65 year old female with pluritc chest pain and elevated d dimer
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I have all the information needed for a thorough, authoritative response. Here it is:
Clinical Assessment: 65F with Pleuritic Chest Pain + Elevated D-dimer
This presentation is suspicious for pulmonary embolism (PE) until proven otherwise. Here is a systematic approach.
Step 1: Calculate the Wells Score for PE
The Wells criteria determine pre-test probability and guide your next steps:
| Clinical Variable | Points |
|---|---|
| Signs/symptoms of DVT | 3.0 |
| Alternative diagnosis less likely than PE | 3.0 |
| Heart rate >100/min | 1.5 |
| Immobilization >3 days or surgery within 4 weeks | 1.5 |
| Prior PE or DVT | 1.5 |
| Hemoptysis | 1.0 |
| Cancer | 1.0 |
Score interpretation:
- ≤4 = PE unlikely
-
4 = PE likely (proceed directly to CT-PA)
Step 2: Interpret the D-dimer in This Patient
A 65-year-old requires an age-adjusted D-dimer threshold - this is a key point for this patient's age:
"The upper limit of normal for D-dimer was considered to be 500 ng/mL; however, guidelines now recommend use of an age-adjusted D-dimer when ruling out acute PE. The age-adjusted D-dimer applies to patients older than 50 years of age with low or intermediate clinical probability."
Formula: Age × 10 = upper limit of normal (ng/mL)
For this 65-year-old: 65 × 10 = 650 ng/mL is the adjusted cutoff
- If D-dimer is elevated but below 650 ng/mL AND Wells score is low/intermediate - this can still rule out PE
- If above 650 ng/mL with any clinical suspicion - imaging is required
Using the age-adjusted D-dimer reduces the number of CT pulmonary angiograms ordered without missing clinically significant PE. (Harrison's Principles of Internal Medicine 22E, p. 2203)
Also note: The D-dimer is not specific. It rises in MI, pneumonia, sepsis, cancer, post-op states, and advancing age - making it less useful as a rule-in test in a 65-year-old. - Harrison's, p. 2203
Step 3: Diagnostic Algorithm
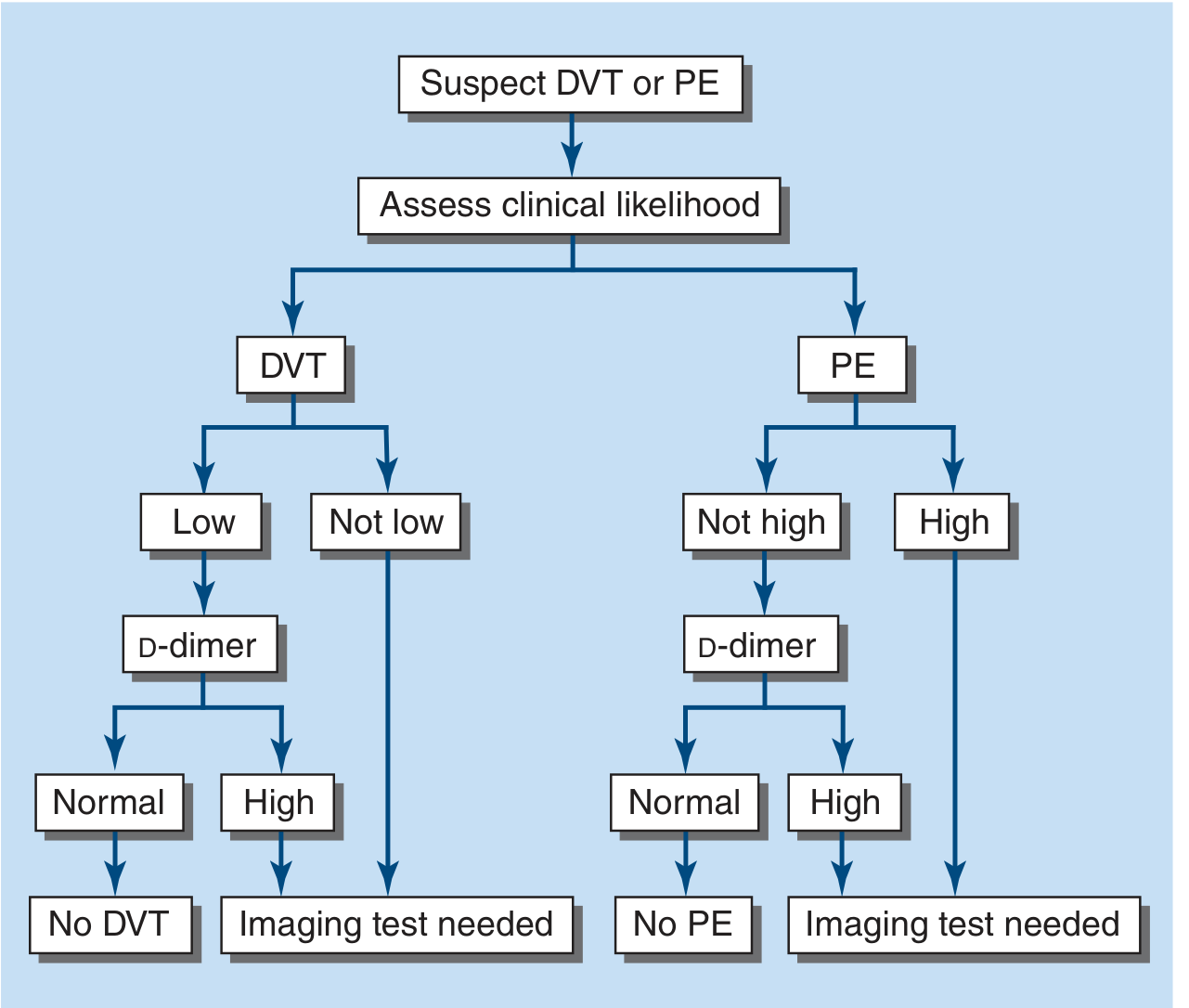
Figure 290-10 from Harrison's 22E: Decision-making for suspected DVT or PE
| Scenario | Action |
|---|---|
| Wells ≤4 AND D-dimer < age-adjusted cutoff | PE excluded - no imaging needed |
| Wells ≤4 AND D-dimer ≥ cutoff | CT pulmonary angiography (CT-PA) |
| Wells >4 (PE likely) | CT-PA directly - do not rely on D-dimer |
| Hemodynamically unstable | Emergent echo or CT-PA, consider empiric anticoagulation |
Step 4: Imaging
CT Pulmonary Angiography (CT-PA) is the principal imaging test for PE. It provides:
- High resolution (≤1 mm, visualizing 6th-order branches)
- Assessment of RV size (RV:LV ratio >1 indicates increased 30-day mortality)
