Write me a general surgery resident level essay on Haemorrhoids including upto management
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Searching PubMed
hemorrhoids management systematic review
I now have all the content I need from Schwartz's Principles of Surgery and Bailey & Love's, plus excellent surgical illustrations. Let me compose the comprehensive resident-level essay.
Haemorrhoids: A Comprehensive Essay for the General Surgery Resident
1. Definition and Historical Perspective
Haemorrhoids (from Greek: haima = blood, rhos = flowing; synonym: piles, from Latin pila = a ball) are symptomatic enlargements or prolapse of the normal anal cushions. It is important to appreciate at the outset that haemorrhoids are not simply dilated veins but rather vascular cushions - submucosal structures containing venules, arterioles, arteriovenous communications, and smooth muscle fibres (the muscularis submucosae ani) - that are an anatomically normal component of the anal canal. Treatment is therefore only indicated when these structures become symptomatic. - Schwartz's Principles of Surgery, 11th Ed.
The condition has been recognised since antiquity. Descriptions appear in the Ebers Papyrus (~1550 BC) and the works of Hippocrates. The modern operative approaches were systematised by Milligan and Morgan (1937) and Parks/Ferguson (1959), whose techniques remain the gold standard today.
2. Surgical Anatomy
2.1 The Anal Canal
The anal canal extends from the anorectal junction to the anal verge, measuring approximately 3-4 cm. The dentate line (pectinate line) lies at its midpoint and is the embryological boundary between the endodermal hindgut above and the ectodermal proctodeum below. This boundary has major clinical implications:
| Feature | Above Dentate Line | Below Dentate Line |
|---|---|---|
| Epithelium | Columnar/transitional mucosa | Squamous anoderm |
| Innervation | Autonomic (insensate) | Somatic (richly innervated) |
| Lymphatics | Internal iliac nodes | Inguinal nodes |
| Venous drainage | Portal (via superior rectal) | Systemic (via inferior rectal) |
2.2 Anal Cushions
Three primary anal cushions are located at the left lateral, right anterior, and right posterior positions (3, 7, and 11 o'clock in the lithotomy position). Secondary haemorrhoids may develop between these primary positions. The cushions are composed of:
- The internal haemorrhoidal venous plexus (submucosal)
- Terminal branches of the superior, middle, and inferior rectal arteries
- Smooth muscle fibres (muscularis submucosae ani) and elastic connective tissue
- Arteriovenous communications that explain the characteristic bright-red, arterialised nature of haemorrhoidal bleeding
The internal plexus communicates with the external haemorrhoidal plexus (which lies below the dentate line, within and deep to the anoderm) via perforating vessels through the internal sphincter. The cushions function as part of the continence mechanism, contributing up to 15-20% of resting anal pressure, and ensure complete sealing of the anal canal at rest. - Bailey and Love's Short Practice of Surgery, 28th Ed.
3. Pathophysiology
The exact aetiology of symptomatic haemorrhoids remains debated. Three main theories exist:
3.1 Vascular Engorgement Theory (traditional): Increased intra-abdominal or intravascular pressure engorges the haemorrhoidal plexus. Contributory factors include:
- Constipation with prolonged straining
- Pregnancy (direct compression by the gravid uterus plus progesterone-induced venous relaxation)
- Prolonged sitting on the toilet
- Low-fibre diet producing hard, bulky stools
- Portal hypertension (though haemorrhoids are not more common in cirrhosis - rectal varices are a distinct entity)
3.2 Mucosal Sliding / Anal Cushion Prolapse Theory (Parks, 1956 - now accepted as central): Fragmentation and degradation of the supportive connective tissue (Treitz's muscle, Parks's ligament) anchoring the cushions to the internal sphincter leads to downward displacement. Once prolapsed, impaired venous drainage creates progressive engorgement, oedema, and local stasis. Shearing forces during defecation cause mucosal trauma and bleeding.
