define blood pressure normal values of blood pressure describe regulation of BP by Baroreceptor essay
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive, authoritative content from multiple textbooks plus three excellent diagrams. Let me compose the full essay.
Blood Pressure: Definition, Normal Values, and Regulation by Baroreceptors
1. Definition of Blood Pressure
Blood pressure (BP) is the lateral pressure exerted by the flowing blood on the walls of blood vessels. More precisely, it is the force per unit area that the blood exerts against the arterial wall. It is generated by the pumping action of the heart and is maintained by the resistance of the peripheral vasculature.
BP is expressed as two values:
- Systolic BP (SBP) — the peak pressure in the arteries during ventricular contraction (systole).
- Diastolic BP (DBP) — the minimum pressure during ventricular relaxation (diastole).
A third derived value is the Mean Arterial Pressure (MAP), which represents the average driving pressure throughout the cardiac cycle:
MAP = Diastolic pressure + 1/3 × Pulse pressure
or
MAP = 1/3 SBP + 2/3 DBP
Pulse Pressure = SBP − DBP (normally ~40 mm Hg).
The fundamental determinants of BP are:
BP = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
(Roberts and Hedges' Clinical Procedures in Emergency Medicine; Costanzo Physiology 7th Ed.)
2. Normal Values of Blood Pressure
Adults
| Classification (JNC 7) | SBP (mm Hg) | DBP (mm Hg) | |
|---|---|---|---|
| Normal | < 120 | and | < 80 |
| Prehypertension | 120–139 | or | 80–89 |
| Stage 1 Hypertension | 140–159 | or | 90–99 |
| Stage 2 Hypertension | ≥ 160 | or | ≥ 100 |
(Comprehensive Clinical Nephrology, 7th Ed., Table 34.2)
Key reference values in adults:
- Optimal BP: 115/75 mm Hg — associated with minimal vascular mortality.
- Normal SBP range: 90–140 mm Hg.
- Normal DBP range: 60–90 mm Hg.
- Normal MAP: ~93 mm Hg (at a BP of ~120/80 mm Hg).
The ACC/AHA 2017 guideline redefined hypertension as ≥ 130/80 mm Hg (Stage 1 ≥ 130/80; Stage 2 ≥ 140/90), which increased the prevalence of hypertension in US adults to 46%.
In geriatric trauma patients, SBP readings of 90–120 mm Hg may represent occult hypoperfusion and increased mortality — standard hypotension thresholds must be re-evaluated in this population.
(Roberts and Hedges' Clinical Procedures in Emergency Medicine; Comprehensive Clinical Nephrology)
3. Regulation of Blood Pressure by Baroreceptors
3.1 Overview of Neural Regulation
Blood pressure is regulated on two timescales:
- Short-term (seconds to minutes): Neural pathways — primarily baroreceptor reflexes — targeting the heart, vessels, and adrenal medulla.
- Long-term (hours to days): Hormonal and renal mechanisms (renin–angiotensin–aldosterone system, fluid balance).
The baroreceptor reflex is the most important short-term BP regulator, operating as a negative-feedback loop that continuously adjusts cardiovascular output to maintain mean arterial pressure at a set point (~100 mm Hg).
(Medical Physiology, Boron & Boulpaep; Costanzo Physiology 7th Ed.)
