I now have comprehensive, authoritative information from Sabiston, Yamada, and Current Surgical Therapy. Let me compile the full detailed answer.
Ischemic Colitis — Comprehensive Review
1. Definition & Epidemiology
Definition
Ischemic colitis (IC) is a condition in which blood supply to colonocytes fails to meet metabolic demands, resulting in a spectrum of injury ranging from mucosal ischemia to transmural infarction and perforation. It is the most common form of gastrointestinal ischemia, and it differs fundamentally from acute mesenteric ischemia (AMI) in that it is primarily a small-vessel disease rather than a major-vessel occlusive event, and it seldom requires vascular intervention.
Injury occurs by two mechanisms:
- Initial hypoperfusion phase — mucosal ischemia begins within 20 minutes to 1 hour of reduced blood flow; transmural infarction occurs within 8–16 hours of sustained ischemia.
- Reperfusion injury — restoration of blood flow generates reactive oxygen species causing lipid peroxidation and cell necrosis.
Spectrum of severity:
| Depth of injury | Outcome |
|---|
| Mucosal only | Reversible |
| Mucosal + submucosal | Potential stricture formation |
| Transmural | Infarction, perforation, sepsis, death |
Epidemiology
- Incidence: 4.5–44 cases per 100,000 person-years (ranges vary by study); a large US insurance-claims study reported 7.1 per 100,000; another estimated 10.4 per 100,000 inhabitants.
- Incidence is increasing over the last three decades.
- Predominantly affects patients >60 years of age; the 70–79 age group has a relative risk 3.69× higher than the 50–59 group.
- Slight female predominance.
- About 20% of patients require operative intervention, usually emergent.
- Overall in-hospital mortality: ~12.7% (surgical cases: ~39.3%; medically managed: ~6.2%).
— Current Surgical Therapy 14e; Yamada's Textbook of Gastroenterology 7e; Sabiston Textbook of Surgery
2. Causes & Risk Factors
Pathomechanisms
IC is classified by mechanism of blood flow reduction:
- Non-occlusive (most common): Low-flow states — shock, sepsis, congestive heart failure, drugs, colon obstruction.
- Occlusive vascular: Arterial thrombosis, embolism, or venous occlusion.
- Postoperative: Following aortic (especially abdominal aortic aneurysm repair) or cardiac surgery — intraoperative cessation of blood flow, sacrifice of the IMA, or prolonged cross-clamp time.
During hypotension, splanchnic blood flow is preferentially redirected to the brain. At the histologic level, initial ischemic changes always begin in the mucosa on the antimesenteric side, then spread transmurally if the insult continues.
Risk Factors (Box 95.6, Sabiston)
Low-flow states:
- Septic shock, congestive heart failure, hemorrhagic shock, hypotension
Atherosclerotic disease:
- Ischemic heart disease, cerebrovascular disease, peripheral vascular disease
Gastrointestinal:
- Constipation, diarrhea, irritable bowel syndrome
- Obstructing lesions: volvulus, carcinoma, diverticulitis
- Fecal impaction
Surgery / Invasive interventions:
- Abdominal aortic aneurysm repair (highest risk)
- Cardiovascular surgery
- Endovascular abdominal interventions (chemoembolization)
- Post-colonoscopy (air insufflation raises intraluminal pressure)
Cardiovascular/Pulmonary:
- COPD, atrial fibrillation, hypertension
Metabolic/Rheumatologic:
- Diabetes mellitus, dyslipidemia
- Systemic lupus erythematosus, rheumatoid arthritis
Miscellaneous:
- Hypercoagulable states (thrombophilia)
- Sickle cell disease
- Long-distance running ("steal phenomenon" — exercise-induced splanchnic vasoconstriction)
- COVID-19 (recently identified association)
Drugs associated with IC:
- Constipation-inducing drugs (opioids and non-opioids)
- Cocaine and methamphetamines
- Immunomodulatory drugs
- Oral contraceptives
- Triptans
- Angiotensin-converting enzyme inhibitors / angiotensin receptor blockers
- NSAIDs
- Chemotherapy agents (e.g., taxanes, bevacizumab)
Recurrent bouts occur in up to 15% of patients; smoking, COPD, and peripheral vascular disease predispose to recurrence.
