen) granules** that are PAS-positive and eosinophilic. These granules contain **α-amylase (ptyalin)**, **lysozyme**, **lactoferrin**, and **secretory IgA**.
- Well-developed **Golgi apparatus** supranuclear in position.
- Numerous **mitochondria** scattered throughout.
- **Secretory product**: Thin, watery, enzyme-rich (serous) fluid.
- **Intercellular secretory canaliculi**: Small channels between adjacent serous cells that extend toward the lumen, increasing the secretory surface area.
### B. Mucous Acini (Tubules)
- **Shape**: Tubular, larger than serous acini, with a wider, more obvious lumen.
- **Cell shape**: Columnar to pyramidal.
- **Nucleus**: Flattened, compressed against the base of the cell by accumulated mucin (mucinogen) granules.
- **Cytoplasm**: Appears pale and foamy in H&E sections because mucin is extracted during histological processing. With **PAS staining** or **mucicarmine**, the mucin granules stain intensely.
- **Secretory product**: Thick, viscous, glycoprotein-rich mucus (mainly **MUC5B** and **MUC7** mucins).
### C. Serous Demilunes (of Gianuzzi/von Ebner)
- **Definition**: Crescent-shaped caps of serous cells that sit on the outside of mucous acini.
- **Classic interpretation**: Serous cells that could not fit around the lumen directly, so they form a "half-moon" over the mucous tubule.
- **Modern interpretation (rapid-freeze fixation studies)**: Serous demilunes may be an **artifact of fixation**. In vivo, serous cells are likely arranged alongside mucous cells rather than capping them. The mucous cells swell during conventional fixation, pushing serous cells peripherally.
- **Secretory canaliculi**: Even in the demilune arrangement, intercellular canaliculi pass between mucous cells to reach the lumen, allowing serous secretions access to the duct system.
### D. Myoepithelial (Basket) Cells
- Located between the **basal lamina** and the **basal surface** of secretory cells and intercalated duct cells.
- **Shape**:
- On acini: Stellate/spider-like with long branching processes (basket cells).
- On intercalated ducts: More elongated, spindle-shaped.
- **Cytoplasm**: Contains **actin and myosin filaments** (hence "myo-epithelial") — they are contractile.
- **Function**: Their contraction squeezes secretory end pieces and small ducts, aiding in expulsion of secretory products into the duct system. They also help maintain the structural integrity of the acinus and may play a role in resisting elevated intraluminal pressure during secretion.
- **Immunohistochemistry**: Positive for **smooth muscle actin (SMA)**, **calponin**, **p63**, **cytokeratin 14 (CK14)**, and **S-100 protein**.
> **CLINICAL: Myoepithelial cells and tumors**
> Myoepithelial cells are the cell of origin of **myoepitheliomas** and are a significant component of **pleomorphic adenomas (mixed tumors)** of salivary glands — the most common salivary gland tumor. In pleomorphic adenomas, myoepithelial cells can produce the characteristic **chondromyxoid stroma**. Immunohistochemistry for SMA, p63, calponin, and S-100 helps identify the myoepithelial component in salivary gland tumors.
---
## DUCT SYSTEM
The duct system progressively modifies the primary secretion produced by the acini.
### 1. Intercalated Ducts
- **Location**: Immediately connect to the secretory end pieces.
- **Epithelium**: Simple **cuboidal** (low cuboidal) or **squamous** epithelium.
- **Lumen**: Very narrow.
- **Cells**: Small cells with relatively little cytoplasm, central round nuclei.
- **Myoepithelial cells**: Present around these ducts.
- **Function**: Add **bicarbonate** and **water** to the primary secretion; contain **stem/progenitor cells** that can regenerate both acinar and duct cells.
- **Length**: Longest and most prominent in the **parotid**; shortest (and fewest) in the **sublingual**.
> **CLINICAL: Intercalated duct cells as progenitors**
> These cells are believed to be the progenitor cells of the gland. They can give rise to both acinar cells and striated duct cells. **Intercalated duct hyperplasia** and **intercalated duct carcinoma** (a low-grade salivary gland carcinoma) arise from these cells.
### 2. Striated Ducts (Secretory Ducts/Intralobular Ducts)
- **Location**: Continuation of intercalated ducts; located within lobules.
- **Epithelium**: Simple **columnar** epithelium.
- **Cells**: Tall, eosinophilic columnar cells.
- **Key feature — Basal striations**:
- Caused by deep **infoldings of the basal plasma membrane** with numerous **elongated mitochondria** aligned perpendicular to the basement membrane between the folds.
- This arrangement is identical to the basal striations seen in the **proximal convoluted tubule** of the kidney and is characteristic of cells involved in **active ion transport**.
- **Function**: **Modification of saliva**:
- **Reabsorb Na⁺ and Cl⁻** from the primary secretion.
- **Secrete K⁺ and HCO₃⁻** into the lumen.
- The net effect is that saliva becomes **hypotonic** relative to plasma.
- Also secrete **kallikrein** (which produces bradykinin from kininogen, causing vasodilation), **EGF (epidermal growth factor)**, **lysozyme**, and **IgA**.
- **Length**: Longest and most prominent in the **submandibular** gland; shortest in the **sublingual**.
- **Myoepithelial cells**: Generally absent around striated ducts.
### 3. Excretory (Interlobular) Ducts
- **Location**: In the connective tissue septa between lobules.
- **Epithelium**: Initially **pseudostratified columnar**; becomes **stratified columnar** as ducts increase in size.
- **Goblet cells**: Occasionally present.
- **Function**: Primarily conduit; some continued modification of saliva.
- As ducts approach the oral cavity, the epithelium transitions to **stratified squamous** epithelium (continuous with the oral epithelium).
### 4. Main Excretory Duct
- **Parotid → Stensen's duct** (opens opposite the second upper molar).
- **Submandibular → Wharton's duct** (opens at the sublingual caruncle on the floor of the mouth).
- **Sublingual → Bartholin's duct** (main) and numerous **Rivinus ducts**.
- Epithelium: **Stratified squamous** near the orifice.
---
## INDIVIDUAL SALIVARY GLANDS
### I. PAROTID GLAND
- **Location**: Anterior and inferior to the ear; superficial and deep to the ramus of the mandible.
- **Type of gland**: **Purely serous** (in humans).
- **Secretory end pieces**: All serous acini. No mucous acini or serous demilunes.
- **Duct system**:
- **Intercalated ducts**: Very **long** and prominent.
- **Striated ducts**: Present but **shorter** than in the submandibular.
- **Stroma**: Contains significant amounts of **adipose tissue** (fat cells) within the connective tissue, which **increases with age**. This is a key identifying feature — in aged individuals, the parenchyma may be largely replaced by fat.
- **Important anatomical relationship**: The **facial nerve (CN VII)** passes through the substance of the parotid gland, dividing it into superficial and deep lobes.
- **Serous secretion**: Rich in **amylase (ptyalin)**, proline-rich proteins, and water.
> **CLINICAL: Mumps (Epidemic Parotitis)**
> Caused by the **paramyxovirus (Mumps virus)**. Primarily affects the parotid gland causing painful bilateral (or unilateral) swelling. Can also affect the submandibular and sublingual glands. Complications include **orchitis** (inflammation of the testes, can cause sterility), **oophoritis**, **pancreatitis**, and **meningoencephalitis**. Histologically: lymphocytic infiltration, edema of the interstitium, and degeneration of acinar cells.
> **CLINICAL: Pleomorphic Adenoma (Mixed Tumor)**
> The **most common salivary gland tumor** (60-70% of all salivary gland tumors). Most common in the **parotid** (80%). Benign but has a tendency for **local recurrence** if incompletely excised. Histologically: mixture of epithelial elements (ductal structures, myoepithelial cells) and mesenchymal-like elements (chondroid, myxoid, osseous stroma — all produced by myoepithelial cells).
> **CLINICAL: Warthin's Tumor (Papillary Cystadenoma Lymphomatosum)**
> Second most common benign parotid tumor. Almost exclusively in the **parotid**. Strong association with **smoking**. More common in males. Can be **bilateral** (10-15%). Histologically: **double layer of eosinophilic (oncocytic) epithelial cells** lining papillary cystic spaces, supported by a **dense lymphoid stroma with germinal centers**. The oncocytic cells are packed with mitochondria (hence the eosinophilia).
> **CLINICAL: Mucoepidermoid Carcinoma**
> The **most common malignant** salivary gland tumor. Most common in the parotid. Contains a mixture of **mucous cells, epidermoid (squamous) cells, and intermediate cells**. Graded as low, intermediate, or high grade. Low-grade tumors have a good prognosis; high-grade tumors behave aggressively.
> **CLINICAL: Adenoid Cystic Carcinoma (Cylindroma)**
> A malignant tumor known for **perineural invasion** (spreads along nerves) and **late distant metastases** (especially to the lungs). Most common malignant tumor of the **minor salivary glands** and the **submandibular gland**. Histologically: characteristic **cribriform (Swiss cheese) pattern** with pseudocystic spaces filled with basophilic mucoid material or reduplicated basal lamina.
> **CLINICAL: Sjögren's Syndrome**
> An **autoimmune** disease characterized by **dry mouth (xerostomia)** and **dry eyes (keratoconjunctivitis sicca)** due to lymphocytic infiltration and destruction of salivary and lacrimal glands. Histologically: **periductal and periacinar lymphocytic infiltration** with formation of **lymphoid follicles with germinal centers** — the so-called **"lymphoepithelial lesions"** (lymphocytes infiltrating duct epithelium, forming epimyoepithelial islands). Associated with **anti-Ro (SS-A)** and **anti-La (SS-B)** antibodies. Increased risk of **B-cell lymphoma (MALT lymphoma / marginal zone lymphoma)** — 40-fold increased risk.
> **CLINICAL: Sialolithiasis (Salivary Stones)**
> Most commonly affects the **submandibular gland** (80-90%) because Wharton's duct is long, courses upward against gravity, and submandibular secretion is more viscous (mixed serous and mucous) and has higher calcium and phosphate content. Stones cause obstruction, leading to pain and swelling during eating. Can lead to **sialadenitis** (inflammation of the salivary gland).
> **CLINICAL: Frey's Syndrome (Gustatory Sweating)**
> Occurs after parotid surgery. The **auriculotemporal nerve** (which carries parasympathetic secretomotor fibers to the parotid) is damaged during surgery. During regeneration, parasympathetic nerve fibers aberrantly reinnervate the **sweat glands of the overlying skin**. This causes sweating and flushing of the skin overlying the parotid during eating.
### II. SUBMANDIBULAR (SUBMAXILLARY) GLAND
- **Location**: In the submandibular triangle (floor of the mouth).
- **Type of gland**: **Mixed**, predominantly **serous** (~80% serous, ~20% mucous).
- **Secretory end pieces**:
- Mostly **serous acini**.
- Some **mucous tubules** capped by **serous demilunes**.
- Some purely serous acini.
- **Duct system**:
- **Intercalated ducts**: Shorter than in the parotid.
- **Striated ducts**: Very **long** and prominent — **longest** of all three major glands. This is a key distinguishing feature.
- **Less adipose tissue** in the stroma compared to the parotid.
### III. SUBLINGUAL GLAND
- **Location**: In the floor of the mouth, beneath the mucous membrane.
- **Type of gland**: **Mixed**, predominantly **mucous**.