3.3 Hyperperfusion Theory: Studies using Doppler have shown increased arterial inflow to the haemorrhoidal plexus in symptomatic patients, which forms the rationale for Doppler-guided haemorrhoidal artery ligation (DGHAL/THD).
The consequence of these processes is the triad of bleeding, prolapse, and pruritus - the cardinal symptoms of haemorrhoidal disease. - Schwartz's Principles of Surgery, 11th Ed.
4. Classification
4.1 By Location Relative to the Dentate Line
Internal haemorrhoids are located proximal to the dentate line and covered by insensate anorectal mucosa. They may bleed or prolapse but rarely cause pain unless strangulated.
External haemorrhoids are located distal to the dentate line and covered by richly innervated anoderm. Thrombosis causes significant pain. Residual fibrotic skin tags are common sequelae.
Mixed (combined) haemorrhoids straddle the dentate line and exhibit features of both. These are common in long-standing disease.
4.2 Grading of Internal Haemorrhoids (Goligher Classification)
This is the most widely used clinical grading system and directly guides management:
| Grade | Description |
|---|---|
| I | Bulge into the anal canal; may prolapse beyond the dentate line on straining; do not prolapse out of the anus; bleed |
| II | Prolapse through the anus on straining; reduce spontaneously |
| III | Prolapse through the anus and require manual reduction |
| IV | Permanently prolapsed; cannot be reduced; risk of strangulation |
A practical aide-memoire: "Bulge - Spontaneous - Manual - Permanent"
5. Clinical Features
5.1 Symptoms
Bleeding is the earliest and most common symptom. It is characteristically:
- Bright red (arterialised blood)
- Painless
- Separate from the stool - seen on the paper on wiping, as a splash in the pan, or dripping after defecation
- Rarely sufficient alone to cause anaemia, though chronic occult loss can do so in neglected cases
Prolapse - patients describe lumps at the anal orifice during defecation (Grade II-IV).
Pruritus ani - caused by mucus discharge from the prolapsed mucosa irritating the perianal skin and impairing hygiene.
Mucus discharge - common with prolapsing haemorrhoids.
Pain is not a typical symptom of uncomplicated internal haemorrhoids (they are insensate above the dentate line). The presence of pain should prompt consideration of:
- Thrombosed external haemorrhoid
- Anal fissure
- Perianal abscess
- Anal carcinoma
Thrombosed external haemorrhoid (perianal haematoma): Presents as sudden onset, severe, well-localised perianal pain with a tense, olive-shaped, bluish subcutaneous swelling at the anal margin, typically following a precipitating event (straining at stool, heavy lifting, coughing). - Bailey and Love's Short Practice of Surgery, 28th Ed.

Figure 1: Thrombosed external haemorrhoid that has spontaneously ruptured. Note the extruded clot and separate mucosal prolapse. (Source: Bailey and Love's, 28th Ed.)
5.2 Strangulated Haemorrhoids
A surgical emergency. Grade IV or acutely irreducible Grade III haemorrhoids may become strangulated when the anal sphincter contracts around prolapsed tissue, occluding venous return. This leads to:
- Oedema and engorgement of all three haemorrhoidal cushions
- Thrombosis
- Necrosis and potential sepsis if untreated
6. Diagnosis
Haemorrhoids are a clinical diagnosis, supported by examination findings:
History: Note the character of bleeding (bright red, separate from stool), prolapse, bowel habits, diet, and associated symptoms (change in bowel habit, weight loss, tenesmus - which raise the suspicion of colorectal malignancy).
Examination:
- Perianal inspection: Skin tags, external haemorrhoids, prolapse at rest or on Valsalva
- Digital rectal examination (DRE): Internal haemorrhoids are typically not palpable unless thrombosed. DRE is essential to exclude anorectal malignancy, prostatic pathology, and assess sphincter tone
- Proctoscopy/rigid sigmoidoscopy: Required to directly visualise and grade internal haemorrhoids
Important: Any patient over 40, or any patient with an atypical history, a change in bowel habit, or a family history of colorectal cancer must undergo colonoscopy or flexible sigmoidoscopy to exclude a proximal colorectal neoplasm before attributing rectal bleeding to haemorrhoids. Haemorrhoids do not cause a change in bowel habit.