— Sabiston Textbook of Surgery; Yamada's Textbook of Gastroenterology 7e
3. Watershed Areas of the Colon
The colon receives its blood supply from:
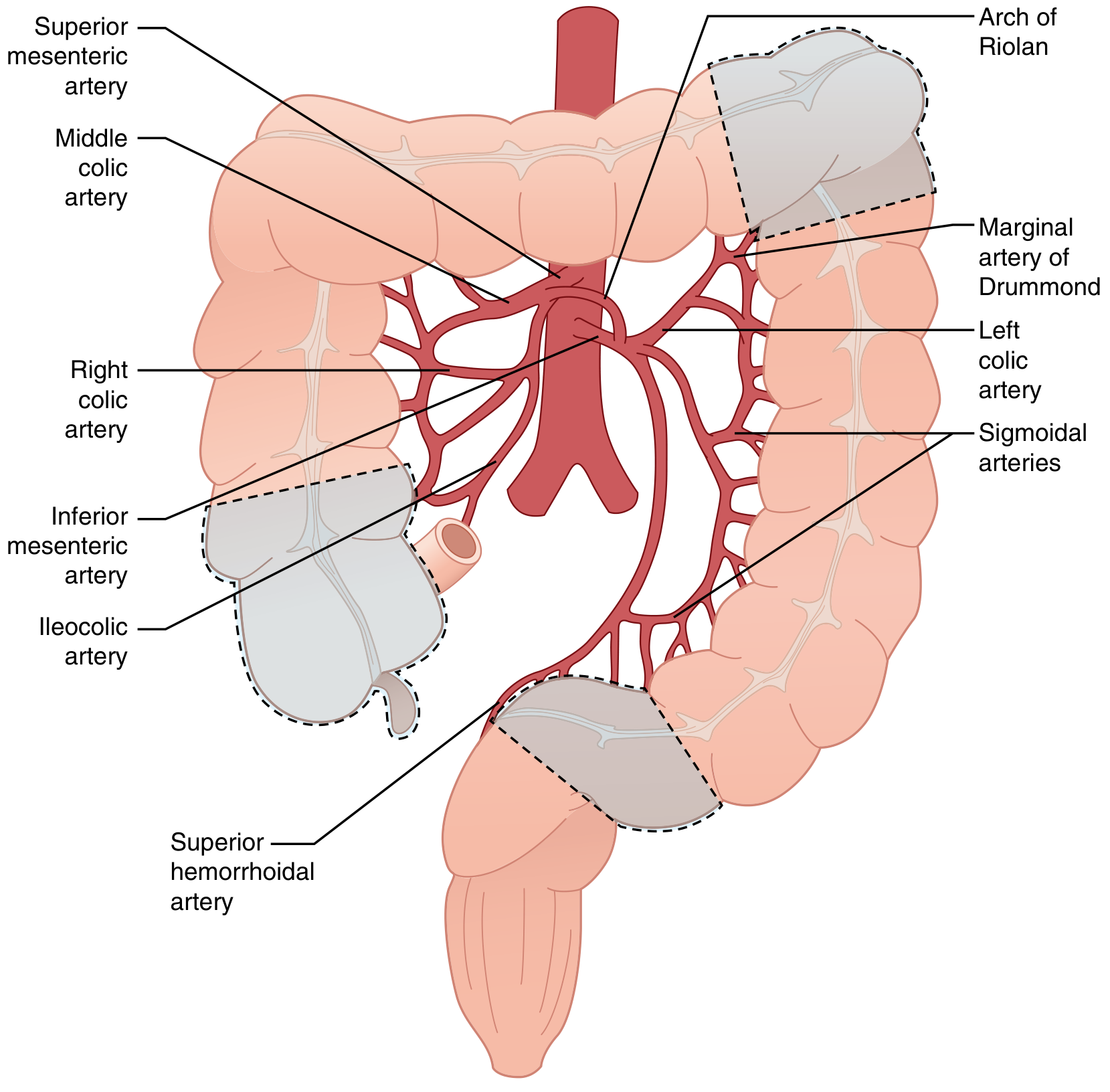
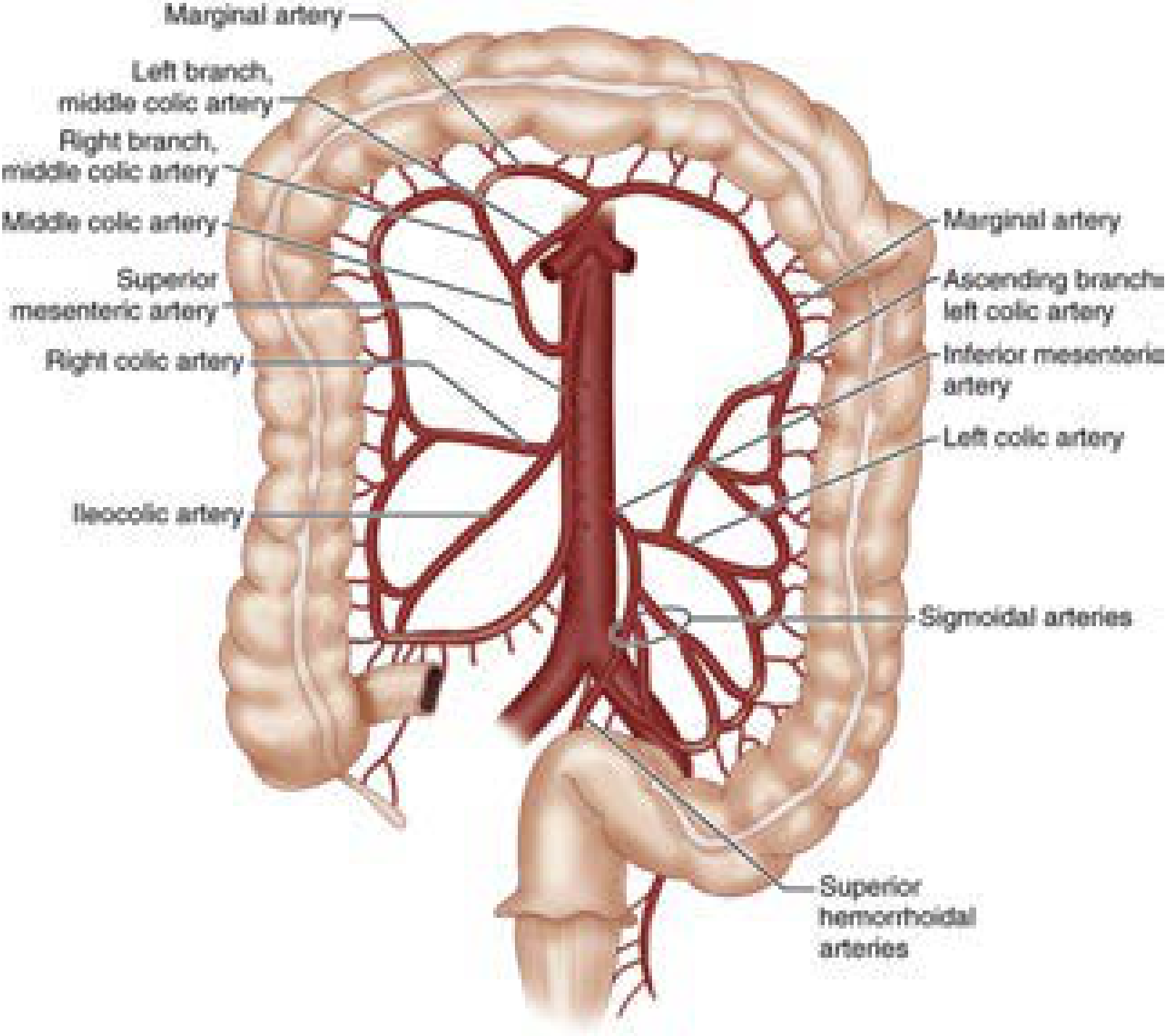
- Superior mesenteric artery (SMA): ileocolic, right colic, middle colic arteries → cecum, ascending colon, proximal 2/3 transverse colon
- Inferior mesenteric artery (IMA): left colic, sigmoid arteries, superior rectal artery → distal transverse colon, descending colon, sigmoid, upper rectum
- Internal iliac arteries: middle and inferior rectal arteries → rectum (hence rectum is relatively protected)
Collateral networks:
- Marginal artery of Drummond — runs parallel to the mesenteric margin from cecocolic to rectosigmoid junction; absent at the splenic flexure in up to 18–50% of individuals.