- **Secretory end pieces**:
- Mostly **mucous tubules** with occasional **serous demilunes**.
- Very few purely serous acini.
- **Duct system**:
- **Intercalated ducts**: Very **short** or **absent**.
- **Striated ducts**: Very **short** or **poorly developed**.
- **Capsule**: Poorly defined (no well-developed capsule, unlike the parotid and submandibular).
> **CLINICAL: Ranula**
> A type of **mucocele** (mucus extravasation or retention cyst) that occurs in the floor of the mouth, usually associated with the sublingual gland or minor salivary glands. It presents as a blue, translucent swelling. A **plunging ranula** extends through the mylohyoid muscle into the neck.
---
## SUMMARY TABLE: MAJOR SALIVARY GLANDS
| Feature | Parotid | Submandibular | Sublingual |
|---|---|---|---|
| Secretory type | Purely serous | Mixed (serous predominant) | Mixed (mucous predominant) |
| Serous demilunes | Absent | Present | Present |
| Intercalated ducts | Longest | Intermediate | Short/absent |
| Striated ducts | Intermediate | Longest | Short/absent |
| Adipose tissue | Abundant (increases with age) | Less | Minimal |
| Capsule | Well-defined | Well-defined | Poorly defined |
| Most common tumor location | Most tumors arise here | Adenoid cystic carcinoma | — |
---
## MINOR SALIVARY GLANDS
- Scattered throughout the **oral mucosa**: lips, cheeks, palate, tongue, pharynx.
- Mostly **mucous** (except **von Ebner's glands** — purely serous glands in the tongue that open into the troughs of **circumvallate papillae** and **foliate papillae**).
- **No capsule**; embedded directly in the lamina propria or submucosa.
- Short or absent intercalated and striated ducts.
- **Von Ebner's glands** produce a watery secretion that flushes the taste bud troughs, allowing new tastants to reach the taste buds. They also secrete **lingual lipase**.
> **CLINICAL: Minor salivary gland tumors**
> Although less common overall, the **hard palate** is the most common site of minor salivary gland tumors. Approximately **50% of minor salivary gland tumors are malignant** (compared to only 15-30% for parotid tumors). **Adenoid cystic carcinoma** is the most common malignant tumor of minor salivary glands.
---
## SALIVA — COMPOSITION AND CONTROL
### Composition
- **99.5% water**.
- **Electrolytes**: Na⁺, K⁺, Cl⁻, HCO₃⁻, Ca²⁺, PO₄³⁻ (concentrations are modified by striated ducts).
- **Enzymes**: α-amylase (ptyalin), lingual lipase (from von Ebner's glands), lysozyme, peroxidase, kallikrein.
- **Immunoglobulins**: Secretory **IgA** (the predominant immunoglobulin — provides mucosal immunity). Produced by **plasma cells** in the stroma; the IgA dimer binds to the **polymeric Ig receptor (secretory component)** on the basolateral surface of acinar/ductal cells, is transcytosed, and released with the secretory component into the lumen.
- **Mucins**: MUC5B and MUC7 (from mucous cells).
- **Other proteins**: Proline-rich proteins (bind Ca²⁺ and tannins), histatins (antifungal), statherin (inhibits hydroxyapatite precipitation), cystatins.
- **Growth factors**: EGF, NGF.
### Innervation and Control
- **Parasympathetic** stimulation (via CN VII for submandibular and sublingual; CN IX for parotid):
- Produces **copious, watery** saliva.
- Neurotransmitter: **Acetylcholine** acting on **muscarinic (M3) receptors**.
- Also causes vasodilation (via VIP and NO) → increased blood flow to the glands.
- **Sympathetic** stimulation (via superior cervical ganglion):
- Produces **small volume, thick, viscous, protein-rich** saliva.
- Neurotransmitter: **Norepinephrine** acting on **β-adrenergic receptors** (promotes exocytosis of secretory granules).
- α-adrenergic stimulation causes vasoconstriction → reduced blood flow.
> **CLINICAL: Xerostomia (Dry Mouth)**
> Causes: Sjögren's syndrome, radiation therapy for head/neck cancers (causes **acinar atrophy and fibrosis — irreversible if dose exceeds 40 Gy**), medications (anticholinergics, antihistamines, antidepressants, diuretics), aging, mouth breathing, dehydration. Consequences: increased dental caries, oral candidiasis, difficulty swallowing and speaking, altered taste.
---
# 2. PANCREAS
The pancreas is a **retroperitoneal organ** (except for the tail, which is intraperitoneal). It has both **exocrine** (~98-99% of the mass) and **endocrine** (~1-2% of the mass) components.
---
## CAPSULE AND GENERAL ORGANIZATION
- Covered by a **thin connective tissue capsule** (but not as well-defined as some other organs).
- **Septa** extend inward, incompletely dividing the gland into **lobules**.
- The septa carry blood vessels, lymphatics, nerves, and excretory ducts.
- **No muscularis mucosae or submucosa** — the pancreas is NOT a hollow organ.
---
## EXOCRINE PANCREAS
The exocrine pancreas is a **compound acinar gland** — the **largest** purely serous gland in the body (the parotid is also purely serous but smaller).
### Serous Acini
- **Shape**: Roughly spherical, with a narrow lumen.
- **Cells**: Pyramidal serous cells arranged around the lumen.
- **Nucleus**: Round, basally located.
- **Cytoplasm**:
- **Basal portion**: Intensely **basophilic** (deep blue/purple with H&E) due to extensive **rER** — reflects the enormous protein (enzyme) synthetic capacity.
- **Apical portion**: Filled with large, round, eosinophilic **zymogen granules** (secretory granules). These are membrane-bound granules containing the **inactive precursors (zymogens)** of digestive enzymes.
- **Well-developed Golgi apparatus**: Located between the nucleus and the apical surface (supranuclear).
- **Abundant mitochondria**.
- **Lumen**: Very small.
- **No myoepithelial cells**: Unlike salivary glands, the pancreas has **no myoepithelial cells**.
### Zymogen Granule Contents (Pancreatic Enzymes)
The pancreas produces about **1.5 liters** of enzyme-rich, alkaline fluid daily.
| Enzyme (Zymogen form) | Active form | Function |
|---|---|---|
| Trypsinogen | Trypsin | Protein digestion (endopeptidase); activates other zymogens |
| Chymotrypsinogen | Chymotrypsin | Protein digestion (endopeptidase) |
| Proelastase | Elastase | Digests elastin |
| Procarboxypeptidase A & B | Carboxypeptidase A & B | Exopeptidases |
| Prophospholipase A₂ | Phospholipase A₂ | Fat digestion |
| Pancreatic lipase | (secreted active) | Fat digestion (with colipase) |
| Colipase | (secreted as procolipase) | Anchors lipase to lipid droplet |
| Pancreatic α-amylase | (secreted active) | Starch digestion |
| DNase | (secreted active) | Nucleic acid digestion |
| RNase | (secreted active) | Nucleic acid digestion |
**Key point**: Most enzymes are secreted as **inactive zymogens** to prevent autodigestion of the pancreas. **Enterokinase (enteropeptidase)**, a brush border enzyme of duodenal enterocytes, converts **trypsinogen → trypsin**. Trypsin then activates all other zymogens (**trypsin cascade**).
**Protective mechanisms against autodigestion**:
1. Enzymes stored as inactive zymogens in membrane-bound granules.
2. **Pancreatic secretory trypsin inhibitor (PSTI / SPINK1)** — co-packaged with zymogens; inhibits any prematurely activated trypsin within the gland.
3. Segregation of enzymes in membrane-bound compartments away from the cytoplasm.
4. Lysosomal enzymes can degrade any inappropriately activated enzymes.
> **CLINICAL: Acute Pancreatitis**
> Caused by premature intrapancreatic activation of trypsinogen → trypsin, leading to autodigestion of the pancreas. Most common causes: **gallstones** (impacted at the ampulla of Vater, causing reflux of bile into the pancreatic duct) and **alcohol** (causes increased secretion with decreased flow, protein precipitation in ducts). Histologically: **coagulative necrosis of acinar cells, fat necrosis (saponification — calcium + fatty acids = chalky white deposits), hemorrhage, acute inflammation (neutrophilic infiltrate), and edema**. Clinically: severe epigastric pain radiating to the back, elevated serum **amylase** and **lipase** (lipase is more specific). Complications: pseudocyst, abscess, ARDS, DIC, hypocalcemia (from fat saponification).
> **CLINICAL: Chronic Pancreatitis**
> Most commonly caused by **chronic alcohol abuse** (70-80% of cases). Histologically: **fibrosis, atrophy of acinar tissue, chronic inflammation (lymphocytes, macrophages), calcifications within ducts, and relative preservation of islets of Langerhans** (endocrine function is preserved until late). Eventually leads to **pancreatic exocrine insufficiency** (maldigestion, steatorrhea, fat-soluble vitamin deficiency) and, in late stages, **diabetes mellitus** (when islets are finally destroyed).
> **CLINICAL: Mutations in SPINK1 (PSTI) and PRSS1 (cationic trypsinogen)**
> Mutations in **PRSS1** (hereditary pancreatitis — autosomal dominant) cause trypsin to resist inactivation. Mutations in **SPINK1** lower the threshold for pancreatitis from other causes. Both increase risk of **pancreatic adenocarcinoma**.
### Centroacinar Cells
- **THE MOST DISTINCTIVE histological feature of the pancreatic acinus** — unique to the pancreas; not found in salivary glands.
- **Definition**: These are the terminal cells of the intercalated duct that extend INTO the lumen of the acinus.
- **Appearance**:
- Pale-staining, small, flattened cells visible in the center of the acinus (hence "centro-acinar").
- Pale (lightly eosinophilic or almost clear) cytoplasm.
- Relatively large, round, centrally placed nucleus.
- Very few organelles — no secretory granules, minimal rER.
- **Function**: Along with intercalated duct cells, they secrete a **watery, bicarbonate-rich fluid** that:
- Alkalinizes the pancreatic juice (pH ~8.0).
- Neutralizes gastric acid entering the duodenum.
- Is stimulated by **secretin** (released from S cells of the duodenal mucosa in response to acid).
- Contains the enzyme **carbonic anhydrase**, which generates HCO₃⁻.
- The **CFTR chloride channel** on the apical membrane of centroacinar and ductal cells secretes Cl⁻ into the lumen, which is then exchanged for HCO₃⁻ via a **Cl⁻/HCO₃⁻ exchanger**.
> **CLINICAL: Cystic Fibrosis (CF)**
> Caused by mutations in the **CFTR gene** (chromosome 7; most common mutation: **ΔF508**). In the pancreas, defective CFTR leads to decreased Cl⁻ (and therefore HCO₃⁻ and water) secretion. The pancreatic juice becomes thick, viscous, and protein-concentrated. This causes **obstruction of pancreatic ducts → acinar atrophy → fibrosis → cystic dilatation of ducts (hence "cystic fibrosis")**. Results in **pancreatic exocrine insufficiency** (steatorrhea, malabsorption) in ~85-90% of CF patients. Histologically: ducts are dilated and filled with inspissated eosinophilic secretions; acini are atrophic and replaced by fibrosis; islets are usually preserved initially.
### Duct System of the Exocrine Pancreas
**1. Intercalated Ducts**
- Begin at the centroacinar cells.