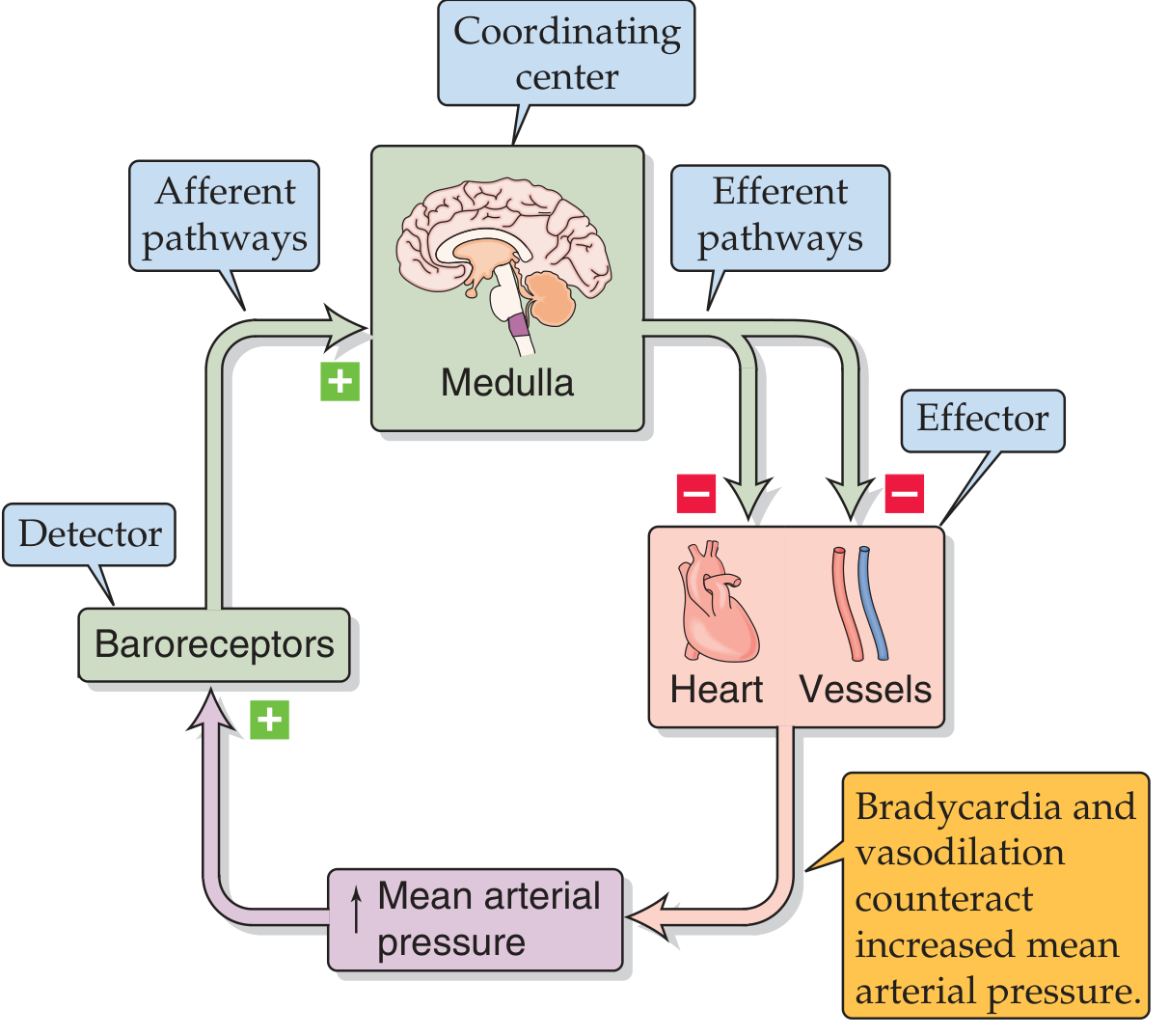
3.2 The Baroreceptor Reflex Arc
The complete reflex arc consists of five components:
| Component | Structure |
|---|---|
| Detector | Baroreceptors (carotid sinus, aortic arch) |
| Afferent pathways | CN IX (glossopharyngeal), CN X (vagus) |
| Coordinating center | Nucleus tractus solitarius → CVLM → RVLM (medulla) |
| Efferent pathways | Sympathetic and parasympathetic outflow |
| Effectors | SA node, cardiac muscle, arterioles, veins, adrenal medulla |
3.3 The Baroreceptors (Sensors)
Baroreceptors are mechanoreceptors (stretch receptors) located in the walls of:
- Carotid sinus — a dilation of the internal carotid artery just above the bifurcation of the common carotid. These receptors respond to both increases and decreases in arterial pressure.
