AIDS - etiology, routes of transmission, natural history (phases), diagnosis 2nd yr mbbs patho refer harsh mohan
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Searching Images
HIV AIDS natural history CD4 count viral load phases
Loading Image
I now have all the material needed for a comprehensive answer. Let me compose it.
AIDS — Etiology, Routes of Transmission, Natural History & Diagnosis
(Based on Robbins Cotran & Kumar: Pathologic Basis of Disease + Robbins & Kumar Basic Pathology)
1. Etiology
Causative agent: Human Immunodeficiency Virus (HIV), a retrovirus belonging to the family Retroviridae, subfamily Lentiviridae.
Two types exist:
- HIV-1 — responsible for the global pandemic; more virulent
- HIV-2 — largely confined to West Africa; less pathogenic
Structure of HIV-1
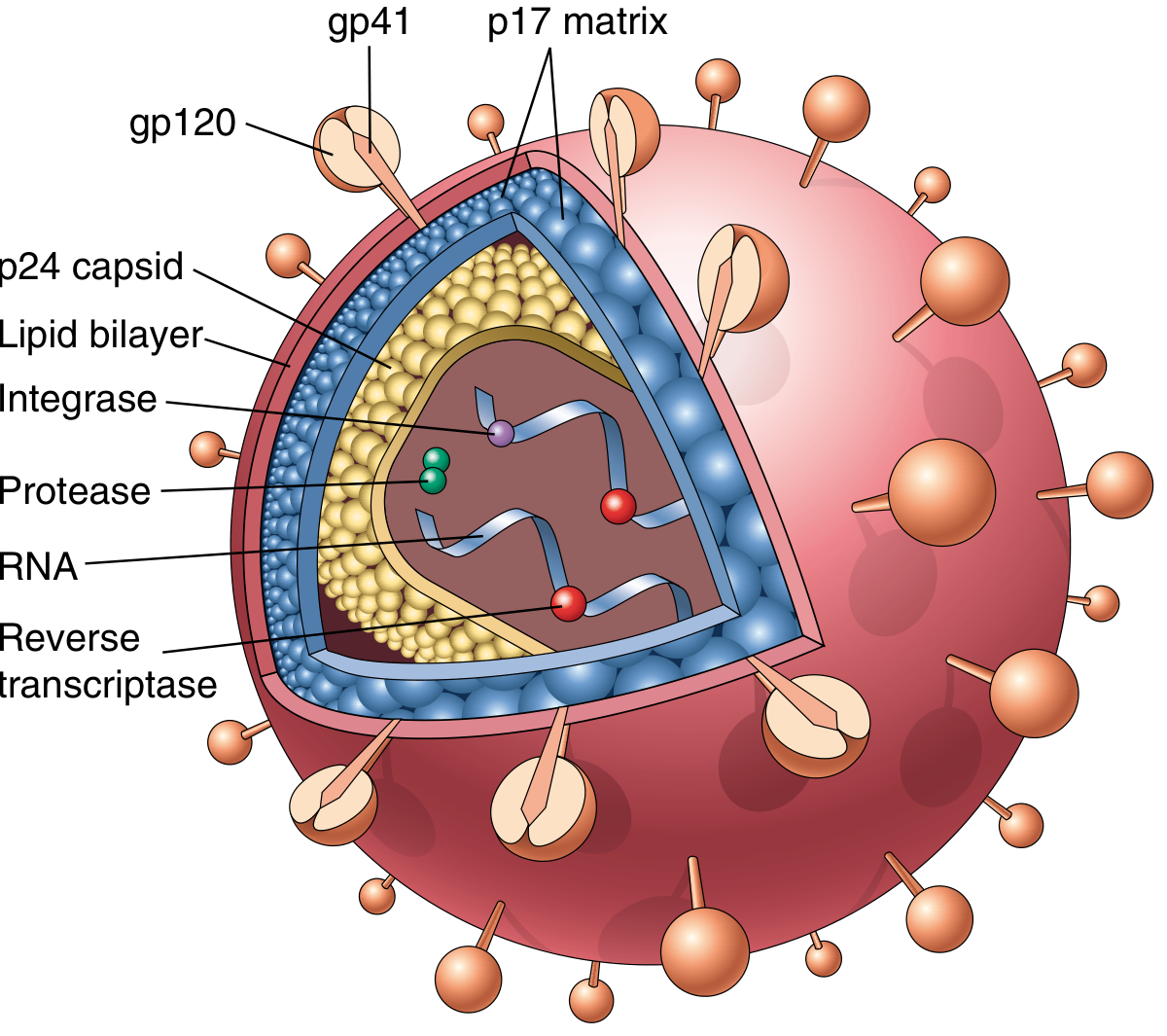
The HIV-1 virion is spherical with an electron-dense, cone-shaped core surrounded by a host cell–derived lipid envelope. Key components:
| Component | Function |
|---|---|
| gp120 (envelope glycoprotein) | Binds CD4 receptor on host cells |
| gp41 (transmembrane) | Mediates membrane fusion/viral entry |
| p17 (matrix protein) | Lines inner surface of envelope |
| p24 (capsid protein) | Most abundant antigen; detected by ELISA in diagnosis |
| Reverse transcriptase | Converts viral RNA → DNA |
| Integrase | Integrates proviral DNA into host genome |
| Protease | Cleaves precursor proteins into mature viral proteins |
| Two copies of ssRNA genome | Carries genetic information |
Genome
The RNA genome contains:
- Structural genes: gag (core proteins), pol (enzymes), env (envelope glycoproteins)
- Regulatory genes: tat (1000× increase in viral transcription — critical for replication), rev, vif, nef, vpr, vpu
- LTRs (Long Terminal Repeats) — regulate gene expression
— Robbins Cotran & Kumar: Pathologic Basis of Disease
2. Routes of Transmission
HIV is transmitted by three major routes:
A. Sexual Transmission
- Most common route worldwide — predominantly heterosexual transmission globally
- In the United States, men who have sex with men (MSM) account for >50% of reported cases (~70% of new cases)
- Heterosexual transmission accounts for ~20% of US cases
- Virus is present in semen and cervical/vaginal secretions
- Receptive anal intercourse carries the highest risk; mucosal disruption amplifies risk
B. Parenteral Transmission (Blood-borne)
- Intravenous drug users sharing contaminated needles — a major risk group
- Transfusion of infected blood or blood products (now rare in countries with blood screening)
- Needle-stick injuries in healthcare workers (risk ~0.3% per exposure)
- Sharing of contaminated needles, syringes
C. Vertical (Mother-to-Child) Transmission
- Transplacental spread during pregnancy
- Intrapartum — exposure to infected maternal blood/secretions during delivery
- Breastfeeding (postpartum)
- ART has dramatically reduced vertical transmission
Notable: HIV is not transmitted by casual contact, insect vectors, saliva, tears, or shared utensils.
— Robbins Cotran & Kumar: Pathologic Basis of Disease
3. Natural History — Phases of HIV Infection