- **Epithelium**: Simple low cuboidal/squamous.
- **Very long** (longer than those of salivary glands).
- **Function**: Secrete bicarbonate-rich fluid (like centroacinar cells).
- Stimulated by **secretin**.
**2. Intralobular Ducts**
- Receive intercalated ducts within lobules.
- Simple cuboidal to low columnar epithelium.
- Surrounded by a small amount of connective tissue.
**Important difference from salivary glands**: The pancreas has **NO STRIATED DUCTS**. This is because the primary secretion of the pancreas is already isotonic and does not need to be made hypotonic (unlike saliva).
**3. Interlobular Ducts**
- Located in connective tissue septa.
- **Epithelium**: Simple columnar; some goblet cells.
- Surrounded by more substantial connective tissue.
**4. Main Pancreatic Duct (Duct of Wirsung)**
- Runs the length of the gland from tail to head.
- Joins the **common bile duct** to form the **hepatopancreatic ampulla (Ampulla of Vater)**, which opens into the duodenum at the **major duodenal papilla**.
- Surrounded by smooth muscle — **sphincter of Oddi**.
- **Epithelium**: Tall columnar with goblet cells.
**5. Accessory Pancreatic Duct (Duct of Santorini)**
- Drains the upper part of the head.
- Opens at the **minor duodenal papilla**.
> **CLINICAL: Pancreatic Ductal Adenocarcinoma (PDAC)**
> The most common pancreatic malignancy (~85% of pancreatic cancers). **60-70%** arise in the **head** of the pancreas. Arises from the **ductal epithelium** (not acinar cells). **Precursor lesion**: **PanIN** (Pancreatic Intraepithelial Neoplasia) — graded 1, 2, 3. Key mutations: **KRAS** (>90% — the earliest and most common), **p16/CDKN2A** (95%), **TP53** (75%), **SMAD4/DPC4** (55%). When in the head, causes **obstructive jaundice** (compresses the common bile duct), **Courvoisier's sign** (painless palpable gallbladder with jaundice), and **Trousseau's syndrome** (migratory thrombophlebitis — paraneoplastic). Histologically: moderately to poorly differentiated glandular structures embedded in an intensely **desmoplastic stroma**. Prognosis is dismal: 5-year survival < 10%.
> **CLINICAL: Annular Pancreas**
> A developmental anomaly in which a ring of pancreatic tissue encircles the **second part of the duodenum**, potentially causing duodenal obstruction. Results from failure of the ventral pancreatic bud to rotate properly.
> **CLINICAL: Pancreas Divisum**
> The most common congenital anomaly of the pancreas (~5-10% of the population). Results from failure of fusion of the dorsal and ventral pancreatic ducts. The majority of the pancreas (body and tail) drains through the **accessory duct (of Santorini)** and the minor papilla. Can predispose to **recurrent pancreatitis** due to inadequate drainage through the small minor papilla.
### Regulation of Exocrine Pancreatic Secretion
| Stimulus | Source | Target | Effect |
|---|---|---|---|
| **Secretin** | S cells of duodenal mucosa (stimulated by acid, pH < 4.5) | Centroacinar and intercalated duct cells | Watery, HCO₃⁻-rich secretion (increases volume, alkalinizes) |
| **CCK (Cholecystokinin)** | I cells of duodenal mucosa (stimulated by fats and amino acids/peptides) | Acinar cells | Enzyme-rich secretion (stimulates exocytosis of zymogen granules) |
| **Acetylcholine (Vagal)** | Parasympathetic nerve endings | Acinar cells and duct cells | Potentiates both enzyme and HCO₃⁻ secretion |
---
## ENDOCRINE PANCREAS — ISLETS OF LANGERHANS
### General Features
- **Scattered throughout the pancreatic parenchyma** — approximately **1-2 million islets** in the human pancreas.
- More numerous in the **tail** of the pancreas.
- Each islet is a **spherical cluster** of endocrine cells, separated from the surrounding acinar tissue by a thin reticular fiber capsule.
- Islets are **richly vascularized** — each islet receives a disproportionately large blood supply (receives 10-15% of pancreatic blood flow despite comprising only 1-2% of the mass).
- **Fenestrated capillaries** within islets allow rapid sensing of blood glucose and rapid hormone release.
- **Insulo-acinar portal system**: Blood flows from the islets to the surrounding acinar tissue, bathing acinar cells in high concentrations of islet hormones (especially insulin, which potentiates acinar cell function).
### Cell Types
In H&E sections, islet cells appear as pale-staining clusters of cells. Special staining (immunohistochemistry, Gomori's aldehyde fuchsin, immunofluorescence) is needed to distinguish cell types.
| Cell type | % of islet | Location in islet | Hormone | Staining (Mallory-Azan/IHC) | Function |
|---|---|---|---|---|---|
| **Beta (β) cells** | 60-70% | Central core | **Insulin** | Aldehyde fuchsin positive (blue/purple); anti-insulin IHC | Lowers blood glucose; anabolic (promotes glycogenesis, lipogenesis, protein synthesis) |
| **Alpha (α) cells** | 15-20% | Peripheral mantle | **Glucagon** | Orange-red with Mallory-Azan; anti-glucagon IHC | Raises blood glucose; catabolic (promotes glycogenolysis, gluconeogenesis) |
| **Delta (δ) cells** | 5-10% | Scattered (between α and β) | **Somatostatin** | Anti-somatostatin IHC | Paracrine inhibition of both insulin and glucagon secretion; inhibits GI motility and secretion |
| **PP (F) cells** | ~1-2% | Periphery; more in head of pancreas | **Pancreatic polypeptide** | Anti-PP IHC | Inhibits exocrine pancreatic secretion and gallbladder contraction |
| **Epsilon (ε) cells** | <1% | Scattered | **Ghrelin** | Anti-ghrelin IHC | Stimulates appetite ("hunger hormone"); stimulates GH release |
### Ultrastructure of Beta Cell Granules
- **Distinctive crystalline core** with a wide **halo** (clear space between the crystalline core and the granule membrane).
- The crystal is formed by **zinc-insulin hexamers**.
- This wide halo is the most distinctive feature on EM.
### Ultrastructure of Alpha Cell Granules
- **Dense, round core** with a **narrow halo** (thin clear space).
- More electron-dense than beta cell granules.
> **CLINICAL: Type 1 Diabetes Mellitus**
> **Autoimmune destruction** of beta cells by T lymphocytes (Type IV hypersensitivity). Histologically: **insulitis** — lymphocytic infiltration of islets (especially early in the disease), selective loss of beta cells with preservation of other islet cell types. Eventually, islets become atrophic and may show fibrosis and amyloid deposition. Autoantibodies: **anti-GAD65 (glutamic acid decarboxylase)**, **anti-insulin (IAA)**, **anti-IA-2 (islet antigen 2)**, **anti-ZnT8**. Associated with **HLA-DR3 and HLA-DR4**. Presents with absolute insulin deficiency → hyperglycemia, polyuria, polydipsia, polyphagia, weight loss, **diabetic ketoacidosis (DKA)**.
> **CLINICAL: Type 2 Diabetes Mellitus**
> Characterized by **insulin resistance** and **relative insulin deficiency** (beta cell dysfunction). Histologically: **amyloid deposition in islets** — the amyloid is composed of **islet amyloid polypeptide (IAPP / amylin)**, which is co-secreted with insulin by beta cells. IAPP misfolds and deposits as amyloid fibrils around islet capillaries and between endocrine cells. Diagnosed by Congo red staining (apple-green birefringence under polarized light). Eventually leads to beta cell loss. Also: reduced beta cell mass (20-60% reduction), but NO insulitis.
> **CLINICAL: Insulinoma**
> Most common islet cell tumor. Usually **benign** (90%). Causes **hypoglycemia** (Whipple's triad: symptoms of hypoglycemia, low blood glucose, relief with glucose administration). Histologically: nests and trabeculae of uniform cells with round nuclei (neuroendocrine pattern); positive for **insulin, chromogranin A, synaptophysin** by IHC. Amyloid deposits (IAPP-derived) are commonly found within the tumor.
> **CLINICAL: Glucagonoma**
> Rare alpha cell tumor. Causes **necrolytic migratory erythema** (characteristic skin rash), diabetes mellitus, weight loss, anemia, DVT. The **4D syndrome**: Dermatitis, Diabetes, DVT, Depression.
> **CLINICAL: Gastrinoma (Zollinger-Ellison Syndrome)**
> Gastrin-secreting tumor. Most are in the **"gastrinoma triangle"** (duodenum, pancreas head, cystic/common bile duct junction). ~60% are malignant. Causes massive gastric acid hypersecretion → multiple peptic ulcers (especially in unusual locations like the jejunum), diarrhea. Associated with **MEN 1** (Multiple Endocrine Neoplasia type 1 — pituitary, parathyroid, pancreas; caused by mutation in the **menin** gene on chromosome 11q13).
> **CLINICAL: VIPoma (Verner-Morrison Syndrome)**
> VIP-secreting tumor. Causes watery diarrhea, hypokalemia, achlorhydria — **WDHA syndrome** or "pancreatic cholera."
> **CLINICAL: Somatostatinoma**
> Rare delta cell tumor. Causes **diabetes mellitus, gallstones (cholelithiasis), steatorrhea** — due to inhibition of insulin, CCK, and pancreatic enzyme secretion.
> **CLINICAL: MEN Syndromes and Pancreatic Islet Tumors**
> **MEN 1** (Wermer syndrome): Parathyroid hyperplasia + Pituitary adenoma + Pancreatic islet cell tumors (gastrinoma most common, then insulinoma, glucagonoma, VIPoma). Mutation: **menin gene** (tumor suppressor, 11q13).
> **MEN 2A** (Sipple syndrome): Medullary thyroid carcinoma + Pheochromocytoma + Parathyroid hyperplasia. Mutation: **RET proto-oncogene** (10q11.2).
---
# 3. LIVER
The liver is the **largest internal organ** (~1.5 kg) and the **largest gland** in the body. It is both an exocrine gland (secretes bile) and an endocrine gland (secretes proteins and hormones directly into the blood).
---
## CAPSULE
- **Glisson's capsule**: A thin layer of **dense irregular connective tissue** covering the entire liver surface.
- Covered externally by **visceral peritoneum (mesothelium/serosa)** except at the **bare area** (where the liver is in direct contact with the diaphragm).
- At the **porta hepatis** (hilum), Glisson's capsule extends into the liver parenchyma, forming a **connective tissue tree** that accompanies the portal triad (portal vein, hepatic artery, bile duct) throughout the liver. This connective tissue framework is minimal in humans (compared to pigs, where it is very prominent and clearly delineates lobules).
