Tabulate side effects of phenytoin, phenobarbitone,carbamazipine,Na valproate,midozolam
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the complete table.
Side Effects of Major Antiepileptic Drugs
Here is a comprehensive tabulation drawn from Harrison's Principles of Internal Medicine (22nd Ed.), Kaplan & Sadock's Synopsis of Psychiatry, Adams & Victor's Neurology, and Goldman-Cecil Medicine.
Overview Table
| System / Effect | Phenytoin | Phenobarbitone | Carbamazepine | Sodium Valproate | Midazolam |
|---|---|---|---|---|---|
| CNS - Dose-related | Nystagmus, ataxia, slurred speech, diplopia, dizziness, mental confusion, motor twitching | Sedation (adults), hyperactivity (children), cognitive impairment, lethargy | Ataxia, drowsiness, diplopia/blurred vision, dizziness, task-performance impairment | Tremor, sedation, ataxia | Sedation, psychomotor impairment, amnesia, dizziness |
| CNS - Behavioural | Insomnia, transient nervousness, headache | Irritability, mood changes, behavioural disturbance | -- | -- | Paradoxical agitation/delirium (especially elderly) |
| CNS - Movement disorder | Dyskinesias (rare, phenothiazine-like) | -- | -- | -- | -- |
| Respiratory | Cardiovascular/respiratory depression at toxic IV doses | Respiratory depression (overdose) | -- | -- | Dose-related respiratory depression and apnea (especially with opioids); synergistic with co-administered CNS depressants |
| Cardiovascular | Hypotension, cardiac dysrhythmias (especially IV), contraindicated in 2nd/3rd degree AV block | -- | Decreased cardiac conduction; caution in cardiac disease; rare: immune myocarditis | -- | Mild hypotension (alone); significant hypotension with opioids |
| GI | Nausea, vomiting (less common) | -- | Nausea, vomiting, gastric distress, constipation, diarrhea, anorexia | GI upset (less with delayed-release formulation), nausea, vomiting | Nausea, vomiting (less common) |
| Haematological | Thrombocytopenia, leukopenia, agranulocytosis, pancytopenia, aplastic anaemia (rare) | Megaloblastic anaemia (long-term, folate-related) | Leukopenia (1-2%), aplastic anaemia, agranulocytosis (1:125,000); monitor CBC at 3, 6, 9, 12 months | Bone marrow suppression (reversible, rare) | -- |