- Aortic arch — receptors here are primarily responsive to increases in arterial pressure.
Mechanism of action:
- An increase in arterial pressure stretches the vessel wall → depolarizes the mechanoreceptor membrane (receptor potential) → increases action potential firing frequency in afferent nerves.
- A decrease in arterial pressure → less stretch → decreased firing rate (approaches zero below ~40–60 mm Hg).
- Baroreceptors are more sensitive to pulsatile (changing) pressure than to constant pressure. The strongest stimulus is a rapid change in arterial pressure.
- The response is biphasic: an initial large dynamic depolarization followed by a smaller, sustained static depolarization — encoding both rate-of-change and absolute magnitude of pressure.
Threshold for carotid sinus nerve activity: ~50 mm Hg
Maximum activity: ~200 mm Hg
At normal mean BP (~100 mm Hg), bursts of action potentials appear during systole with few spikes in early diastole.
(Costanzo Physiology 7th Ed.; Ganong's Review of Medical Physiology 26th Ed.; Medical Physiology)
3.4 Afferent Pathways
- Carotid sinus baroreceptors → carotid sinus nerve (branch of CN IX, glossopharyngeal nerve) → medulla.
- Aortic arch baroreceptors → aortic depressor nerve (branch of CN X, vagus nerve) → medulla.
These afferent fibers release glutamate at their first synapse in the Nucleus Tractus Solitarius (NTS) — the primary integration center in the brainstem.