---
## STRUCTURAL AND FUNCTIONAL UNITS OF THE LIVER
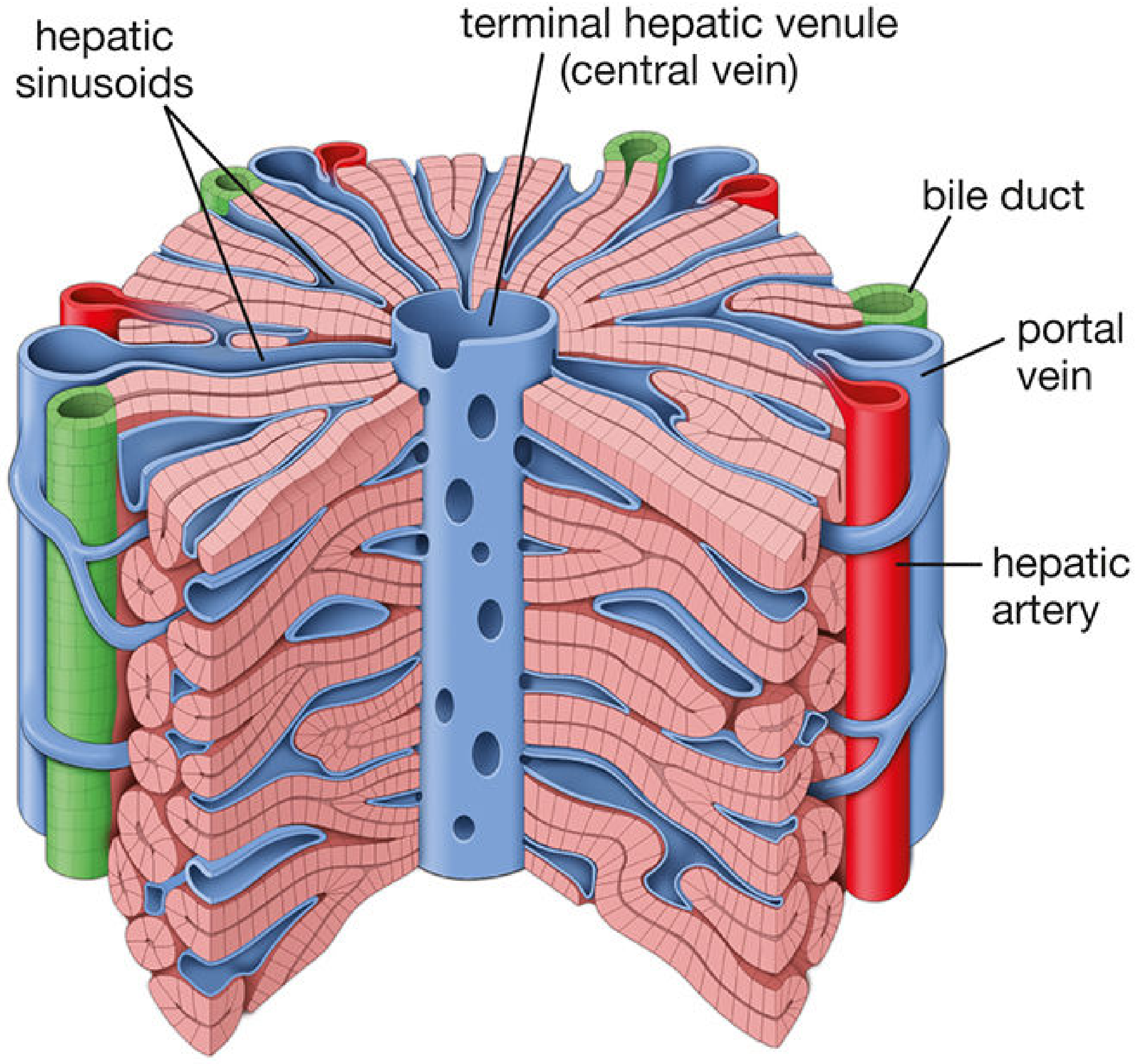
### A. Classic Hepatic Lobule
The **traditional** model for understanding liver architecture.
- **Shape**: **Hexagonal** in cross-section (best seen in pig liver where interlobular connective tissue is abundant; in humans, lobule boundaries are indistinct).
- **Central vein**: Each lobule is centered on a **central vein (terminal hepatic venule/centrilobular vein)**.
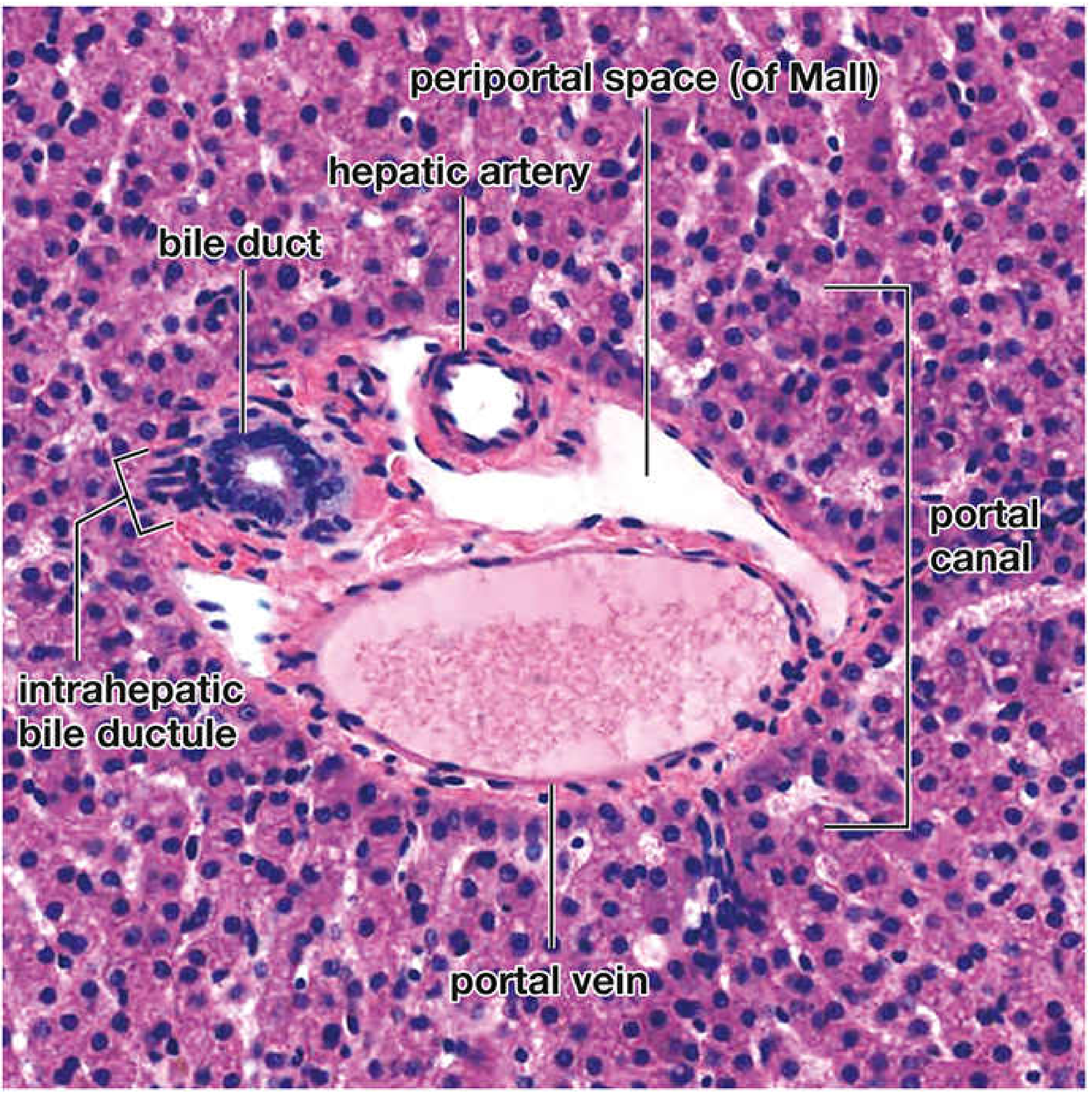
- **Portal triads (portal canals)**: Located at the **corners (angles)** of the hexagon. Each portal triad contains:
1. **Branch of the hepatic artery** (hepatic arteriole) — carries oxygenated blood.
2. **Branch of the portal vein** (portal venule) — carries nutrient-rich, deoxygenated blood from the GI tract, spleen, and pancreas.
3. **Bile duct (bile ductule)** — carries bile away from the lobule (toward the porta hepatis; bile flows in the **opposite direction** to blood flow).
4. **Lymphatic vessel** (not always visible).
5. All surrounded by connective tissue (part of Glisson's capsule extension).
- **Hepatocyte plates (Muralium)**: Hepatocytes are arranged in **anastomosing plates** (one to two cells thick) that radiate from the central vein like **spokes of a wheel**.
- **Sinusoids**: Between the hepatocyte plates are hepatic sinusoids — wide, irregular vascular channels through which blood flows from the periphery (portal triads) **centripetally toward the central vein**.
- **Bile flow**: Bile flows **centrifugally** — from the center of the lobule (bile canaliculi between hepatocytes) toward the periphery (portal triads where bile ductules are located). This is **OPPOSITE** to blood flow.
### B. Portal Lobule
- Emphasizes the **exocrine function** of the liver (bile secretion).
- **Shape**: **Triangular**, with a portal triad at the center and three central veins at the corners.
- All hepatocytes within one portal lobule drain bile into the **same bile duct** (at the central portal triad).
### C. Liver Acinus (of Rappaport)
The **most physiologically relevant** and clinically useful model.
- **Shape**: **Diamond (rhomboid)**-shaped, centered on the short axis between two adjacent portal triads. Two central veins lie at the ends of the long axis.
- Divided into **three zones** based on proximity to the portal triad (blood supply):
| Zone | Location | O₂/nutrient supply | Characteristics |
|---|---|---|---|
| **Zone 1 (periportal)** | Closest to the portal triad | Highest O₂ and nutrients | Most active in: oxidative metabolism, gluconeogenesis, urea synthesis, bile salt secretion, cholesterol synthesis. **First to regenerate** after injury. **Last to show necrosis** (most resistant to ischemia). **First to accumulate fat** in starvation (not alcohol). First affected by toxins entering via portal blood (e.g., **phosphorus poisoning**). |
| **Zone 2 (intermediate/midzone)** | Between zones 1 and 3 | Intermediate | Intermediate metabolic activity. **Yellow fever** characteristically causes **midzonal necrosis**. |
| **Zone 3 (pericentral/centrilobular)** | Closest to the central vein | Lowest O₂ and nutrients | Most active in: drug detoxification (highest concentration of **CYP450 enzymes**, especially CYP2E1), lipogenesis, glycolysis, glycogenolysis, glutamine synthesis. **Most susceptible to ischemic necrosis** (e.g., in heart failure, shock). **First to show fatty change (steatosis) in alcohol abuse**. **First to show necrosis with toxic injury** (e.g., CCl₄, acetaminophen — because CYP450 metabolizes these to toxic metabolites, and zone 3 has the most CYP450). **Last to regenerate**. |
> **CLINICAL: Centrilobular (Zone 3) Necrosis**
> Causes: **ischemia** (shock, congestive heart failure — "nutmeg liver" appearance due to congested central veins surrounded by pale periportal parenchyma), **acetaminophen toxicity** (toxic metabolite NAPQI generated by CYP2E1 in zone 3 depletes glutathione → oxidative damage; treated with **N-acetylcysteine** which replenishes glutathione), **CCl₄ toxicity**, **halothane hepatitis**.
> **CLINICAL: Periportal (Zone 1) Necrosis**
> Causes: **eclampsia of pregnancy** (periportal fibrin deposition and hemorrhage), **phosphorus poisoning**.
> **CLINICAL: Midzonal (Zone 2) Necrosis**
> Cause: **Yellow fever** (Councilman bodies = apoptotic hepatocytes).