- Arc of Riolan (meandering mesenteric artery) — an inconsistent but critical collateral connecting SMA/middle colic to IMA/left colic at the mesenteric root; its presence often signals occlusion of one of the major trunks.
Watershed areas of the colon — Sabiston Textbook of Surgery
Colonic blood supply: SMA and IMA territories — Current Surgical Therapy 14e
The Two Classic Watershed Areas
| Watershed Point | Location | Significance |
|---|
| Griffiths' point | Splenic flexure (junction of SMA & IMA territories) | Most vulnerable; marginal artery absent in 18–50%; accounts for ~majority of IC cases |
| Sudeck's point | Rectosigmoid junction (junction of IMA & superior rectal artery) | Second most vulnerable area |
Together, these two points account for approximately 80% of all IC cases.
The rectum is infrequently affected because it receives dual blood supply from both the IMA (superior rectal) and the internal iliac arteries (middle and inferior rectal). Surgeons deliberately avoid anastomoses at the splenic flexure because the impaired blood supply risks anastomotic failure.
— Current Surgical Therapy 14e; Sabiston Textbook of Surgery
4. Clinical Features
Subtypes / Clinical Presentations
1. Transient ulcerating ischemic colitis (most common)
- Acute onset in elderly patients with or without predisposing factors
- Classic triad: crampy abdominal pain + urgent desire to defecate + passage of bright red or maroon blood per rectum (blood usually mixed with stool)
- Overall blood loss is small; transfusion rarely required
- Later: abdominal distension, ileus, nausea, vomiting
- Physical examination: tenderness or vague mass palpable along the affected colonic segment
- Peritoneal signs (transmural infarction) present in ~15% — accompanied by leukocytosis, metabolic acidosis, elevated lactate
2. Reversible ischemic colopathy
- Milder, more transient form
- Common with drug-induced ischemia
3. Segmental ulcerating colitis with stricture formation
- More chronic, indolent course
- Mild abdominal discomfort with intermittent diarrhea; blood may or may not be apparent
- Some patients are minimally symptomatic — discovered incidentally at endoscopy
- Risk of evolution to fibrotic stricture (may or may not cause obstructive symptoms)
- Systemic signs (fever, leukocytosis, bacteremia) signal risk of perforation → surgical resection indicated
4. Fulminant universal ischemic colitis (most severe)
- May involve the entire colon
- Systemically very ill patient
- Marked abdominal distension, leukocytosis, elevated lactate, metabolic acidosis
- High risk of transmural perforation and death
Key Clinical Pointers
- Left colon is more commonly affected than right colon; splenic flexure is most susceptible
- Rectum is typically spared (dual blood supply)
- Segmental distribution with normal-appearing colon proximal and distal to the affected segment
- Unlike AMI, pain is usually not out of proportion to physical findings (AMI presents with severe pain disproportionate to exam)
— Yamada's Textbook of Gastroenterology 7e; Current Surgical Therapy 14e
5. Investigations
Laboratory Tests
- CBC: Leukocytosis (elevated WBC correlates with severity)
- Metabolic panel: Metabolic acidosis (decreased bicarbonate), elevated BUN
- Lactate: Elevated — marker of severe ischemia; peak lactate >2.5 mmol/L predicts worse surgical outcome
- LDH: Elevated lactate dehydrogenase — associated with severe disease
- Albumin: Decreased in severe disease
- Haemoglobin: Decreased
- Stool studies: C. difficile toxin, ova & parasites, culture & sensitivity — to exclude infectious etiology
Plain Abdominal Radiograph (AXR)
- Abnormal in ~1/5 of patients
- "Thumbprinting" — rounded densities along the sides of gas-filled colon, representing submucosal edema (classic but non-specific)
- Bowel distension; air-fluid levels
- Free air → perforation → immediate surgery
CT Abdomen (Primary Imaging Modality)
Performed with IV and oral contrast — first-line investigation.
| CT Finding | Significance |
|---|
| Segmental bowel wall thickening | Most common finding (detected in up to 89%) |
| Pericolonic fat stranding | Supportive |
| Thumbprinting | Submucosal edema |
| Pneumatosis intestinalis | Gas in the bowel wall — suggests transmural disease / infarction |
| Portal venous gas | Severe transmural disease → immediate surgery |
| Absence of bowel wall enhancement | Transmural ischemia/infarction |
| Intraperitoneal fluid | Predicts need for delayed surgery |
CT angiography (multiphasic) should be performed in cases of severe pain out of proportion to findings or isolated right colon ischemia — to exclude proximal AMI (occlusion of ileocolic branch of SMA).