| Hepatic | Elevated alkaline phosphatase, GGT | Enzyme induction (hepatic cytochrome P450) | Hepatitis (transaminase elevation), cholestasis (elevated bilirubin/ALP); fatal hepatic failure if reintroduced | Fatal hepatotoxicity (idiosyncratic; highest risk children <2 yrs); avoid in pre-existing liver disease | Prolonged half-life with CYP3A4 inhibitors (azole antifungals, HIV protease inhibitors, CCBs) |
| Skin | Maculopapular rash, Stevens-Johnson syndrome (rare) | Morbilliform rash | Maculopapular rash (10-15% within 3 weeks), Stevens-Johnson syndrome, toxic epidermal necrolysis, exfoliative dermatitis | Rash (lower risk than CBZ after 2 months) | -- |
| Metabolic / Endocrine | Hyperglycemia; elevated serum glucose (diabetes); decreased thyroxine | Osteoporosis (CYP P450 induction → ↓ vitamin D) | Hyponatremia, SIADH-like picture (water intoxication); no significant weight gain | Weight gain, hyperandrogenism, menstrual irregularities, polycystic ovary-like syndrome | -- |
| Cosmetic (long-term) | Gingival hyperplasia, hirsutism, coarsening of facial features, gynecomastia | -- | -- | Alopecia (hair loss), weight gain | -- |
| Bone | Osteoporosis (CYP induction → ↓ vitamin D) | Osteoporosis | Osteoporosis | Elevated cholesterol (lesser effect) | -- |
| Renal / Electrolyte | -- | -- | Hyponatremia, water intoxication (esp. elderly); also has antidiuretic effect (occasionally used for diabetes insipidus) | -- | -- |
| Psychiatric | -- | Depression, cognitive slowing | -- | -- | Delirium in elderly; paradoxical excitation |
| Lymphatic | Lymphadenopathy, pseudolymphoma, Hodgkin's disease (rare, long-term) | -- | -- | -- | -- |
| Teratogenicity | Congenital malformations ("fetal hydantoin syndrome"); neonatal bleeding (↓ vitamin K-dependent factors) | -- | Cleft palate, fingernail hypoplasia, microcephaly, spina bifida | Neural tube defects; highest rate of adverse fetal outcome (~20%); teratogenic | Potential fetal harm with prolonged exposure |
| Dependence / Tolerance | -- | Physical dependence; tolerance; withdrawal seizures on abrupt cessation | -- | -- | Tolerance with chronic use; psychological and physical dependence |