> **CLINICAL: Bridging Necrosis**
> Necrosis that connects central veins to portal triads (central-central or central-portal bridging). Seen in severe viral hepatitis, drug reactions. Indicates severe injury with risk of progression to cirrhosis.
---
## HEPATOCYTES
Hepatocytes make up **~80% of the liver's volume** and are the principal functional cells.
### General Features
- **Shape**: Large, polyhedral cells (~20-30 μm in diameter).
- **Nucleus**:
- Round, centrally placed, with one or two prominent **nucleoli**.
- Many hepatocytes are **binucleated** (~25% in adults).
- Many are **polyploid** (4n, 8n, or even 16n — tetraploid or octaploid) — this increases with age and reflects the high metabolic activity without cell division.
- **Lifespan**: ~150-200 days (long-lived but with significant regenerative capacity).
### Surfaces/Domains of Hepatocytes
Each hepatocyte has **THREE distinct surface domains**:
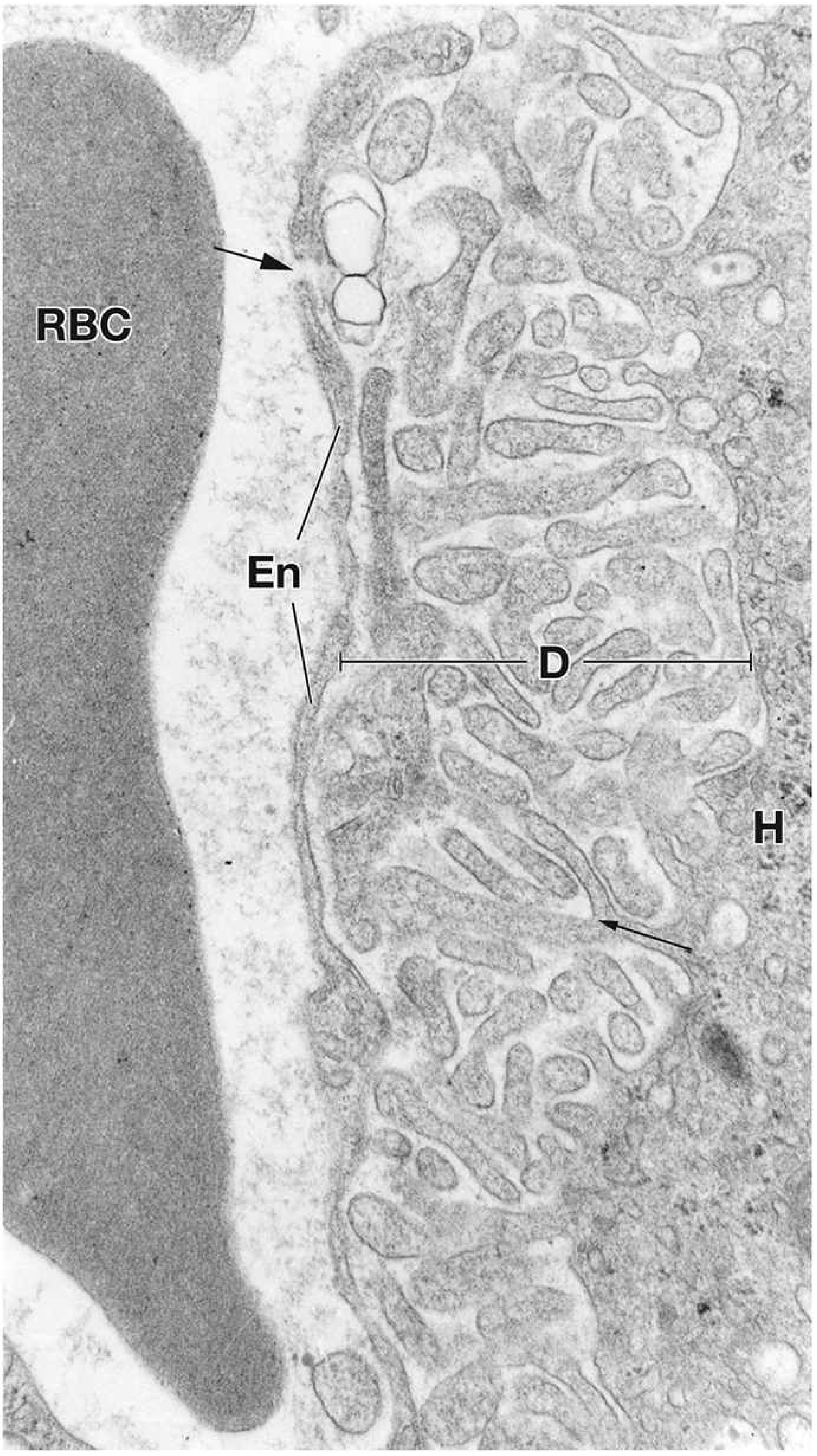
**1. Sinusoidal (Basal) Surface**
- Faces the hepatic sinusoid.
- Separated from the sinusoidal endothelium by the **Space of Disse (perisinusoidal space)**.
- Has abundant **microvilli** that project into the space of Disse, greatly increasing the surface area for exchange of substances between the blood and hepatocytes.
- Site of absorption of nutrients, hormones, drugs from sinusoidal blood.
- Site of secretion of proteins (albumin, coagulation factors, lipoproteins), glucose, and other substances into the blood.
**2. Lateral (Intercellular) Surface**
- Faces adjacent hepatocytes.
- Contains **gap junctions** (intercellular communication), **desmosomes** (adhesion), and the **bile canaliculus**.
**3. Bile Canalicular (Apical) Surface**
- A **groove** formed between two adjacent hepatocytes.
- The bile canaliculus is NOT a separate structure with its own wall — it is simply a **specialized portion of the intercellular space** sealed by **tight junctions (zonulae occludentes)** on either side.
- **Microvilli** project into the canaliculus.
- **ABC transporters** on the canalicular membrane actively secrete bile components (bile salts, bilirubin diglucuronide, phospholipids, cholesterol) into the canaliculus.
- Bile flows through the canalicular network toward the portal triads.
### Hepatocyte Ultrastructure (Extensive Organelle Complement)
Hepatocytes are among the most organelle-rich cells in the body, reflecting their enormous metabolic versatility.
- **rER (Rough Endoplasmic Reticulum)**: Extensive, organized into stacks (ergastoplasm). Responsible for synthesis of:
- **Albumin** (the most abundant plasma protein)
- **Coagulation factors** (I/fibrinogen, II/prothrombin, V, VII, IX, X, XI, XII, XIII)
- **Complement proteins** (C3, etc.)
- **Transferrin, ceruloplasmin, α₁-antitrypsin, haptoglobin, lipoproteins (VLDL, HDL), angiotensinogen, IGF-1, thrombopoietin**
- **sER (Smooth Endoplasmic Reticulum)**: Very abundant. Functions:
- **Drug detoxification**: Contains **cytochrome P450 (CYP450)** mixed-function oxidase system — Phase I reactions (oxidation, reduction, hydrolysis). Most important enzymes: CYP3A4, CYP2D6, CYP2E1.
- **Steroid hormone metabolism**: Conjugation and inactivation of steroid hormones.
- **Bile acid synthesis** from cholesterol.
- **Cholesterol synthesis** (contains **HMG-CoA reductase**).
- **Glucuronidation**: Bilirubin conjugation (UDP-glucuronosyltransferase).
- **Lipid and lipoprotein metabolism**.
- **Glycogenolysis**: Contains **glucose-6-phosphatase**, which converts G6P → glucose (unique to liver and kidney — this enzyme is absent in muscle, which is why muscle glycogen cannot directly contribute to blood glucose).
- sER **proliferates (hypertrophies)** in response to drugs (e.g., barbiturates, alcohol, phenytoin) — this is the basis of **drug tolerance/enzyme induction**.
- **Golgi apparatus**: Multiple (up to 50 Golgi stacks per hepatocyte). Involved in packaging and sorting of proteins and lipoproteins (VLDL assembly).
- **Mitochondria**: Very numerous (~800-1000 per cell). Both round and elongated forms. Contain their own DNA. Support the enormous energy demands.
- **β-oxidation of fatty acids**
- **Citric acid (Krebs) cycle**
- **Urea cycle** (partially — some enzymes in mitochondria, some in cytoplasm)
- **Ketogenesis**
- **Heme synthesis** (first step: ALA synthase in mitochondria)
- **Lysosomes**: Contain acid hydrolases. Involved in:
- Turnover of organelles (autophagy)
- Degradation of glycogen (acid α-glucosidase)
- Storage of **lipofuscin** ("wear-and-tear pigment") — increases with age, representing undigested residual bodies from lysosomal activity
- Storage of **iron** as **ferritin** and **hemosiderin**
- Storage of **copper** (normally excreted into bile)
- **Peroxisomes (Microbodies)**: Abundant. Functions:
- **β-oxidation of very-long-chain fatty acids (VLCFA)**
- **α-oxidation of branched-chain fatty acids (e.g., phytanic acid)**
- Breakdown of **H₂O₂** by **catalase**
- Bile acid synthesis
- Cholesterol synthesis
- Plasmalogen synthesis
- **Glycogen**: Stored as glycogen particles (rosettes of α particles or individual β particles). Visible in EM and can be demonstrated by **PAS staining** (magenta/pink). Amount varies with nutritional state (more after meals, less during fasting).
- **Lipid droplets**: Small lipid inclusions normally present; increase dramatically in **steatosis (fatty liver disease)**.
- **Inclusions**: Lipofuscin, ferritin, hemosiderin, glycogen, lipid.
> **CLINICAL: sER Induction and Drug Metabolism**
> Chronic exposure to barbiturates, alcohol, phenytoin, rifampin, and other drugs induces proliferation of sER in hepatocytes (sER hypertrophy). This is visible on EM and causes **hepatocyte swelling (ground-glass hepatocytes)**. It increases the rate of drug metabolism, leading to **drug tolerance** (the same dose produces less effect) and potentially **drug interactions** (one drug induces enzymes that metabolize another drug faster).
> **CLINICAL: Hepatitis B — Ground-Glass Hepatocytes**
> In chronic hepatitis B infection, hepatocytes accumulate large amounts of **HBsAg (hepatitis B surface antigen)** in their sER, causing the cytoplasm to have a characteristic **"ground-glass" appearance** on H&E staining. Confirmed by **Orcein stain** or **immunohistochemistry for HBsAg**.
> **CLINICAL: α₁-Antitrypsin Deficiency**
> **PiZZ genotype** — the mutant Z variant of α₁-antitrypsin misfolds and accumulates in the rER of hepatocytes (cannot be secreted). Histologically: **PAS-positive, diastase-resistant globules** in the cytoplasm of periportal hepatocytes. Leads to **liver disease** (neonatal hepatitis, cirrhosis, hepatocellular carcinoma) and **emphysema** (uninhibited neutrophil elastase destroys alveolar walls). Liver disease is caused by the **accumulation of misfolded protein** (gain-of-function toxic effect), NOT by deficiency of the protein.