7. Management
Management is graded to the severity of symptoms and the haemorrhoidal grade. The management ladder ascends from conservative measures through office-based procedures to surgical intervention.
7.1 Conservative (Non-Operative) Management
Indications: First-line for Grade I, II, and mild Grade III. Aims to reduce straining and engorgement.
- Dietary modification and hydration: High-fibre diet (25-30 g/day), adequate hydration (1.5-2 L/day) to produce soft, formed stools. This is the single most important and most often neglected intervention.
- Fibre supplementation: Psyllium husk, ispaghula husk
- Stool softeners/laxatives: Lactulose, macrogol (PEG) preparations
- Avoid prolonged sitting on the toilet
- Sitz baths: Warm water soaks for symptomatic relief, especially post-procedure or for thrombosed haemorrhoids
- Topical preparations: Anaesthetic and steroid-containing creams (e.g. Anusol-HC, Proctosedyl) provide symptomatic relief but do not treat the underlying condition and should not be used long-term
- Flavonoids (micronised purified flavonoid fraction - MPFF, e.g. Daflon): A recent meta-analysis (PMID: 38847122) demonstrated that flavonoids improve post-haemorrhoidectomy recovery, reduce bleeding, and reduce pain. They act by improving venous tone, reducing capillary permeability, and enhancing lymphatic drainage. They have a role both in conservative management and as adjuncts peri-operatively.
7.2 Office-Based (Outpatient) Procedures
Indications: Grade I, II, and selected Grade III haemorrhoids failing conservative treatment.
7.2.1 Rubber Band Ligation (RBL)
The most widely used and most effective office procedure. Best suited for Grade I, II, and selected Grade III bleeding internal haemorrhoids.
Technique: Mucosa located 1-2 cm proximal to the dentate line is grasped with an applicator and drawn into the barrel of a rubber band ligator. Firing the device deploys two small elastic bands that strangulate the tissue, causing ischaemic necrosis, scarring, and fixation of the cushion, preventing further prolapse or bleeding. Only 1-2 quadrants are banded per session. Multiple sessions 4-6 weeks apart may be required.