(Ganong's Review of Medical Physiology 26th Ed.; Costanzo Physiology 7th Ed.)
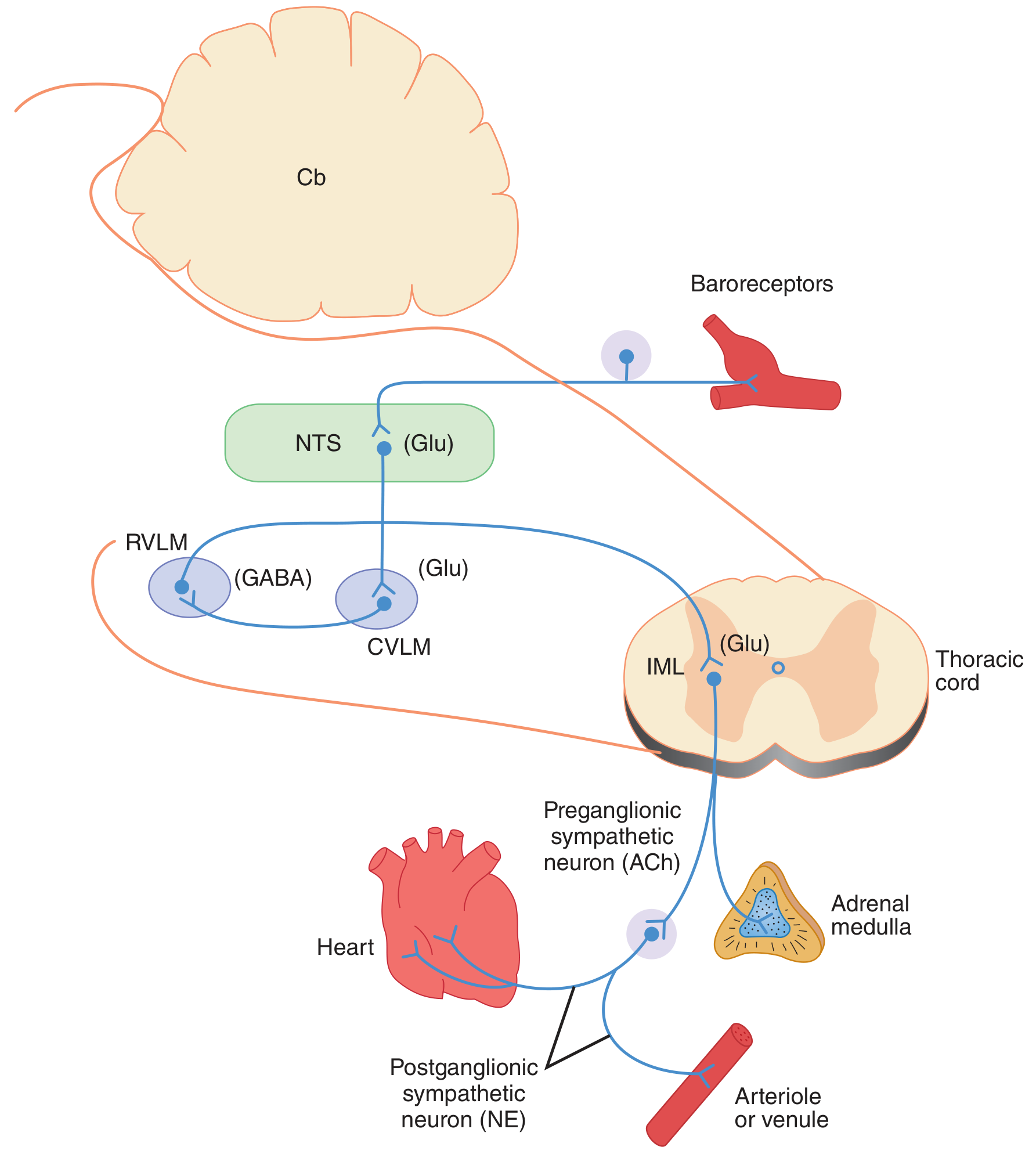
3.5 The Central Coordinating Center (Medulla)
The NTS processes baroreceptor input and directs responses through several medullary cardiovascular centers:
-
Nucleus Tractus Solitarius (NTS): First relay station. Glutamatergic input from baroreceptors → excites NTS neurons → activates CVLM.
-
Caudal Ventrolateral Medulla (CVLM): Receives excitatory input from NTS → releases GABA to inhibit RVLM.
-
Rostral Ventrolateral Medulla (RVLM): The major vasomotor center — source of tonic sympathetic outflow to the cardiovascular system. When inhibited by CVLM (in response to high BP), sympathetic tone is reduced.
-
Nucleus Ambiguus / Dorsal Motor Nucleus: Receive excitatory projections from NTS → increase vagal (parasympathetic) outflow to the heart.
Summary of medullary circuit:
↑BP → ↑Baroreceptor firing → ↑NTS (glutamate) → ↑CVLM (glutamate) → ↑RVLM inhibition (GABA) → ↓Sympathetic outflow
AND: ↑NTS → ↑Vagal motor neurons → ↑Parasympathetic outflow
↑BP → ↑Baroreceptor firing → ↑NTS (glutamate) → ↑CVLM (glutamate) → ↑RVLM inhibition (GABA) → ↓Sympathetic outflow
AND: ↑NTS → ↑Vagal motor neurons → ↑Parasympathetic outflow
(Ganong's Review of Medical Physiology 26th Ed.)