> **CLINICAL: Wilson Disease (Hepatolenticular Degeneration)**
> Autosomal recessive mutation in **ATP7B** gene (copper-transporting ATPase on hepatocyte canalicular membrane). Copper cannot be excreted into bile or incorporated into ceruloplasmin → copper accumulates in hepatocytes (stored in lysosomes), then in brain (basal ganglia — particularly putamen), cornea (**Kayser-Fleischer rings** — copper deposits in Descemet's membrane). Histologically in liver: steatosis, hepatitis, eventually cirrhosis. **Rhodanine stain** or **rubeanic acid stain** demonstrates copper. EM shows characteristic **mitochondrial abnormalities** (increased matrix density, widened cristae, crystalline inclusions).
> **CLINICAL: Hemochromatosis**
> **Primary/Hereditary**: Autosomal recessive mutation in **HFE gene** (C282Y most common). Leads to excessive iron absorption. Iron deposits in hepatocytes (as hemosiderin) → hepatocyte damage → cirrhosis, hepatocellular carcinoma. Also affects heart (cardiomyopathy), pancreas (diabetes — "bronze diabetes"), skin (hyperpigmentation), joints (arthritis). **Prussian blue stain (Perls stain)** demonstrates iron as blue granules.
> **CLINICAL: Steatosis (Fatty Liver)**
> **Macrovesicular steatosis**: Large single fat droplet displacing the nucleus to the periphery (signet-ring appearance). Causes: alcohol, obesity/metabolic syndrome (NAFLD/NASH), diabetes, corticosteroids, starvation (kwashiorkor).
> **Microvesicular steatosis**: Numerous small fat droplets, nucleus remains central. Causes: **Reye syndrome** (children given aspirin during viral infection), **acute fatty liver of pregnancy**, tetracycline toxicity, valproic acid. More serious — indicates mitochondrial dysfunction/β-oxidation defects.
---
## HEPATIC SINUSOIDS
The sinusoids are the unique vascular channels of the liver.
### Structure
- **Wide, irregular channels** (9-12 μm diameter) — much wider than regular capillaries.
- Lined by a **discontinuous endothelium**:
- Endothelial cells have **large fenestrations (fenestrae)** grouped into clusters called **sieve plates**.
- Fenestrae are ~100-150 nm in diameter.
- **No diaphragms** over the fenestrae (unlike fenestrated capillaries of the kidney or intestine).
- **No continuous basal lamina** — there may be a discontinuous or absent basal lamina.
- This unique structure makes sinusoids the most permeable blood vessels in the body, allowing free passage of plasma (but not cells) into the space of Disse.
### Space of Disse (Perisinusoidal Space)
- The narrow space between the sinusoidal endothelium and the hepatocyte surface.
- Contains:
- **Plasma** that has filtered through the endothelial fenestrae.
- **Reticular fibers (type III collagen)** that provide structural support.
- **Hepatocyte microvilli** projecting into the space.
- **Hepatic stellate cells (Ito cells)** — see below.
- Blood plasma in the space of Disse has direct access to the hepatocyte surface, facilitating efficient exchange of substances.
- The space of Disse is the primary site of **lymph formation** in the liver — fluid from this space enters lymphatic vessels in the portal triads. The liver produces approximately **25-50% of all thoracic duct lymph**.
### Cells Associated with Sinusoids
**1. Kupffer Cells**
- **Identity**: Resident macrophages of the liver; part of the **mononuclear phagocyte system (MPS/reticuloendothelial system)**.
- **Location**: Within the sinusoidal lumen, attached to or partly embedded in the endothelial lining. Most abundant in the periportal region (zone 1).
- **Morphology**: Large, irregular cells with a kidney-shaped or indented nucleus. Cytoplasm contains **lysosomes**, **phagosomes**, and residual bodies (including **hemosiderin** from red blood cell breakdown).
- **Functions**:
- **Phagocytosis**: Remove bacteria, cell debris, aged erythrocytes, immune complexes, endotoxins from the portal blood. Particularly important because portal blood from the GI tract contains bacteria and bacterial products (endotoxins/LPS) that have crossed the intestinal barrier.
- **Antigen presentation**.
- **Cytokine production**: TNF-α, IL-1, IL-6, IL-12.
- **Iron recycling**: Phagocytose old RBCs, break down hemoglobin, store iron as ferritin/hemosiderin, release iron to transferrin.
- **Markers**: CD68, CD163, lysozyme.
> **CLINICAL: Kupffer cells in disease**
> In alcoholic liver disease, Kupffer cells are activated by endotoxin (LPS) that enters the portal blood due to increased gut permeability. Activated Kupffer cells release **TNF-α and other pro-inflammatory cytokines**, contributing to hepatocyte injury and inflammation. In chronic liver disease, Kupffer cells play a role in hepatic fibrosis by activating **hepatic stellate cells**. In **Gaucher disease** (glucocerebrosidase deficiency), Kupffer cells (and other macrophages) accumulate **glucocerebroside**, becoming enlarged "Gaucher cells" with characteristic **"wrinkled tissue paper" cytoplasm**.
**2. Hepatic Stellate Cells (Ito Cells / Perisinusoidal Cells / Fat-Storing Cells / Lipocytes)**
- **Location**: In the **Space of Disse**, between endothelial cells and hepatocytes.
- **Normal function**: Store **vitamin A (retinol/retinoids)** as retinyl esters in characteristic **lipid droplets** in their cytoplasm. They store ~80% of the body's vitamin A.
- **Identification**: EM shows characteristic lipid droplets; IHC positive for **desmin**, **GFAP (glial fibrillary acidic protein)** in quiescent state.
- **In liver injury/fibrosis**: Stellate cells undergo **activation** — they transform from quiescent, vitamin A-storing cells into **myofibroblast-like cells** that:
- Lose their vitamin A stores.
- Express **α-smooth muscle actin (α-SMA)**.
- Proliferate.
- Produce excessive **extracellular matrix** (especially **Type I and Type III collagen**) in the space of Disse.
- This process is called **"capillarization of sinusoids"**: the deposition of collagen in the space of Disse creates a continuous basal lamina, and the sinusoidal endothelium loses its fenestrae. This impairs the exchange of substances between blood and hepatocytes.
- Activated stellate cells also contract (due to α-SMA), increasing portal pressure.
- **Activation signals**: TGF-β (most potent fibrogenic cytokine), PDGF (most potent mitogen/proliferative signal), TNF-α (from Kupffer cells), reactive oxygen species, endothelin-1, acetaldehyde (alcohol metabolite).
> **CLINICAL: Hepatic Fibrosis and Cirrhosis**
> Hepatic stellate cell activation is the **central event** in hepatic fibrosis of any etiology (viral hepatitis, alcohol, NAFLD, autoimmune hepatitis, etc.). Continued fibrosis leads to **cirrhosis**: irreversible transformation of normal liver architecture into **regenerative nodules** surrounded by **fibrous septa (bridging fibrosis)**. The fibrosis disrupts the normal lobular architecture, compresses sinusoids and central veins, and leads to **portal hypertension** (increased resistance to portal blood flow). Consequences of portal hypertension: **esophageal/gastric varices** (risk of fatal hemorrhage), **caput medusae** (periumbilical varices), **splenomegaly** (congestion), **hemorrhoids** (anorectal varices), **ascites** (from increased hydrostatic pressure + decreased albumin synthesis). Hepatocyte dysfunction in cirrhosis causes: decreased albumin → edema/ascites; decreased clotting factors → bleeding tendency; decreased bilirubin conjugation → jaundice; decreased estrogen metabolism → gynecomastia, spider angiomata, palmar erythema, testicular atrophy; decreased ammonia metabolism → hepatic encephalopathy.
> **CLINICAL: Special stains for fibrosis**
> **Masson's trichrome** stains collagen **blue/green**. **Reticulin stain (silver impregnation)** shows the reticular fiber framework (type III collagen — fibers appear black). In cirrhosis, there is both increased collagen AND distortion of the reticulin framework. **Sirius red stain** under polarized light specifically highlights collagen fibers.
**3. Pit Cells**
- **Identity**: **Liver-associated natural killer (NK) cells** / large granular lymphocytes.
- **Location**: Within sinusoidal lumen, attached to endothelial cells or Kupffer cells.
- **Function**: Cytotoxic activity against tumor cells and virus-infected cells. Important in innate immune surveillance of the liver.
- **Granules**: Contain perforin and granzymes.
---
## BILE CANALICULI AND BILE DRAINAGE PATHWAY
### Bile Canaliculi
- Smallest bile channels — formed by grooves in adjacent hepatocyte surfaces.
- Sealed by **tight junctions (zona occludens)** — prevent bile leakage into the sinusoidal space.
- Contain **microvilli** to increase surface area.
- **Bile flow direction**: From the center of the lobule → toward the periphery (centrifugal — opposite to blood flow).
- Canaliculi are NOT lined by duct cells — they are simply modified intercellular spaces between hepatocytes.
### Canals of Hering (Cholangioles)
- The **transition zone** between bile canaliculi and bile ductules.
- Lined partly by hepatocytes and partly by **cholangiocytes** (bile duct epithelial cells).
- Believed to harbor **hepatic progenitor/stem cells (oval cells)** that can differentiate into both hepatocytes and cholangiocytes.
> **CLINICAL: Oval cells and liver regeneration**
> When hepatocyte proliferation is impaired (e.g., in severe or chronic injury), **oval cells** (hepatic progenitor cells) in the canals of Hering are activated. They proliferate and differentiate into hepatocytes and cholangiocytes. This is called the **"ductular reaction."** These progenitor cells may play a role in hepatocarcinogenesis.
### Bile Ductules (Cholangioles/Ductules of Hering)
- Small ducts at the periphery of the lobule.
- Lined by cuboidal cholangiocytes.
### Interlobular Bile Ducts
- Located in the portal triads.
- Lined by **simple cuboidal to columnar epithelium** (cholangiocytes).
- Cholangiocytes **modify bile** by:
- **Secreting water and HCO₃⁻** (stimulated by **secretin**) — similar to pancreatic duct cells.
- **Absorbing glucose** and amino acids from bile.
- **Reabsorbing bile salts** via ASBT (apical sodium-dependent bile acid transporter) — part of cholehepatic shunt.
### Larger Bile Ducts
- Right and left hepatic ducts → **common hepatic duct** → joined by cystic duct → **common bile duct (ductus choledochus)** → opens at the major duodenal papilla (with or without the pancreatic duct).
- Wall becomes progressively thicker with a layer of smooth muscle appearing in larger ducts.
- Epithelium: Simple columnar with increasing goblet cells.
- Periductal glands (mucous glands) are present around larger bile ducts.
> **CLINICAL: Primary Biliary Cholangitis (PBC, formerly Primary Biliary Cirrhosis)**
> Autoimmune destruction of **small intrahepatic bile ducts** (interlobular bile ducts). Characterized by **anti-mitochondrial antibodies (AMA)** — specifically against the **E2 subunit of pyruvate dehydrogenase (PDC-E2)**. Histologically: **"florid duct lesion"** — granulomatous destruction of bile ducts with lymphocytic and granulomatous inflammation surrounding damaged bile ducts. Leads to chronic cholestasis, pruritus, jaundice, xanthomas, eventually cirrhosis. Most common in **middle-aged women**.
> **CLINICAL: Primary Sclerosing Cholangitis (PSC)**
> Chronic inflammation and fibrosis of intrahepatic AND extrahepatic bile ducts. "Onion-skin" periductal fibrosis. Strong association with **ulcerative colitis** (70% of PSC patients have UC). **p-ANCA** positive in ~80%. Leads to cholestasis, cirrhosis, and increased risk of **cholangiocarcinoma**. ERCP shows characteristic "beaded" appearance of bile ducts (alternating strictures and dilations). Most common in **young men**.