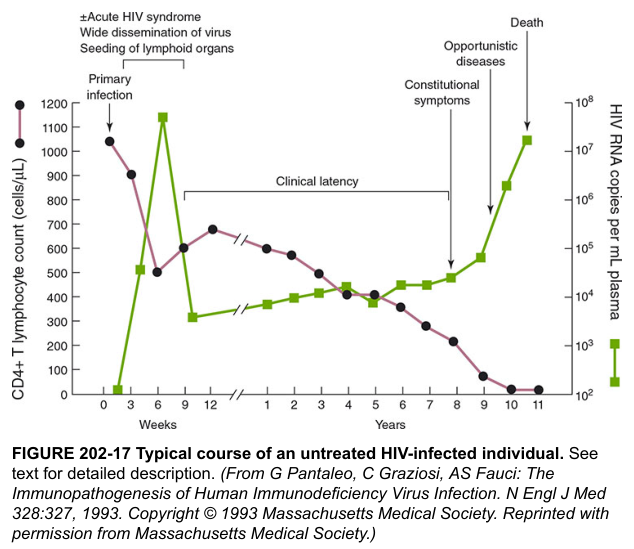
HIV infection progresses through three distinct phases:
Phase 1: Acute (Primary) HIV Infection
Timing: 3–6 weeks after initial exposure
Pathophysiology:
- Virus enters via mucosal surfaces; initially infects CD4+ T cells, dendritic cells (DCs), and macrophages
- Massive viral replication → viremia → widespread dissemination to lymphoid organs
- CD4+ T cell count drops sharply; then partially recovers as immune response mounts
- Viral load peaks then falls to a "viral set point" — this plateau level predicts future progression rate
Clinical features (acute retroviral syndrome):
- Flu-like/mononucleosis-like illness: fever, lymphadenopathy, pharyngitis, rash, myalgia, headache
- Self-limiting, lasting 2–4 weeks
- Window period: antibodies not yet detectable (hence ELISA may be negative for up to 3–4 weeks)
Phase 2: Chronic Infection (Clinical Latency Phase)
Duration: Typically 7–10 years (untreated)
Pathophysiology:
- Lymph nodes and spleen are sites of continuous HIV replication
- CD4+ T cells are progressively destroyed (HIV destroys up to 2 × 10⁹ CD4+ cells/day)
- CD4 count steadily declines; >90% of body's T cells reside in lymphoid organs
- Despite apparent clinical silence, viral replication is not truly "latent" — it is ongoing in lymphoid tissue
Viral set point & CD4 count:
- Only 8% of patients with viral load <4,350 copies/μL progressed to AIDS in 5 years vs. 62% of those with >36,270 copies
Clinical features:
- Patient often asymptomatic for years
- Minor opportunistic infections may appear: oral candidiasis (thrush), vaginal candidiasis, herpes zoster, tuberculosis
- Persistent generalized lymphadenopathy (PGL) — enlarged nodes in ≥2 extra-inguinal sites for >3 months
- Autoimmune thrombocytopenia possible
Phase 3: AIDS (Acquired Immunodeficiency Syndrome)
Definition: CD4+ count <200 cells/μL OR the appearance of an AIDS-defining illness
Pathophysiology:
- Complete breakdown of host cellular immunity
- Dramatic rise in viral load (CD4 cell loss overwhelms regenerative capacity)
- Destruction of lymphoid tissue architecture
CDC Classification (stratifies by CD4 count × clinical category):
| CD4 ≥500/μL | CD4 200–499/μL | CD4 <200/μL | |
|---|---|---|---|
| A: Asymptomatic/PGL/Acute HIV | A1 | A2 | A3 |
| B: Symptomatic, not A or C | B1 | B2 | B3 |
| C: AIDS-indicator conditions | C1 | C2 | C3 |
Clinical features of full-blown AIDS:
- Fever (>1 month), fatigue, weight loss ("AIDS wasting"), diarrhea, generalized lymphadenopathy
AIDS-Indicator (Opportunistic) Infections:
| Organism | Disease |
|---|---|
| Pneumocystis jirovecii | Pneumocystis pneumonia (PCP) — 15–30% of untreated patients |
| Toxoplasma gondii | CNS toxoplasmosis |
| Mycobacterium avium complex | Disseminated MAC infection |
| Candida spp. | Esophageal/tracheobronchial candidiasis |
| Cryptococcus neoformans | Meningitis |
| Cytomegalovirus (CMV) | Retinitis, colitis |
| Mycobacterium tuberculosis | Pulmonary/extrapulmonary TB |
| Cryptosporidium parvum | Chronic diarrhea |
AIDS-Associated Neoplasms:
- Kaposi sarcoma (KS) — caused by HHV-8; most common AIDS-associated tumor