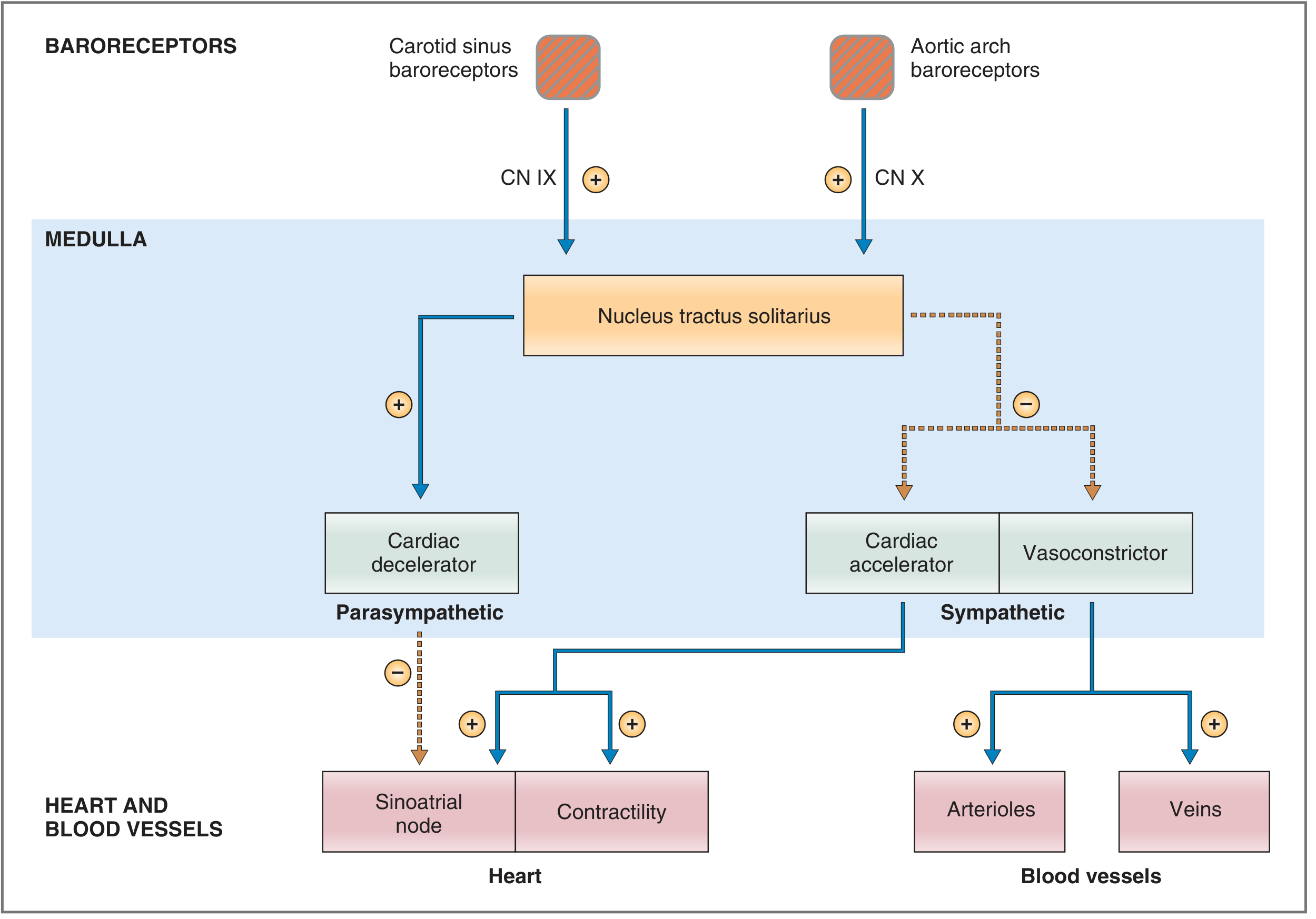
3.6 Efferent Responses
The medullary centers coordinate three cardiovascular centers via the autonomic nervous system:
| Center | Division | Synapse Path | Effect |
|---|---|---|---|
| Cardiac decelerator | Parasympathetic | Vagus → SA node | ↓ Heart rate |
| Cardiac accelerator | Sympathetic | Spinal cord → sympathetic ganglia → SA node/AV node/myocardium | ↑ Heart rate, ↑ contractility |
| Vasoconstrictor (C1) | Sympathetic | Spinal cord → sympathetic ganglia → arterioles + veins | Vasoconstriction / venodilation |
3.7 Integrated Baroreceptor Response
Response to INCREASED Arterial Pressure (e.g., hypertensive stimulus):
- ↑ Pa → ↑ stretch on carotid sinus and aortic arch baroreceptors
- ↑ Firing frequency in CN IX and CN X afferents
- NTS senses Pa > set-point → coordinates response:
- ↑ Parasympathetic outflow (vagus → SA node) → ↓ Heart rate
- ↓ Sympathetic outflow to SA node → further ↓ Heart rate
- ↓ Sympathetic outflow to myocardium → ↓ Contractility → ↓ Stroke volume
- ↓ Sympathetic outflow to arterioles → Vasodilation → ↓ TPR
- ↓ Sympathetic outflow to veins → Venodilation → ↑ unstressed volume → ↓ stressed volume → ↓ venous return
- Net effect: ↓ CO + ↓ TPR → ↓ MAP back to set-point
Response to DECREASED Arterial Pressure (e.g., hemorrhage):
- ↓ Pa → ↓ stretch on baroreceptors → ↓ afferent firing
- NTS senses Pa < set-point:
- ↓ Parasympathetic outflow → ↑ Heart rate
- ↑ Sympathetic outflow → ↑ Heart rate + ↑ Contractility → ↑ CO
- ↑ Sympathetic outflow to arterioles → Vasoconstriction → ↑ TPR
- ↑ Sympathetic outflow to veins → Venoconstriction → ↑ venous return → ↑ CO (Frank-Starling)
- Net effect: ↑ CO + ↑ TPR → ↑ MAP back to set-point
3.8 Sensitivity and Resetting
- Baroreceptors are more sensitive to rapid changes in pressure than to gradual or sustained changes.