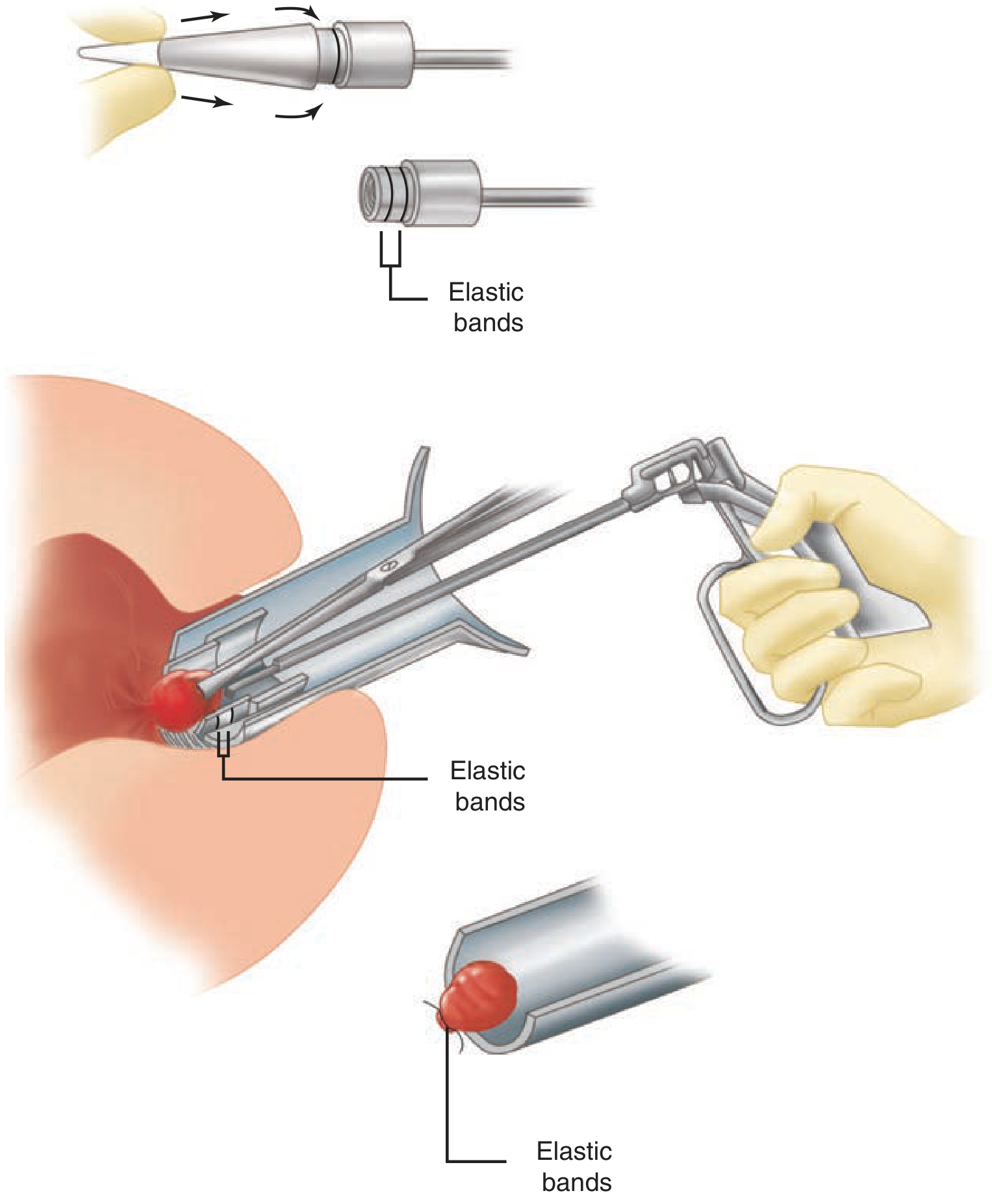
Figure 2: Rubber band ligation technique showing the banding applicator and deployment of elastic bands around the haemorrhoidal pedicle. (Source: Schwartz's Principles of Surgery, 11th Ed.)
Key safety point: The band must be placed at or above the dentate line. Placement below the dentate line results in intense pain due to the rich somatic innervation of the anoderm.
Complications:
- Pain/discomfort (~15%): from an excessively low or tight band
- Urinary retention (~1%): suggests inadvertent inclusion of internal sphincter fibres
- Delayed bleeding (7-10 days post-procedure): when the ligated pedicle necroses and sloughs; usually self-limited
- Necrotising infection (rare but life-threatening): presents with severe pain, fever, and urinary retention; requires urgent examination under anaesthesia, debridement, drainage, and broad-spectrum antibiotics
7.2.2 Sclerotherapy (Injection Sclerotherapy)
Sclerosant (typically 5% phenol in almond oil, sodium tetradecyl sulphate, or hypertonic saline) is injected into the submucosa above the haemorrhoidal base, inducing fibrosis, obliterating the feeding vessels, and fixing the mucosa to the underlying muscle.
Indications: Grade I, II, and some Grade III haemorrhoids, particularly when the patient is anticoagulated (safer than RBL).
Volume: 1-3 mL per haemorrhoid; all three quadrants may be treated at one visit.
Complications: Pain (if injected too deeply), mucosal ulceration, impotence (if injected anteriorly in males - injection into the prostatic plexus), and abscess formation.
7.2.3 Infrared Photocoagulation (IRC)
An infrared probe applied to the apex of each haemorrhoid coagulates the underlying venous plexus, causing fibrosis and fixation. All three quadrants can be treated at one visit.