- B-cell lymphomas (EBV-associated) — particularly CNS lymphoma
- Invasive cervical carcinoma (HPV-associated)
Neurological complications:
- HIV-associated neurocognitive disorder (HAND) / AIDS dementia complex
- Vacuolar myelopathy, peripheral neuropathy
- Aseptic meningitis (at seroconversion)
- CNS toxoplasmosis, cryptococcal meningitis
Special Patterns of Progression
| Pattern | Features |
|---|---|
| Rapid progressors | Chronic phase telescoped to 2–3 years |
| Long-term nonprogressors | Asymptomatic >10 years, stable CD4, viral load <5000 copies/mL |
| Elite controllers | Viral load usually <50 copies/mL — vigorous HIV-specific T-cell response, protective HLA alleles |
— Robbins Cotran & Kumar: Pathologic Basis of Disease
4. Diagnosis
A. Serological Tests
1. ELISA (Enzyme-Linked Immunosorbent Assay) — Screening Test
- 4th generation ELISA (currently used): detects both anti-HIV antibodies (IgG/IgM) AND p24 antigen simultaneously
- Detects infection 2–4 weeks after exposure (earlier than antibody-only tests)
- High sensitivity (~99.9%) but lower specificity — positive results must be confirmed
- False positives possible in: autoimmune diseases, multiple pregnancies, recent viral infections, malignancies
2. Western Blot — Confirmatory Test
- Detects antibodies to specific HIV proteins separated by molecular weight
- Positive: bands against ≥2 of: p24, gp41, gp120/160
- Negative: no bands
- Indeterminate: some bands but not meeting criteria → repeat in 4–6 weeks
3. RT-PCR (Real-Time Reverse Transcriptase PCR) — Viral Load / NAT
- Detects HIV RNA directly in plasma
- Used for:
- Early diagnosis (before seroconversion — detects virus in ~10 days)
- Measuring viral load (copies/mL) — monitors disease progression and treatment response
- Neonatal diagnosis (maternal antibodies cross placenta and persist up to 18 months — serology unreliable in infants)
- Resolving indeterminate Western blot
4. CD4+ T Cell Count — Immunological Assessment
- Measured by flow cytometry
- Normal: 500–1500 cells/μL
- Used to:
- Stage disease (CDC classification)
- Determine when to start ART
- Monitor treatment response
- Assess risk of specific opportunistic infections
- AIDS diagnosed when CD4 <200 cells/μL
Diagnostic Algorithm (Summary)
Screening: 4th Gen ELISA (p24 Ag + Ab)
↓ Reactive
Confirmatory: Western Blot or HIV-1/2 differentiation assay
↓ Positive
CD4+ T cell count → Stage disease
Viral load (RT-PCR) → Baseline & monitor therapy
B. AIDS Diagnosis Criteria (CDC)
AIDS is confirmed by:
- HIV-positive status (ELISA + Western blot) AND
- CD4+ T cell count <200 cells/μL OR
- Presence of an AIDS-defining illness (regardless of CD4 count)
C. p24 Antigen Detection
- Useful in the window period before antibody development
- Incorporated into 4th generation combination ELISA assays
— Medical Microbiology 9e; Robbins Cotran & Kumar: Pathologic Basis of Disease
Quick Revision Summary
| Feature | Key Points |
|---|---|
| Causative agent | HIV-1 (retrovirus); RNA virus with reverse transcriptase |
| Target cell | CD4+ T helper cells (also macrophages, DCs) |