- Alternative diagnoses if PE is absent (pneumonia, aortic pathology, malignancy)
V/Q scan is second-line, used when the patient cannot tolerate IV contrast (e.g., contrast allergy, severe CKD). (Harrison's, p. 2204)
Step 5: Additional Workup
| Test | Finding in PE |
|---|---|
| ECG | Sinus tachycardia most common; S1Q3T3 pattern (specific but insensitive); T-wave inversions V1-V4 suggest RV strain |
| Troponin | Elevated due to RV microinfarction |
| BNP/NT-proBNP | Elevated due to myocardial stretch from RV dilation |
| CXR | Often normal or near-normal; Westermark's sign (focal oligemia), Hampton's hump (peripheral triangular density at pleural base) |
| Leg ultrasound | Identify concurrent DVT; non-compressibility of proximal veins = DVT |
| Echo | Not a primary diagnostic tool but useful to exclude mimics (tamponade, aortic dissection, MI) and assess RV function |
Step 6: Differential Diagnosis
Given pleuritic chest pain, keep these alternatives in mind:
- Pneumonia / pleuritis
- Pericarditis
- Pleurisy (viral, costochondritis, musculoskeletal)
- Pneumothorax
- Rib fracture
- Acute coronary syndrome
- Aortic dissection
(Harrison's Table 290-3)
Step 7: If PE is Confirmed - Risk Stratification and Treatment
Risk categories:
- High-risk (massive): Hemodynamic instability (hypotension, shock) - consider systemic thrombolysis, catheter-directed therapy, or surgical embolectomy
- Intermediate-risk (submassive): Normotensive but RV dysfunction or elevated troponin - anticoagulation +/- escalation based on clinical trajectory
- Low-risk: Normal vitals, no RV dysfunction - anticoagulate, consider early discharge/outpatient treatment
Anticoagulation options:
- DOACs (rivaroxaban, apixaban) - first-line for most patients with confirmed PE
- LMWH - effective and preferred in cancer patients
- UFH - preferred when rapid reversal may be needed or if thrombolysis is planned
- Vitamin K antagonists (warfarin) - still used, bridged with heparin
"When acute PE is suspected, if the bleeding risk is deemed acceptable, anticoagulation should be initiated because this is the one approach that has proven to reduce mortality." (Fuster and Hurst's The Heart, 15th Ed., p. 1763)
Key Point for This Patient's Age
At 65, also evaluate for underlying malignancy as a provoking factor (unprovoked PE in older patients warrants age-appropriate cancer screening). Consider duration of anticoagulation carefully - extended therapy may be needed for unprovoked PE.
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 290
- Fuster and Hurst's The Heart, 15th Ed., Chapter 58
- Goldman-Cecil Medicine, Chapter 68
This is a shared conversation. Sign in to Orris to start your own chat.