| Drug interactions | Levels raised by: amiodarone, cimetidine, fluoxetine, INH, estrogens. Levels lowered by: carbamazepine, chronic alcohol | Induces CYP enzymes; accelerates metabolism of many drugs | Auto-induction of own metabolism; inhibits lamotrigine; interacts with lithium | Inhibits lamotrigine metabolism (doubles lamotrigine half-life); valproate levels affected by carbamazepine | CYP3A4 substrate; prolonged by azole antifungals, HIV protease inhibitors, CCBs |
Key "Must-Know" Side Effects by Drug
| Drug | Most Distinctive / Exam-Important Side Effects |
|---|---|
| Phenytoin | Gingival hyperplasia, hirsutism, nystagmus/ataxia (dose-toxic), lymphadenopathy, teratogenicity, nonlinear (zero-order) kinetics - small dose increments cause large toxicity |
| Phenobarbitone | Sedation (adults) / hyperactivity (children), cognitive impairment, tolerance and dependence, enzyme induction, osteoporosis, megaloblastic anaemia |
| Carbamazepine | Aplastic anaemia/agranulocytosis, Stevens-Johnson syndrome, hepatitis, hyponatremia (SIADH), diplopia/ataxia, teratogenicity (spina bifida) |
| Sodium Valproate | Hepatotoxicity (fatal in children <2 yrs), neural tube defects (highest teratogenic risk), weight gain, alopecia, tremor, pancreatitis (rare), bone marrow suppression |
| Midazolam | Respiratory depression (potentiated by opioids), apnea, amnesia, paradoxical agitation in elderly, delirium, prolonged effect with CYP3A4 inhibitors; reversible with flumazenil |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed., Table 436-9 (Antiepileptic Drug Adverse Effects)
- Kaplan & Sadock's Synopsis of Psychiatry, pp. 2001-2024 (Carbamazepine, Phenytoin sections)
- Adams & Victor's Principles of Neurology, 12th Ed., Chapter 15 (Specific Drugs in Seizure Treatment)
- Goldman-Cecil Medicine, MIDAZOLAM section
- Barash, Cullen & Stoelting's Clinical Anesthesia, 9th Ed., Benzodiazepines chapter
Clinical Note: Sodium valproate carries the highest teratogenic risk among all five drugs and should be avoided in women of childbearing age whenever possible. Midazolam is the only drug in this list that is reversible with a specific antagonist (flumazenil).
Each stage of lesion on facial nerve pathway and presentation
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive, detailed information from multiple authoritative sources. Let me compile the full answer.