| Entry receptors | CD4 (receptor) + CCR5 or CXCR4 (coreceptors) |
| Transmission | Sexual > parenteral (IV drug use, blood) > vertical |
| Phase 1 | Acute retroviral syndrome, high viremia, CD4 drops then recovers |
| Phase 2 | Clinical latency 7–10 yrs; CD4 slowly falls; ongoing lymphoid replication |
| Phase 3 (AIDS) | CD4 <200/μL; opportunistic infections, tumors, neurological disease |
| Screening | 4th gen ELISA (p24 Ag + anti-HIV Ab) |
| Confirmation | Western blot |
| Viral load | RT-PCR — monitors progression & treatment |
| CD4 count | Flow cytometry — stages disease; primary guide for starting ART |
Pneumonia
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Searching Images
lobar pneumonia stages red gray hepatization gross histology
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have all the material I need. Let me now compose the comprehensive pneumonia answer.
Pneumonia — Pathology (Robbins & Kumar)
Definition
Pneumonia is any infection of the lung parenchyma. It accounts for approximately 2.3% of all deaths in the United States and is the most serious respiratory tract infection.
Classification
Pneumonia is classified by clinical setting (which reliably predicts the likely pathogens) and by morphological pattern.
By Clinical Setting
Table: Pneumonia Syndromes (Robbins Cotran & Kumar)
| Syndrome | Common Organisms |
|---|---|
| Community-Acquired Bacterial (CAP) | S. pneumoniae (most common), H. influenzae, M. catarrhalis, S. aureus, Legionella, Klebsiella, Mycoplasma, Chlamydia, Coxiella |
| Community-Acquired Viral | Influenza A & B, RSV, metapneumovirus, adenovirus, rhinovirus, COVID-19 |
| Healthcare-Associated | MRSA, MSSA, P. aeruginosa, S. pneumoniae |
| Hospital-Acquired (Nosocomial) | Gram-negative rods (Klebsiella, Serratia, E. coli, Pseudomonas), MRSA |
| Aspiration | Anaerobic oral flora (Bacteroides, Peptostreptococcus), mixed aerobes |
| Opportunistic (immunocompromised) | Pneumocystis jirovecii, CMV, Aspergillus, Candida, atypical mycobacteria |
| Chronic/Granulomatous | Mycobacterium tuberculosis, Histoplasma, Coccidioides, Blastomyces |
Predisposing Factors / Pathogenesis
Normal lungs are defended by:
- Mucociliary clearance (mucociliary elevator)
- Alveolar macrophages
- Secretory IgA (upper airway)
- Serum IgM/IgG in alveolar lining fluid
- Complement activation
- Recruited neutrophils
Pneumonia results when these defenses are overwhelmed or bypassed:
| Impaired Defense | Mechanism |
|---|---|
| Loss of cough reflex | Coma, anaesthesia, stroke, drugs |
| Mucociliary dysfunction | Cigarette smoke, viral infection, immotile cilia syndrome |
| Secretion accumulation | Cystic fibrosis, bronchial obstruction |
| Macrophage impairment | Alcohol, tobacco, anoxia |
| Pulmonary congestion/oedema | CCF |
| Neutrophil/complement defects | Leads to pyogenic bacterial infections |
| Cell-mediated immunity defects | Leads to intracellular organisms, PCP, herpesviruses |
| Absent spleen | Encapsulated bacteria (pneumococcus) |
Germline mutations in MYD88 (TLR signalling adaptor → NF-κB) are associated with destructive pneumococcal pneumonias.