Colonoscopy (Gold Standard for Diagnosis)
- Should be performed within 48 hours of presentation
- Avoid in: acute peritonitis, suspected severe transmural ischemia (risk of perforation)
- Perform without or with minimal bowel preparation (left colon most affected — sigmoidoscopy often suffices in critically ill patients)
- Do not overinsufflate; do not advance scope beyond the most distal extent of disease
Colonoscopic findings:
- Edematous, friable mucosa
- Erythema and petechial haemorrhage
- Mucosal ulceration
- "Single-stripe sign" — single linear ulcer running along the longitudinal colonic axis; rare but specific for IC
- Segmental distribution with abrupt transition between injured and normal mucosa
- Sparing of the rectum (supports ischemia over IBD)
- Severe cases: areas of gangrene (dark-blue/black mucosa)
- Biopsy: acute phase — crypt destruction, haemorrhage, capillary thrombosis; chronic phase — granulation tissue, atrophy, fibrosis
Endoscopy cannot reliably distinguish partial-thickness from full-thickness ischemia — clinical and CT correlation is essential.
Angiography
- Rarely indicated (IC is primarily a small-vessel disease; major trunks usually intact)
- Exception: concomitant AMI, isolated right-sided colitis, sudden-onset severe pain
MRI
- Alternative to CT; useful for grading severity; avoids radiation
- Less commonly used in acute presentations
— Sabiston Textbook of Surgery; Yamada's Textbook of Gastroenterology 7e
6. Medical Management
The majority (~80%) of patients respond to conservative management.
General Supportive Measures
- Bowel rest (nil by mouth)
- IV fluid resuscitation — aggressive, especially in low-flow states; correct hypovolemia and hypotension
- Nasogastric tube — if ileus is present
- Optimise underlying conditions — heart failure, sepsis, arrhythmias, diabetes
Antibiotics
- Broad-spectrum antibiotics covering aerobic and anaerobic Gram-negative organisms — prescribed empirically because colonic ischemia disrupts the epithelial barrier, allowing bacterial translocation and sepsis
- Appropriate initial choice: piperacillin-tazobactam or a combination of a 3rd-generation cephalosporin + metronidazole
Vasoactive / Adjunct Therapies
- Phosphodiesterase type 5 (PDE5) inhibitors — may improve colonic blood flow
- Pentoxifylline — improves red blood cell deformability and microcirculatory flow
- Prostaglandin E1 — promotes mucosal healing
Cardiovascular Evaluation
- Evaluate for embolic source (arrhythmia, dilated cardiomyopathy) — may require anticoagulation
- Correct atrial fibrillation if present
Monitoring
- Serial abdominal examinations
- Repeat CT if clinical deterioration
- Early colonoscopy to confirm diagnosis and assess extent
- ICU-level monitoring in severe/complicated cases
Treatment of Complications
- Colonic stricture (chronic sequela): observation, endoscopic dilation, or surgical resection (depending on symptoms)
- Bleeding from ischemic ulcers: endoscopic haemostatic powder spray may be used for palliation
The decision to escalate to surgery is triggered by: peritonitis, deterioration despite 24–48 hours of medical management, massive bleeding, or imaging showing pneumatosis/portal venous gas.
— Sabiston Textbook of Surgery; Yamada's Textbook of Gastroenterology 7e; Current Surgical Therapy 14e
7. Surgical Management
Indications for Emergency Surgery
- Peritonitis on physical examination
- Massive lower GI bleeding not controlled by other means
- Fulminant colitis with systemic deterioration
- Pneumatosis intestinalis or portal venous gas on imaging with clinical picture of IC
- Worsening clinical condition despite maximal medical management
- Free intraperitoneal air (perforation)
Operative Principles
Access: Midline laparotomy is standard; diagnostic laparoscopy may be appropriate in selected cases (intraperitoneal pressure must be kept ≤10–15 mmHg to avoid worsening ischemia).