> **CLINICAL: Cholangiocarcinoma**
> Malignant tumor of bile duct epithelium (cholangiocytes). Risk factors: PSC, liver fluke infection (**Clonorchis sinensis, Opisthorchis viverrini**), Caroli disease, choledochal cysts, hepatolithiasis. **Klatskin tumor**: cholangiocarcinoma at the bifurcation of the right and left hepatic ducts (most common location for extrahepatic cholangiocarcinoma).
---
## BILE COMPOSITION AND ENTEROHEPATIC CIRCULATION
### Bile Composition
- **Bile salts/acids** (~67%): Cholic acid and chenodeoxycholic acid (primary bile acids, synthesized from cholesterol by hepatocytes). Conjugated with taurine or glycine. Bacteria in the colon convert them to secondary bile acids (deoxycholic acid and lithocholic acid).
- **Phospholipids** (~22%): Mainly lecithin (phosphatidylcholine).
- **Cholesterol** (~4%).
- **Bilirubin** (conjugated as bilirubin diglucuronide).
- **Water, electrolytes, bicarbonate, IgA**.
### Enterohepatic Circulation of Bile Salts
- Bile salts secreted into the duodenum.
- Emulsify fats in the small intestine (forming micelles for fat absorption).
- ~95% of bile salts reabsorbed in the **terminal ileum** (by **ASBT** — apical sodium-dependent bile acid transporter on the apical membrane of ileal enterocytes).
- Return to the liver via the **portal vein**.
- Taken up by hepatocytes (via **NTCP** — Na⁺-taurocholate cotransporting polypeptide on the sinusoidal membrane).
- Re-secreted into bile.
- The pool of bile salts (~2-4 g) recycles **6-8 times per day** (~20-30 g total bile salts secreted/day).
- ~5% lost in feces → replaced by new synthesis from cholesterol.
> **CLINICAL: Gallstones (Cholelithiasis)**
> **Cholesterol stones** (80% in Western countries): Result from supersaturation of bile with cholesterol (increased cholesterol, decreased bile salts, decreased lecithin). Risk factors: **5 F's** — Fat, Female, Fertile (multiparous), Forty, Fair (Caucasian). Also: OCP use, rapid weight loss, fibrate drugs, Crohn disease (decreased bile salt reabsorption from diseased terminal ileum → decreased bile salt pool → cholesterol supersaturation).
> **Pigment stones** (20%): **Black** stones — associated with chronic hemolysis (sickle cell disease, thalassemia, hereditary spherocytosis), cirrhosis. Contain calcium bilirubinate. **Brown** stones — associated with biliary infection/stasis; contain calcium bilirubinate + fatty acid salts + cholesterol; more common in Asian populations.
---
## BLOOD SUPPLY OF THE LIVER — DUAL BLOOD SUPPLY
- **Hepatic artery** (~25% of hepatic blood flow, ~50% of O₂ supply): Carries oxygenated blood from the celiac trunk.
- **Portal vein** (~75% of hepatic blood flow, ~50% of O₂ supply): Carries nutrient-rich, partially deoxygenated blood from the GI tract, spleen, and pancreas.
### Blood Flow Pathway
Portal vein + hepatic artery (at porta hepatis) → branches in portal triads → **inlet venules and arterioles** → sinusoids (blood mixes) → **central vein (terminal hepatic venule)** → **sublobular veins (collecting veins)** → **hepatic veins** (3 major: right, middle, left) → **inferior vena cava**.
> **CLINICAL: Budd-Chiari Syndrome**
> Thrombosis of the **hepatic veins** (or IVC at the hepatic vein level). Causes: hypercoagulable states (**polycythemia vera** — most common overall, paroxysmal nocturnal hemoglobinuria, hepatocellular carcinoma, pregnancy, oral contraceptives, myeloproliferative disorders). Clinical triad: **hepatomegaly, ascites, abdominal pain**. Histologically: **centrilobular congestion and necrosis** (zone 3 — because the hepatic vein outflow is blocked). "Nutmeg liver" appearance.
> **CLINICAL: Portal Hypertension**
> Classification by site of obstruction:
> - **Prehepatic**: Portal vein thrombosis, splenomegaly.
> - **Intrahepatic** (most common): Cirrhosis (any cause), schistosomiasis (portal/periportal fibrosis from *S. mansoni* or *S. japonicum*), sinusoidal obstruction syndrome (veno-occlusive disease — toxicity to sinusoidal endothelium, e.g., from bush tea pyrrolizidine alkaloids or post-bone marrow transplant).
> - **Posthepatic**: Budd-Chiari syndrome, constrictive pericarditis, severe right heart failure.
---
## HEPATOCYTE REGENERATION
- Hepatocytes are normally **quiescent (G₀ phase)** but have remarkable regenerative capacity.
- After partial hepatectomy (up to 70% resection), the remaining hepatocytes enter the cell cycle and proliferate to restore the original liver mass within **1-2 weeks**.
- Key signals: **HGF (hepatocyte growth factor)**, **EGF**, **TGF-α**, **IL-6**, **TNF-α** (the latter two are produced by Kupffer cells and prime hepatocytes for mitogenic signals).
- When hepatocyte proliferation is impaired, **oval cells (hepatic progenitor cells)** in the canals of Hering are activated.
> **CLINICAL: Liver tumors**
> **Hepatocellular carcinoma (HCC)**: Most common primary malignant liver tumor. Major risk factors: cirrhosis of any cause (especially hepatitis B, hepatitis C, alcohol, hemochromatosis, aflatoxin B1 exposure — from *Aspergillus flavus*). Aflatoxin B1 causes a specific **TP53 mutation** (codon 249 Arg→Ser). Elevated serum **α-fetoprotein (AFP)**. Histologically: trabecular, pseudoacinar, or solid patterns of atypical hepatocytes; may produce bile; positive for **Hep Par 1** and **arginase-1** by IHC.
> **Hepatic adenoma**: Benign tumor of hepatocytes. Associated with **oral contraceptive (OCP) use** and **anabolic steroids**. Risk of rupture and hemorrhage. Subtype with **β-catenin mutation** has risk of malignant transformation to HCC.
> **Focal nodular hyperplasia (FNH)**: Not a true neoplasm. Characterized by a **central stellate scar** with radiating fibrous septa and abnormal ("dystrophic") blood vessels. No increased risk of malignancy. No association with OCP use (though previously thought).
> **Cavernous hemangioma**: Most common benign liver tumor overall. Vascular malformation. Risk of hemorrhage if biopsied (never biopsy a suspected hemangioma!).
---
# 4. GALLBLADDER
## GENERAL FEATURES
- A **pear-shaped, hollow organ** on the visceral (inferior) surface of the liver.
- **Functions**: Storage, concentration, and release of bile.
- **Capacity**: ~30-50 mL.
---
## HISTOLOGICAL LAYERS
The gallbladder wall has **three layers** (NOT the usual four of the GI tract — there is NO muscularis mucosae and NO submucosa).
### 1. Mucosa
**Epithelium**:
- **Simple tall columnar epithelium** with microvilli (brush border) on the apical surface.
- Cells resemble absorptive cells.
- The primary function is **absorption of water, Na⁺, and Cl⁻** from the stored bile, thereby **concentrating bile up to 10-fold**.
- Mechanism: Na⁺/K⁺-ATPase on the basolateral membrane pumps Na⁺ out → creates an osmotic gradient → water follows.
- Cells also transport **Na⁺ and Cl⁻** into the lateral intercellular space → water follows → fluid transported to lamina propria → absorbed by blood vessels.
- **No goblet cells** in the epithelium of the body and fundus (unlike the stomach or intestine).
- Near the neck of the gallbladder: **mucous glands (tubuloalveolar glands)** are present in the lamina propria. These glands secrete mucus that protects the neck and cystic duct epithelium.
**Lamina propria**:
- Loose connective tissue with blood vessels, lymphatics, and occasional lymphocytes.
- Contains **Rokitansky-Aschoff sinuses**: Deep invaginations/outpouchings of the mucosal epithelium that penetrate into and sometimes through the muscular layer. These are **NOT diverticula** in the pathological sense but are characteristic of the gallbladder, especially prominent in chronic cholecystitis.
**Surface topography**:
- The mucosa is thrown into numerous **irregular folds (rugae)** when the gallbladder is empty, giving a honeycomb appearance in cross-section. These folds flatten when the gallbladder distends with bile.
- These folds should NOT be confused with villi — they are temporary mucosal folds, not permanent projections.
### 2. Muscularis (Muscularis Externa)
- **Randomly oriented** smooth muscle fibers interspersed with connective tissue — NOT organized into distinct circular and longitudinal layers as in the GI tract.
- Some fibers are oblique, some circular, some longitudinal.
- **Function**: Contraction expels bile into the cystic duct and then into the common bile duct.
- Contraction is stimulated by **CCK (cholecystokinin)** — released from I cells of the duodenal mucosa in response to fats and amino acids/peptides.
- **Vagal (parasympathetic)** stimulation also promotes contraction.
- **Sympathetic** stimulation and **somatostatin** inhibit contraction.
### 3. Adventitia/Serosa
- The surface facing the liver: **adventitia** — connective tissue that blends with the liver's connective tissue (Glisson's capsule). No peritoneal covering on this surface.
- The free surface (facing the peritoneal cavity): **serosa** — connective tissue covered by **mesothelium (simple squamous epithelium)**.
- Contains blood vessels, lymphatics, nerves, and adipose tissue.
**Note**: There is **NO MUSCULARIS MUCOSAE** and **NO SUBMUCOSA** in the gallbladder.
---
## SPECIAL FEATURES
### Luschka Ducts (Ducts of Luschka)
- Small bile ductules found in the connective tissue between the gallbladder wall and the liver surface (in the gallbladder bed).
- They may drain directly from the liver parenchyma into the gallbladder or connect with intrahepatic bile ducts.
- **Clinical significance**: If not recognized and ligated during cholecystectomy, they can cause **bile leaks** postoperatively.
### Spiral Valve of Heister
- **Mucosal folds** arranged in a spiral pattern within the **cystic duct**.
- NOT a true valve but helps regulate bile flow into and out of the gallbladder.
- Contains smooth muscle.
- Can be a site of **gallstone impaction**.
---
## CLINICAL CORRELATIONS — GALLBLADDER
> **CLINICAL: Cholelithiasis (Gallstones)**
> Already discussed under liver section. Stones in the gallbladder can obstruct the cystic duct (→ acute cholecystitis) or common bile duct (→ obstructive jaundice, cholangitis).
> **CLINICAL: Acute Cholecystitis**
> Usually caused by **gallstone impaction in the cystic duct** (90% calculous cholecystitis). Occasionally without stones (acalculous cholecystitis — seen in critically ill patients, diabetics, those on TPN). Histologically: **edema, hemorrhage, acute inflammation (neutrophilic infiltrate), fibrin**, and in severe cases, **gangrenous necrosis** of the wall with risk of perforation.
> **CLINICAL: Chronic Cholecystitis**
> Chronic inflammation due to repeated bouts of acute cholecystitis or chronic irritation by gallstones. Histologically: **mucosal atrophy, fibrosis and thickening of the wall, chronic inflammatory infiltrate (lymphocytes, macrophages, plasma cells), prominent Rokitansky-Aschoff sinuses** (deep mucosal invaginations into or through the muscular layer — pathognomonic), and occasionally **dystrophic calcification** of the wall.