- In chronic hypertension, the baroreceptors undergo resetting — they adapt to the elevated baseline and no longer recognize it as abnormal. The set-point in the medullary centers is effectively raised. This explains why the baroreceptor reflex maintains rather than corrects chronic hypertension.
- A decline in pulse pressure (without change in mean pressure) reduces baroreceptor discharge and provokes a compensatory rise in BP and tachycardia.
(Costanzo Physiology 7th Ed.; Ganong's Review of Medical Physiology)
3.9 Clinical Test: Valsalva Maneuver
The Valsalva maneuver (forced expiration against a closed glottis — as in coughing, defecation, or heavy lifting) is used to test baroreceptor reflex integrity:
- ↑ Intrathoracic pressure → ↓ Venous return → ↓ CO → ↓ Pa
- If reflex intact: baroreceptors detect ↓ Pa → ↑ sympathetic + ↓ parasympathetic outflow → ↑ Heart rate (detected clinically)
- On maneuver release: venous return rebounds → ↑ CO → ↑ Pa → baroreceptors detect rise → ↓ Heart rate
A normal Valsalva response (tachycardia then bradycardia) confirms intact baroreceptor reflex function.
(Costanzo Physiology 7th Ed.)
4. Summary Table
| Feature | Detail |
|---|---|
| Normal adult BP | < 120/80 mm Hg (optimal ~115/75) |
| Hypertension threshold (JNC 7) | ≥ 140/90 mm Hg |
| Hypertension threshold (ACC/AHA 2017) | ≥ 130/80 mm Hg |
| Baroreceptor locations | Carotid sinus (CN IX), Aortic arch (CN X) |
| Receptor type | Mechanoreceptors / stretch receptors |
| Afferent neurotransmitter | Glutamate (at NTS) |
| CNS relay | NTS → CVLM (GABA) → RVLM → IML |
| Parasympathetic effect | ↓ Heart rate (via vagus → SA node) |
| Sympathetic effect | ↑ HR + contractility + vasoconstriction + venoconstriction |
| Response to ↑ BP | Bradycardia + vasodilation → ↓ BP |
| Response to ↓ BP | Tachycardia + vasoconstriction → ↑ BP |
| Resetting in hypertension | Set-point shifts upward; reflex maintains high BP |
| Clinical test | Valsalva maneuver |
References:
- Costanzo Physiology, 7th Ed., Ch. 4 — Baroreceptor Reflex
- Medical Physiology, Boron & Boulpaep — Ch. 23: Neural Regulation of Blood Pressure
- Ganong's Review of Medical Physiology, 26th Ed. — Ch. 32: Baroreceptors
- Roberts and Hedges' Clinical Procedures in Emergency Medicine — Normal BP Values
- Comprehensive Clinical Nephrology, 7th Ed. — Table 34.2: JNC 7 BP Classification
This is a shared conversation. Sign in to Orris to start your own chat.