Indications: Best for small Grade I and II haemorrhoids. Not effective for larger haemorrhoids or significant prolapse.
Advantages: Quick, well-tolerated, minimal complications.
Disadvantages: Higher recurrence rate than RBL; equipment cost.
7.2.4 Cryotherapy and Bipolar Diathermy
Less commonly used in modern practice; similar principles of local tissue destruction.
7.3 Operative (Surgical) Management
Indications for surgery:
- Grade III haemorrhoids failing office-based treatment
- Grade IV haemorrhoids
- Mixed internal/external haemorrhoids
- Patient preference after failed conservative/office treatment
- Acutely strangulated haemorrhoids (selected cases)
- Acutely thrombosed external haemorrhoids (within 72 hours)
- Portal hypertension: surgical haemorrhoidectomy should generally be avoided - rectal varices causing haemorrhage are better managed by reducing portal pressure
7.3.1 Excision of Thrombosed External Haemorrhoid
Timing: Within the first 24-72 hours of thrombosis, when pain is maximal and the clot is firm.
Technique: Office or emergency department procedure under local anaesthesia (1% lidocaine with adrenaline). An elliptical excision (not simple incision and drainage - the clot is typically loculated) is made over the thrombosis, the entire clot evacuated, and the wound left open to heal by secondary intention.
After 72 hours: The clot begins to resorb, pain spontaneously resolves, and conservative management with sitz baths and analgesics is preferred. Surgery at this stage offers no additional benefit.
7.3.2 Excisional Haemorrhoidectomy
The definitive treatment for Grade III-IV haemorrhoids and combined (mixed) haemorrhoids. All operative techniques share the same principles: decreasing blood supply to the haemorrhoidal plexuses and excising redundant anoderm and mucosa.
Positioning: Prone jack-knife position (most common) or lithotomy position. The prone position affords excellent perianal exposure and assistant access.
Anaesthesia: Local anaesthesia (LA) with IV sedation, spinal/epidural, or general anaesthesia (GA). LA use is increasing due to reduced urinary retention, faster recovery, and suitability for day-case surgery.
A. Open Haemorrhoidectomy (Milligan-Morgan, 1937)
The original and most widely used technique worldwide.
The three haemorrhoidal pedicles are identified. Each haemorrhoid is grasped and elevated. An artery forceps is placed across the base of the pedicle, the haemorrhoid excised distal to the forceps, the pedicle transfixed and ligated with an absorbable suture, and the wounds left open to heal by secondary intention. Skin bridges (mucosal bridges of 0.5-1 cm width between the excised quadrants) are preserved to avoid anal stenosis.
Advantages: Avoids wound infection; simple; excellent access for large haemorrhoids.
Disadvantages: Prolonged wound healing (4-6 weeks); post-operative pain.
B. Closed (Submucosal) Haemorrhoidectomy (Parks/Ferguson, 1959)
The Parks or Ferguson haemorrhoidectomy involves resection of haemorrhoidal tissue through a narrow elliptical incision starting just distal to the anal verge and extending proximally to the anorectal ring. Key steps:
- Identify the internal sphincter fibres and carefully dissect them away from the haemorrhoidal tissue (submucosal plane) to avoid sphincter injury
- Ligate the apex of the haemorrhoidal pedicle with a transfixion suture
- Excise the haemorrhoid
- Close the wound with a running absorbable suture
All three cushions may be removed. Careful preservation of adequate skin/mucosal bridges between the three excised quadrants is mandatory to prevent anal stenosis, the most dreaded long-term complication.