Facial Nerve (CN VII) Pathway - Lesion Localization and Clinical Presentations
The Facial Nerve Pathway - Overview of Segments
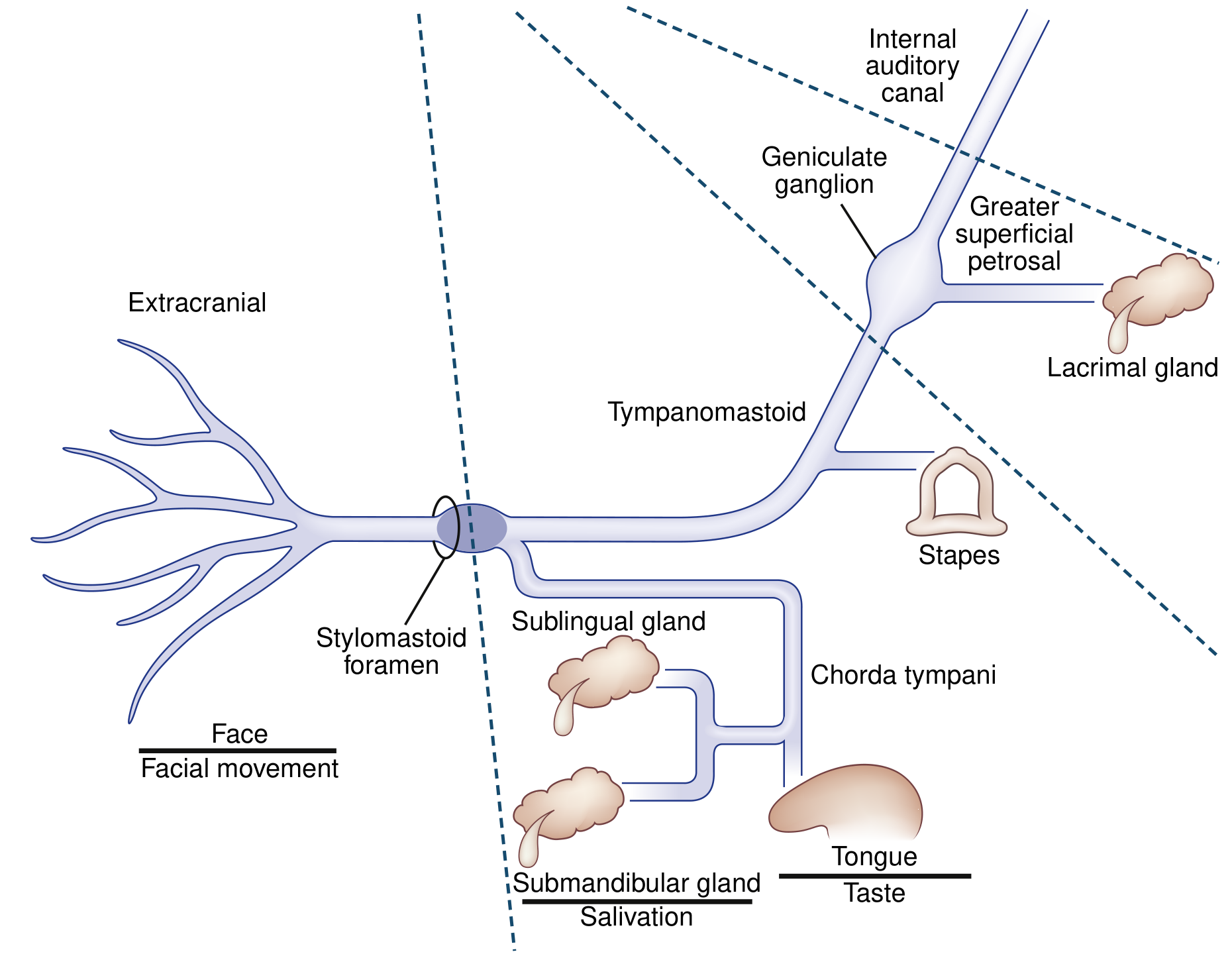
The facial nerve has 6 anatomical segments. Before tabulating lesions, understand the key branches given off along the intratemporal course - each one is the "marker" for lesion localization:
| Segment | Location | Length | Key Branch Given Off |
|---|---|---|---|
| 1. Intracranial | Brainstem (pons) to IAC | 17-24 mm | - |
| 2. Meatal | IAC fundus to meatal foramen | 8-10 mm | - |
| 3. Labyrinthine | Meatal foramen to geniculate ganglion | 4 mm (narrowest - most vulnerable) | Greater superficial petrosal nerve (GSPN) |
| 4. Tympanic | Geniculate ganglion to 2nd genu | 11 mm | Nerve to stapedius |
| 5. Mastoid/Vertical | 2nd genu to stylomastoid foramen | 13 mm | Chorda tympani |
| 6. Extratemporal | Stylomastoid foramen → parotid → 5 terminal branches | - | Temporal, zygomatic, buccal, marginal mandibular, cervical |
Stage-by-Stage Lesion Localization Table
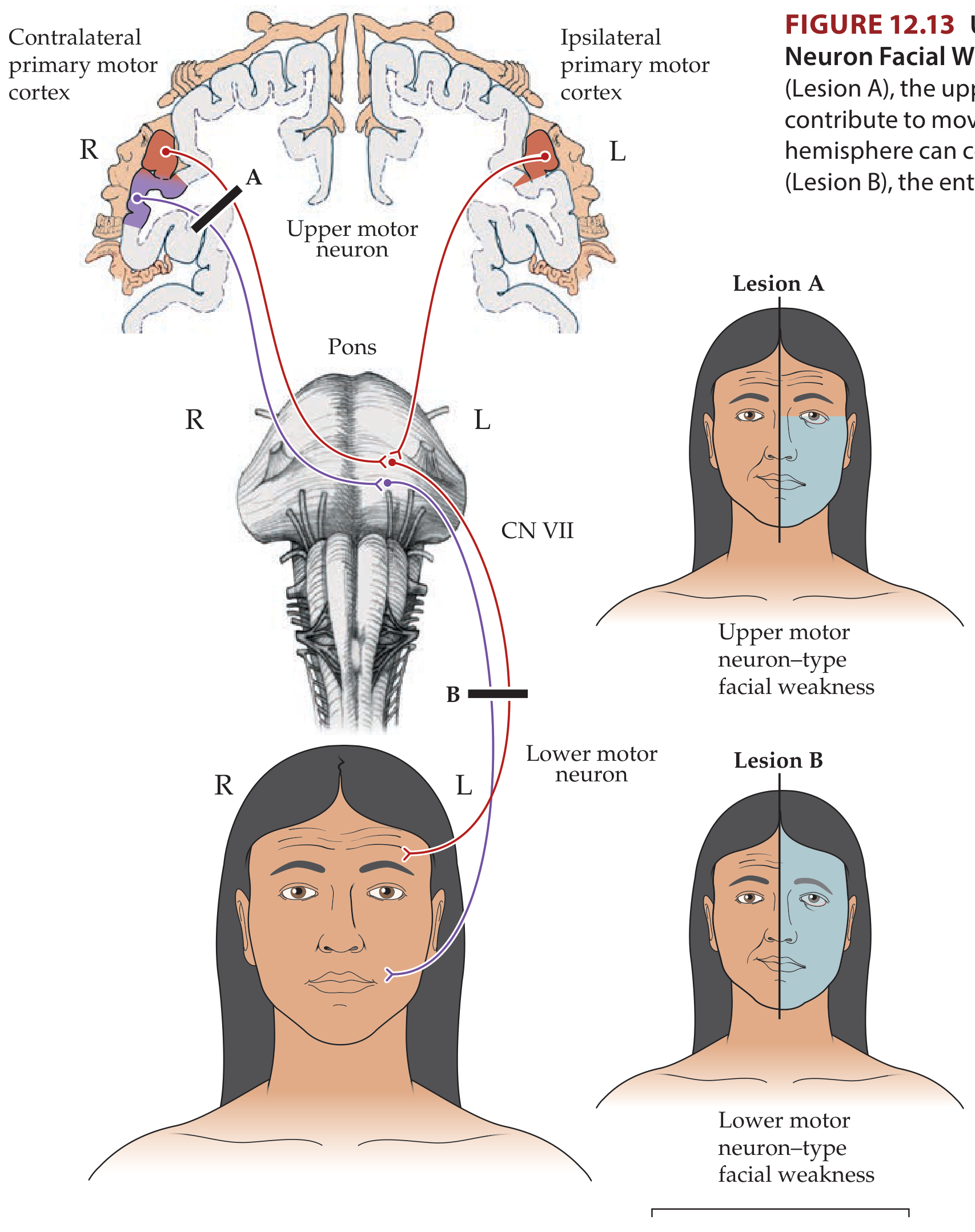
Stage 1: Supranuclear (Upper Motor Neuron) Lesion
Site: Cortex (motor cortex face area) → corticobulbar fibers → before reaching the facial nucleus in the pons
| Feature | Finding |
|---|---|
| Side of weakness | Contralateral lower face |
| Forehead | SPARED (receives bilateral cortical input) |
| Orbicularis oculi | Mildly weak (slightly widened palpebral fissure, slight difficulty burying eyelash on forced closure) |
| Lower face | Weak: flattened nasolabial fold, asymmetric smile, drooped angle of mouth |
| Emotional vs volitional | Dissociation possible - emotional movements (spontaneous smile) may be relatively preserved with impaired volitional movement (or vice versa, depending on cortical vs subcortical level) |
| Taste | Normal |
| Lacrimation | Normal |
| Salivation | Normal |
| Hyperacusis | Absent |
| Accompanying signs | Contralateral hemiparesis, hand/arm weakness, sensory loss, aphasia, or dysarthria (depending on lesion site) |
| Causes | MCA stroke, brain tumor, subdural hematoma, demyelination |
Key rule: UMN lesion = contralateral lower face only; forehead spared.