> **CLINICAL: Porcelain Gallbladder**
> **Dystrophic calcification** of the gallbladder wall, visible on imaging (X-ray/CT). Associated with chronic cholecystitis. Previously thought to carry a high risk of **gallbladder carcinoma**, but this association is now debated (the risk may be lower than previously believed, but prophylactic cholecystectomy is still often recommended).
> **CLINICAL: Cholesterolosis (Strawberry Gallbladder)**
> Accumulation of **cholesterol esters** in macrophages in the lamina propria of the gallbladder mucosa. Grossly: yellow lipid-laden specks on a reddened mucosa (resembling a strawberry). The macrophages become **"foamy cells"**. Usually an incidental finding, generally benign.
> **CLINICAL: Gallbladder Carcinoma**
> Most common malignancy of the biliary tract. Risk factors: gallstones (present in 75-90% of cases), porcelain gallbladder, gallbladder polyps >1 cm, anomalous pancreaticobiliary junction, chronic *Salmonella* infection. Most are **adenocarcinomas**. Often diagnosed late (advanced stage at presentation) because the gallbladder lacks a submucosa — tumors can rapidly invade the muscular layer and the liver. Prognosis is poor.
> **CLINICAL: Courvoisier's Law/Sign**
> A palpable, non-tender gallbladder in the presence of jaundice is likely due to **malignant obstruction** of the common bile duct (e.g., pancreatic head carcinoma, cholangiocarcinoma), NOT gallstones. Gallstones cause chronic inflammation and fibrosis, making the gallbladder shrunken and unable to distend.
---
## CONCENTRATION OF BILE — MECHANISM
The gallbladder concentrates bile by absorbing **NaCl and water**:
1. **Na⁺** is actively transported out of the cell at the **basolateral membrane** by **Na⁺/K⁺-ATPase**.
2. This creates a low intracellular Na⁺ → Na⁺ enters the cell from the lumen via **Na⁺-H⁺ exchanger** and **Na⁺-Cl⁻ cotransporter** at the apical membrane.
3. **Cl⁻** enters the cell apically (with Na⁺) and exits basolaterally through **Cl⁻ channels**.
4. **Water** follows osmotically — through **aquaporins (AQP1 and AQP8)** and through the paracellular pathway.
5. Net result: Bile is concentrated 5-10 fold; bile salts, cholesterol, bilirubin, and phospholipids increase in concentration.
---
# 5. VERMIFORM APPENDIX
Although not a major digestive organ, the appendix is an organ associated with the GI tract with distinctive histological features.
## HISTOLOGICAL LAYERS
### 1. Mucosa
- **Epithelium**: Simple columnar with goblet cells (similar to the colon — the appendix is a diverticulum of the cecum).
- **No villi** (like the colon).
- **Crypts of Lieberkühn**: Present but shorter and fewer than in the colon.
- **Abundant goblet cells**.
- **Enteroendocrine cells**: Present, including **serotonin (5-HT)-producing enterochromaffin cells** — clinically important because the appendix is the **most common site of carcinoid tumors** in the GI tract.
- **Lamina propria**: Contains **abundant lymphoid tissue** — numerous **lymphoid follicles with prominent germinal centers** that often occupy the full thickness of the mucosa and extend into the submucosa. This lymphoid tissue can be so abundant that it nearly obliterates the lumen.
### 2. Submucosa
- Connective tissue with blood vessels and lymphatics.
- Lymphoid follicles from the mucosa frequently extend into the submucosa.
- **Submucosal (Meissner's) plexus** present.
### 3. Muscularis Externa
- **Inner circular** and **outer longitudinal** smooth muscle layers (complete, unlike the colon where the outer longitudinal layer is condensed into teniae coli).
- **Myenteric (Auerbach's) plexus** between the two layers.
### 4. Serosa
- **Complete serosa** — the appendix is entirely covered by visceral peritoneum (it has a mesoappendix).
### Lumen
- Small, irregular, often **partially or completely obliterated** by lymphoid tissue, especially in children and young adults.
- With aging, the lymphoid tissue regresses and may be replaced by fibrosis; the lumen may become obliterated.
---
## CLINICAL CORRELATIONS — APPENDIX
> **CLINICAL: Acute Appendicitis**
> The most common surgical emergency of the abdomen. Most common cause of obstruction: **fecalith (fecal stone/appendicolith)** in adults; **lymphoid hyperplasia** in children. Obstruction → increased intraluminal pressure → ischemia → bacterial invasion → inflammation → necrosis → perforation → peritonitis. Histologically: **transmural acute inflammation** (neutrophilic infiltrate involving all layers, including the muscularis and serosa — this is the key diagnostic criterion). Serosal surface shows fibrinous/fibrinopurulent exudate. Mucosal ulceration with neutrophilic infiltration of the crypts. **McBurney's point**: point of maximal tenderness (⅓ of the distance from the ASIS to the umbilicus).
> **CLINICAL: Carcinoid Tumor (Well-Differentiated Neuroendocrine Tumor) of the Appendix**
> The **most common tumor of the appendix** and the most common location of carcinoid tumors in the GI tract. Most are small (<2 cm), located at the **tip** of the appendix, and are found **incidentally** during appendectomy. Tumors <2 cm: almost always benign — appendectomy alone is curative. Tumors >2 cm or with mesoappendix invasion: may require right hemicolectomy. Histologically: nests, cords, and rosettes of uniform cells with round nuclei, "salt-and-pepper" chromatin (neuroendocrine chromatin pattern), eosinophilic granular cytoplasm. **IHC**: positive for **chromogranin A, synaptophysin**. Rarely causes **carcinoid syndrome** (flushing, diarrhea, wheezing, right-sided heart disease — from serotonin) because the liver metabolizes serotonin before it reaches the systemic circulation. Carcinoid syndrome occurs only with **liver metastases** (serotonin bypasses hepatic metabolism).
> **CLINICAL: Mucocele of the Appendix**
> Dilatation of the appendix by accumulated mucus. Can be caused by: **mucinous cystadenoma** (benign), **mucinous cystadenocarcinoma** (malignant), or simple mucosal hyperplasia. If the mucocele ruptures, mucus-secreting cells can implant on the peritoneal surface → **pseudomyxoma peritonei** (gelatinous ascites filled with mucin and mucinous epithelial cells). Pseudomyxoma peritonei is more commonly associated with mucinous tumors of the **ovary** and appendix.
---
# 6. TEETH (Brief Overview as Associated Structures)
While teeth are part of the oral cavity rather than a separate organ, they are intimately associated with the digestive tract.
## STRUCTURE
### Enamel
- **Hardest tissue in the body** (96% inorganic — hydroxyapatite crystals).
- Produced by **ameloblasts** (of ectodermal origin — the only component of the tooth derived from ectoderm).
- Ameloblasts are lost after tooth eruption → enamel cannot be regenerated.
- Organized into **enamel rods (prisms)**.
### Dentin
- Forms the bulk of the tooth.
- Harder than bone (70% inorganic).
- Produced by **odontoblasts** (of neural crest/mesenchymal origin).
- Odontoblasts persist in the pulp and can form secondary/reparative dentin throughout life.
- Contains **dentinal tubules** with odontoblast processes (Tomes' fibers).
- Types: Primary, secondary (physiological), tertiary/reparative (in response to injury).
### Pulp
- Central connective tissue containing **blood vessels, nerves, lymphatics**, and **odontoblasts** lining the pulp cavity.
- Loose connective tissue with fibroblasts, undifferentiated mesenchymal cells, macrophages.
### Cementum
- Covers the root.
- Similar to bone but **avascular** (unlike bone).
- Produced by **cementoblasts** (mesenchymal origin).
- **Sharpey's fibers** (from the periodontal ligament) insert into cementum and alveolar bone, anchoring the tooth.
### Periodontal Ligament
- Dense connective tissue between cementum and alveolar bone.
- Contains **principal fibers** (collagen bundles — Sharpey's fibers), fibroblasts, cementoblasts, osteoblasts, undifferentiated mesenchymal stem cells, epithelial rests of Malassez (remnants of Hertwig's epithelial root sheath), blood vessels, and nerves.
- Acts as a **biological shock absorber** and allows limited tooth movement.
> **CLINICAL: Dental Caries**
> Caused by acid produced by oral bacteria (especially *Streptococcus mutans*) from fermentable carbohydrates. Acid demineralizes enamel → cavitation. Can progress through dentin to the pulp → pulpitis → periapical abscess.
> **CLINICAL: Ameloblastoma**
> A benign but locally aggressive odontogenic tumor arising from ameloblast remnants, enamel organ, or lining of odontogenic (dentigerous) cysts. Most common in the **mandible** (posterior body/ramus). Histologically: islands and cords of odontogenic epithelium with peripheral palisading of columnar cells resembling ameloblasts (with reverse polarity — nuclei away from basement membrane) and central stellate reticulum-like cells.
> **CLINICAL: Odontogenic Keratocyst (Keratocystic Odontogenic Tumor)**
> Cystic lesion lined by **parakeratinized stratified squamous epithelium** (thin, uniform, 6-10 cell layers with a corrugated parakeratotic surface). High recurrence rate. Associated with **Gorlin syndrome** (nevoid basal cell carcinoma syndrome — PTCH1 mutation).
---
# SUMMARY OF KEY DISTINGUISHING HISTOLOGICAL FEATURES
| Organ | Key Identifying Feature |
|---|---|
| **Parotid** | Purely serous; abundant adipose tissue; long intercalated ducts |
| **Submandibular** | Mixed (serous predominant); serous demilunes; long striated ducts |
| **Sublingual** | Mixed (mucous predominant); poorly developed duct system; no clear capsule |
| **Pancreas (exocrine)** | Purely serous; **centroacinar cells** (unique!); NO myoepithelial cells; NO striated ducts |
| **Pancreas (endocrine)** | Islets of Langerhans; pale-staining clusters; β cells dominant (60-70%) |
| **Liver** | Hepatocyte plates radiating from central vein; sinusoids with Kupffer cells; portal triads; Space of Disse with stellate cells; bile canaliculi |
| **Gallbladder** | Simple columnar epithelium; mucosal folds (honeycomb); NO muscularis mucosae; NO submucosa; Rokitansky-Aschoff sinuses; randomly oriented smooth muscle |
| **Appendix** | Abundant lymphoid follicles with germinal centers; colonic-type epithelium; complete muscularis externa (unlike colon with teniae coli); small/obliterated lumen |
---
# COMPARATIVE TABLE: DUCT SYSTEMS
| Feature | Salivary Glands | Pancreas |
|---|---|---|
| Intercalated ducts | Present | Present (long) |
| Striated ducts | Present | **ABSENT** |
| Centroacinar cells | **ABSENT** | Present (unique) |
| Myoepithelial cells | Present | **ABSENT** |
| Makes secretion hypotonic | Yes (striated ducts) | No (isotonic) |
---
This comprehensive overview covers the major histological features and clinically relevant correlations of all organs associated with the digestive tract. Each organ's microanatomy has been detailed at the cellular and ultrastructural level, with extensive clinical correlations integrated throughout the text.
Rewrite the whole content as it is plus add maximum number of high yield images along the content from your side