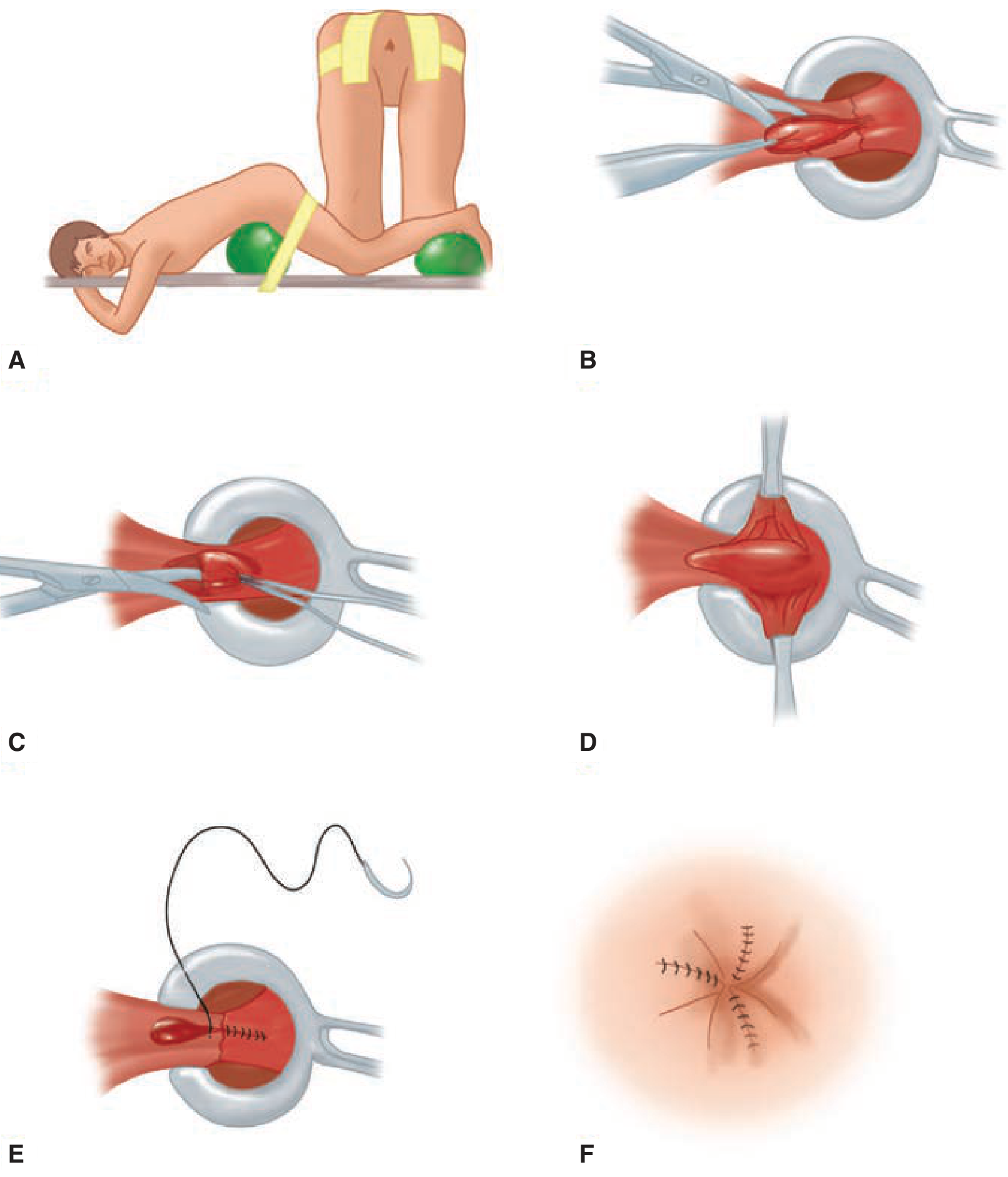
Figure 3: Closed submucosal haemorrhoidectomy (Ferguson technique). Steps A-F as described above. (Source: Schwartz's Principles of Surgery, 11th Ed.)
Advantages: Faster wound healing; reduced post-operative pain vs open technique.
Disadvantages: Risk of wound dehiscence/infection if wounds are too large or tension excessive.