Stage 2: Facial Nucleus (Pons) Lesion
Site: Facial motor nucleus in lateral tegmentum of caudal pons
| Feature | Finding |
|---|---|
| Side of weakness | Ipsilateral entire face (upper + lower) |
| Forehead | NOT spared - involved |
| Type | LMN pattern |
| Taste, lacrimation, salivation | Typically spared (nucleus itself, not branches) |
| Key distinguishing feature | Neighboring pontine structures affected: abducens nucleus (CN VI) involvement → ipsilateral horizontal gaze palsy |
| Classic syndromes | Foville syndrome: ipsilateral CN VI + CN VII palsy + contralateral hemiparesis + corticospinal tract involvement |
| Millard-Gubler syndrome: ipsilateral CN VI + CN VII palsy + contralateral hemiparesis | |
| Other features | Facial myokymia (continuous muscle twitching) - seen with demyelination and brainstem gliomas |
| Causes | Pontine stroke, MS plaque, glioma, cavernous hemangioma |
Stage 3: Fascicular Segment (Brainstem Fascicle)
Site: Fibers looping around the abducens nucleus (forming the facial colliculus) before exiting the lateral pons
| Feature | Finding |
|---|---|
| Pattern | Similar to nuclear lesion - ipsilateral LMN complete facial palsy |
| Key anatomical feature | Fibers wrap around the abducens nucleus as the genu of the facial nerve (forms the facial colliculus visible in the floor of the 4th ventricle) |
| CN VI involvement | Often co-affected (abducens nucleus in the genu) |
| Causes | Brainstem ischemia, hemorrhage, demyelination, neoplasm |
Stage 4: Cerebellopontine Angle (CPA) / Subarachnoid Space
Site: From exit at lateral pons, through CPA, to entry into the internal auditory canal
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy (all of face) |
| Hearing | Sensorineural hearing loss (CN VIII travels alongside in CPA) |
| Taste | May be affected (nervus intermedius travels here) |
| Lacrimation | May be reduced |
| Hemifacial spasm | Compression of nerve root at brainstem exit by aberrant vascular loop → episodic involuntary facial contractions (NOT weakness); "other Babinski sign" (frontalis contraction with eye closure) |
| Causes | Acoustic neuroma (vestibulocochlear schwannoma), facial schwannoma (earlier facial weakness, "labyrinthine tail" on MRI), meningioma; infectious/inflammatory/neoplastic meningitis |
Stage 5: Internal Auditory Canal (IAC) / Meatal Segment
Site: Within the IAC, before reaching the geniculate ganglion; meatal foramen is the narrowest segment - most susceptible to compression/inflammation
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy |
| Hearing | Sensorineural hearing loss (CN VIII in IAC) |
| Lacrimation | Reduced (GSPN not yet given off, but coming up) |
| Causes | Bell's palsy (MRI enhancement typically at geniculate ganglion/meatal foramen), trauma, schwannoma |
Stage 6: Geniculate Ganglion / Labyrinthine Segment
Site: Geniculate ganglion; first intratemporal branch (GSPN) given off here
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy - entire face |
| Lacrimation | Reduced/absent (GSPN to lacrimal gland is disrupted) - increases risk of corneal damage |
| Hyperacusis | Present (stapedius nerve not yet given off, so intact - wait for below) |
| Taste (anterior 2/3 tongue) | Lost (chorda tympani not yet given off - remains intact here but taste is ultimately affected) |
| Salivation | Reduced (submandibular/sublingual glands) |
| Classic presentation | Ramsay Hunt Syndrome (herpes zoster reactivation at geniculate ganglion): facial palsy + auricular vesicles (Ramsay Hunt triad) + sensorineural hearing loss + vertigo; Bell's palsy (HSV reactivation): MRI enhancement most commonly at geniculate ganglion |
Stage 7: Tympanic Segment (Between GSPN and Nerve to Stapedius)
Site: Proximal to nerve to stapedius branch
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy |
| Lacrimation | Reduced (GSPN already given off - now disrupted) |
| Hyperacusis | Present (nerve to stapedius not yet given off, so stapedius is paralyzed) - sounds are perceived as abnormally loud |
| Taste | Lost |
| Salivation | Reduced |
| Causes | Temporal bone fracture, cholesteatoma, otitis media |