Resection:
- Remove all grossly ischemic colonic segments
- The serosa may appear normal even with transmural necrosis — so do not rely on serosal appearance alone
- Use intraoperative adjuncts to assess viability: Doppler ultrasonography, intraoperative colonoscopy, photoplethysmography
- A preoperative CT or endoscopic evaluation is critical to define extent of involvement
Anastomosis vs. Ostomy:
| Situation | Recommended approach |
|---|
| Isolated right colon ischemia, well-perfused remaining bowel | Primary anastomosis can be performed safely |
| Left-sided IC (most common scenario) | Hartmann procedure — end colostomy + rectal stump closure |
| Left-sided IC with favourable conditions | Primary anastomosis ± protective diverting loop ileostomy |
If ongoing ischemia is suspected after resection: leave fascia open, bowel in discontinuity → ICU for resuscitation → planned second-look laparotomy at 12–48 hours to assess viability and achieve definitive closure.
Hartmann reversal: No sooner than 6–8 weeks after the index operation; carries significant complication rates (longer stay, higher risk of anastomotic leak) in this population.
Indications for Elective Surgery (Sequelae)
- Symptomatic colonic stricture — after failed conservative management or dilation
- Ostomy reversal — after full recovery
Postoperative Course & Morbidity
- 2/3 of patients requiring surgery for severe IC develop medical complications: pneumonia, UTI, atrial fibrillation, myocardial infarction, acute renal failure, dialysis requirement
- 37% in-hospital mortality for severe IC requiring surgery
Independent risk factors for post-colectomy mortality:
- Elderly age and poor functional status
- Multiple comorbidities
- Low-output heart failure (EF <20%)
- Preoperative septic shock
- Preoperative blood transfusions
- Preoperative acute renal failure
- Delay from admission to surgery
- Peak preoperative lactate >2.5 mmol/L
- Subtotal or total colectomy required
- Intraoperative catecholamine administration
- ASA class 4
— Current Surgical Therapy 14e; Sabiston Textbook of Surgery
8. Prognosis
Overall Outcomes
- Overall mortality: 12.7% (systematic review)
- Medically managed (mild-moderate disease): mortality ~6.2%
- Surgically managed: mortality ~39.3%
- Population-level overall mortality rate: 1.54 per 100,000 persons
Predictors of Poor Outcome
| Factor | Significance |
|---|
| Right colon involvement | Most significant predictor of poor outcome; highest mortality (20.3% vs. 9%); associated with coronary artery disease, end-stage renal failure |
| Intraperitoneal fluid on CT | Predicts need for subsequent surgery |
| Absence of rectal bleeding | Paradoxically worsens prognosis (suggests more severe disease without mucosal blood escape) |
| Peripheral vascular disease | Predicts need for surgery |
| Atrial fibrillation | Predicts surgery requirement |
| ICU admission | Marker of severity |
| Elevated lactate on admission | Major prognostic marker |
| Peritoneal signs at onset | Unfavourable course |
| Severe pain without bleeding | Suggests transmural ischemia — unfavourable |
| Extensive bowel ischemia | High perioperative mortality |
| Non-occlusive ischemic colitis | Poor long-term survival |
| Acute renal failure | Poor perioperative prognosis |
| High mesenteric atherosclerosis burden (in resected specimen) | Poor long-term survival |
| Coexisting small bowel ischemia (~15% of cases) | Worse prognosis |
Additional Prognostic Considerations
- Right-sided IC carries a distinct presentation and worse outcome; some experts regard right- and left-sided IC as separate entities.
- Ischemic bowel disease predisposes to C. difficile infection among inpatients, which worsens mortality.
- Vascular and metabolic comorbidities significantly worsen outcomes.
- Recurrence occurs in up to 15% — particularly in patients with smoking, COPD, and peripheral vascular disease.
— Yamada's Textbook of Gastroenterology 7e; Current Surgical Therapy 14e; Sabiston Textbook of Surgery
Sources
- Current Surgical Therapy, 14th Edition — Alsaad & Lipsett, Ischemic Colitis
- Sabiston Textbook of Surgery, The Biological Basis of Modern Surgical Practice — Chapter 95
- Yamada's Textbook of Gastroenterology, 7th Edition — Chapter 114, Ischemic Colitis
- Schwartz's Principles of Surgery, 11th Edition — Chapter on Ischemic Colitis