C. Whitehead's Haemorrhoidectomy
Circumferential excision of all haemorrhoidal tissue just proximal to the dentate line, with circumferential advancement and suturing of the rectal mucosa to the dentate line. Largely of historical interest due to the feared Whitehead deformity - mucosal ectropion (the "wet anus") caused by pulling the mucosa too far down, leading to chronic mucus discharge, pruritus, and difficulty with hygiene. Some expert colorectal surgeons still use this technique in select cases.
7.3.3 Procedure for Prolapse and Haemorrhoids (PPH) / Stapled Haemorrhoidopexy
Introduced by Longo in 1998, PPH uses a circular stapling device (similar to an EEA stapler) to excise a doughnut of rectal mucosa and submucosa 3-4 cm proximal to the dentate line. The primary mechanism is:
- Pexying of the redundant prolapsed haemorrhoidal tissue back to its anatomical position
- Interruption of the feeding vessels (superior rectal arteries within the submucosa)
- Fixation of the mucosa proximally
The haemorrhoidal tissue itself is not excised but de-vascularised and repositioned.
Indications: Grade II-III internal haemorrhoids. Best evidence is for circumferential prolapse.
Advantages: Less post-operative pain (the staple line is above the dentate line, in insensate mucosa), shorter hospital stay, faster return to work.
Disadvantages and complications:
- Higher recurrence rate of haemorrhoidal prolapse compared to excisional haemorrhoidectomy (supported by systematic review evidence)
- Chronic anal pain (staple line below the dentate line, or incorporated sphincter fibres)
- Obstructing rectal stricture
- Rectovaginal fistula
- Rectal perforation (rare but catastrophic)
- Bacteraemia
Multiple systematic reviews and meta-analyses have shown PPH has equivalent complication rates to excisional haemorrhoidectomy in the short term but lower long-term durability.
7.3.4 Doppler-Guided Haemorrhoidal Artery Ligation (DGHAL) / Transanal Haemorrhoidal Dearterialization (THD)
A Doppler probe mounted on a purpose-built proctoscope identifies the 6-8 terminal branches of the superior rectal artery entering the haemorrhoidal plexus (typically at the 1, 3, 5, 7, 9, and 11 o'clock positions). These vessels are ligated with a transfixion suture under Doppler guidance. A mucopexy (plication suture to reposition prolapsed tissue) is typically added.
Rationale: Addresses the hyperperfusion mechanism.
Advantages: No excision of tissue, minimal pain, day-case, suitable for anticoagulated patients.
Disadvantages: Specialised equipment required; long-term durability data still accumulating; higher recurrence vs excisional haemorrhoidectomy for Grade IV disease. - Schwartz's Principles of Surgery, 11th Ed.
7.4 Special Situations
Pregnancy: Haemorrhoids are extremely common in pregnancy and the puerperium. The initial management is almost always conservative (fibre, hydration, sitz baths, topical preparations). Postpartum haemorrhoids resulting from straining during labour with significant thrombosis or prolapse may benefit from haemorrhoidectomy, especially in patients with pre-existing chronic haemorrhoidal symptoms. Office-based procedures should generally be deferred until after delivery.
Strangulated haemorrhoids: Can be managed either by emergency haemorrhoidectomy (within the first 24-48 hours, before oedema becomes prohibitive, by an experienced surgeon - associated with higher rates of bleeding and sepsis but definitive treatment) or conservatively with bed rest, ice packs, analgesia, and a stool softener followed by elective haemorrhoidectomy at 6-8 weeks when oedema has resolved. Both approaches are practised; the evidence does not clearly favour one over the other.
Portal hypertension / cirrhosis: Haemorrhoidal disease is not more common in patients with portal hypertension than in the general population. Rectal varices, however, are a distinct entity and may bleed in these patients. The primary treatment is reduction of portal pressure (TIPSS, beta-blockade). Surgical haemorrhoidectomy in this cohort carries very high risk and should generally be avoided. If suture ligation is absolutely necessary for massive persistent bleeding, it should be done with extreme caution.