Stage 8: Mastoid Segment (Between Nerve to Stapedius and Chorda Tympani)
Site: Proximal to chorda tympani branch
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy |
| Lacrimation | Normal (GSPN already given off and now proximal - intact) |
| Hyperacusis | Present (stapedius paralyzed - nerve to stapedius is given off proximal to this) |
| Taste | Lost (chorda tympani not yet given off) |
| Salivation | Reduced |
| Causes | Mastoiditis, surgery, trauma |
Stage 9: At/Below Chorda Tympani (to Stylomastoid Foramen)
Site: Distal to chorda tympani branch, proximal to stylomastoid foramen
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy |
| Lacrimation | Normal |
| Hyperacusis | None (nerve to stapedius was given off proximally - above this) |
| Taste | Normal (chorda tympani preserved distal branching already occurred) |
| Salivation | Normal |
| Causes | Deep parotid surgery, mastoid surgery |
Stage 10: At Stylomastoid Foramen / Extratemporal
Site: At or just beyond the stylomastoid foramen; nerve enters parotid before branching
| Feature | Finding |
|---|---|
| Facial weakness | Ipsilateral complete LMN palsy (all 5 terminal branches) |
| Lacrimation | Normal |
| Taste | Normal |
| Hyperacusis | Absent |
| Salivation | Normal |
| Causes | Parotid gland tumors, parotid surgery, penetrating trauma, forceps delivery in neonates |
Stage 11: Distal/Terminal Branches (Post-Parotid)
Site: After division into temporal, zygomatic, buccal, marginal mandibular, cervical branches
| Feature | Finding |
|---|---|
| Weakness pattern | Partial - only muscles supplied by the affected branch(es) |
| Upper face only | Temporal/zygomatic branch damage: brow droop, inability to close eye |
| Lower face only | Marginal mandibular branch damage: drooped mouth corner, weak lower lip |
| Taste/lacrimation/hyperacusis | All normal |
| Causes | Parotidectomy, facial trauma, skin/soft tissue malignancy |
Summary Table for Quick Localization
| Level | Facial Weakness | Forehead | Lacrimation | Hyperacusis | Taste | Other Clues |
|---|---|---|---|---|---|---|
| Cortex (UMN) | Contralateral lower face | Spared | Normal | Normal | Normal | Hemiparesis, aphasia |
| Facial nucleus (pons) | Ipsilateral all face | Involved | Normal | Normal | Normal | CN VI palsy, gaze palsy (Foville/Millard-Gubler) |
| CPA/subarachnoid | Ipsilateral all face | Involved | ± Reduced | Normal/↑ | ± Lost | SNHL, CN VIII signs, hemifacial spasm |
| Geniculate ganglion | Ipsilateral all face | Involved | Reduced | Present | Lost | Ramsay Hunt (auricular vesicles + SNHL), Bell's palsy |
| Between GSPN & stapedius nerve | Ipsilateral all face | Involved | Reduced | Present | Lost | - |
| Between stapedius & chorda tympani | Ipsilateral all face | Involved | Normal | Present | Lost | Mastoid/middle ear disease |
| Below chorda tympani → stylomastoid | Ipsilateral all face | Involved | Normal | None | Normal | - |
| Extratemporal / parotid | Ipsilateral all face | Involved | Normal | None | Normal | Parotid mass, surgery |
| Terminal branches | Partial facial weakness | Partly | Normal | None | Normal | Trauma, tumor, surgery |
Key principles to remember:
- Forehead spared = UMN (supranuclear) because the upper face motor neurons receive bilateral cortical input
- Forehead involved = LMN (nucleus, fascicle, or peripheral nerve)
- The lower you go in the intratemporal course, the fewer additional features (lacrimation, hyperacusis, taste are progressively "lost" from the deficits as branches are given off)
- Lacrimation lost = lesion at or proximal to geniculate ganglion (GSPN)
- Hyperacusis = lesion proximal to (above) the nerve to stapedius but distal to GSPN
- Taste lost alone (without lacrimal or hyperacusis) = lesion between nerve to stapedius and stylomastoid foramen (chorda tympani involved)
Sources: Neuroanatomy through Clinical Cases, 3rd Ed. (KCC 12.3); Bradley & Daroff's Neurology in Clinical Practice, 8th Ed. (Chapter 104); KJ Lee's Essential Otolaryngology, 11th Ed. (Chapter 21)
This is a shared conversation. Sign in to Orris to start your own chat.