Immunocompromised patients (e.g. HIV, haematological malignancy): Office procedures should be used with caution. Surgical haemorrhoidectomy carries significant risk of sepsis and impaired wound healing. Medical management is preferred wherever possible.
8. Complications of Haemorrhoidectomy
| Complication | Incidence | Notes |
|---|---|---|
| Post-operative pain | Nearly universal | NSAIDs, opioids, muscle relaxants, sitz baths, topical GTN/diltiazem (reduce sphincter spasm) |
| Urinary retention | 10-50% | Minimise IV fluids intra-operatively; adequate analgesia |
| Primary/reactionary haemorrhage | 1-2% | Identify bleeding vessel under GA; suture ligation |
| Secondary haemorrhage (7-10 days) | ~1% | Sloughing of pedicle; usually self-limiting |
| Faecal impaction | ~1-5% | Pre-operative bowel preparation, post-operative laxatives |
| Anal stenosis | <1% | Preserve adequate mucosal bridges; treat with dilation or anoplasty |
| Infection/abscess | Rare | Broad-spectrum antibiotics; drainage |
| Faecal incontinence | Rare (<1%) | Avoid sphincter injury; careful dissection |
| Fistula-in-ano | Rare |
9. Summary: Management Algorithm
HAEMORRHOIDS
|
+--- Grade I/II -------> Conservative (diet, fibre, hydration)
| |
| Fails? --> Office-based procedure
| (RBL preferred; or sclerotherapy/IRC)
|
+--- Grade III ---------> Conservative first, then:
| - Office-based (RBL x multiple sessions)
| - Failing: Excisional haemorrhoidectomy
| OR PPH (grade II-III)
| OR DGHAL/THD
|
+--- Grade IV ----------> Excisional haemorrhoidectomy
| (Milligan-Morgan or Ferguson)
|
+--- Thrombosed ext. ---> < 72 hrs: Elliptical excision under LA
| > 72 hrs: Conservative (sitz baths, analgesia)
|
+--- Strangulated ------> Emergency haemorrhoidectomy (early)
OR Conservative then elective
10. Differential Diagnosis
The following must be excluded before attributing perianal symptoms to haemorrhoids:
- Colorectal carcinoma (most important - always exclude with scoping)
- Anal fissure (bright red rectal bleeding with severe pain)
- Perianal / ischiorectal abscess
- Fistula-in-ano
- Rectal prolapse (full-thickness prolapse vs haemorrhoidal prolapse)
- Condylomata acuminata
- Pruritus ani from other causes
- Inflammatory bowel disease (particularly Crohn's perianal disease)
- Rectal varices (portal hypertension)
Key Points for the Surgeon
- Haemorrhoids are normal structures - treat only when symptomatic.
- Always exclude colorectal malignancy before labelling bleeding as haemorrhoidal, especially in patients over 40 or with change in bowel habit.
- The Goligher classification directly drives management decisions.
- Conservative management and dietary change are the cornerstone for Grade I-II disease.
- RBL is the most effective office-based procedure for Grade II-III internal haemorrhoids.
- Never band below the dentate line - this causes intense pain.
- In excisional haemorrhoidectomy, preserve adequate mucosal bridges to prevent anal stenosis.
- Identify and protect the internal sphincter at every step.
- PPH is associated with less short-term pain than excisional haemorrhoidectomy but higher recurrence rates.
- Suspect necrotising sepsis in any patient with escalating pain, fever, and urinary retention after RBL - examine under anaesthesia urgently.
Sources:
- Schwartz's Principles of Surgery, 11th Ed., Chapter 29
- Bailey and Love's Short Practice of Surgery, 28th Ed., Chapter 80
- Pitesa R et al. Flavonoids and post-haemorrhoidectomy recovery: a systematic review and meta-analysis. ANZ J Surg, 2024 Sep (PMID: 38847122)
This is a shared conversation. Sign in to Orris to start your own chat.