Morphological Patterns
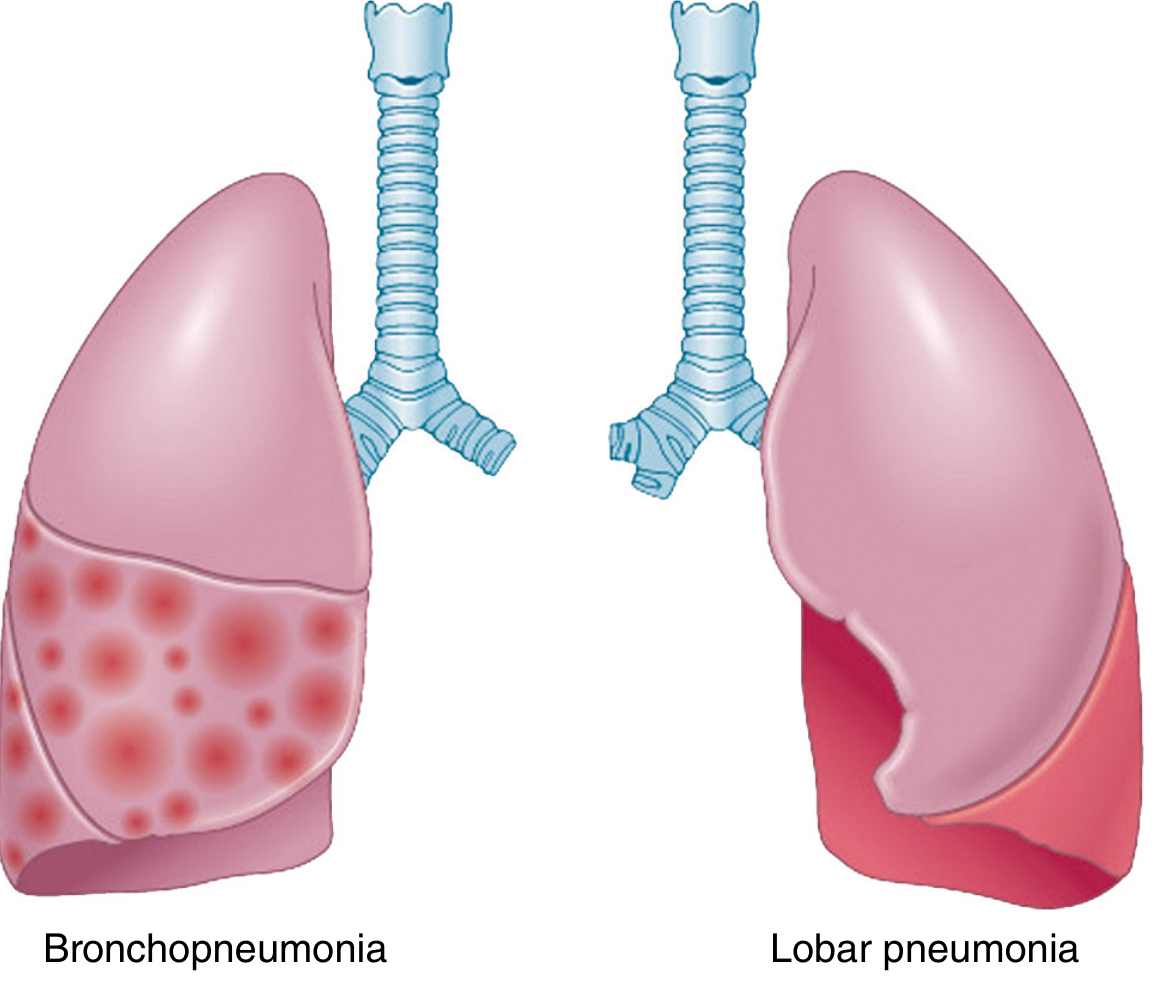
Bacterial pneumonia shows two major anatomical patterns:
1. Lobar Pneumonia
- Consolidation of a large portion or entire lobe
- Caused most often by Streptococcus pneumoniae
- Passes through four classical stages:
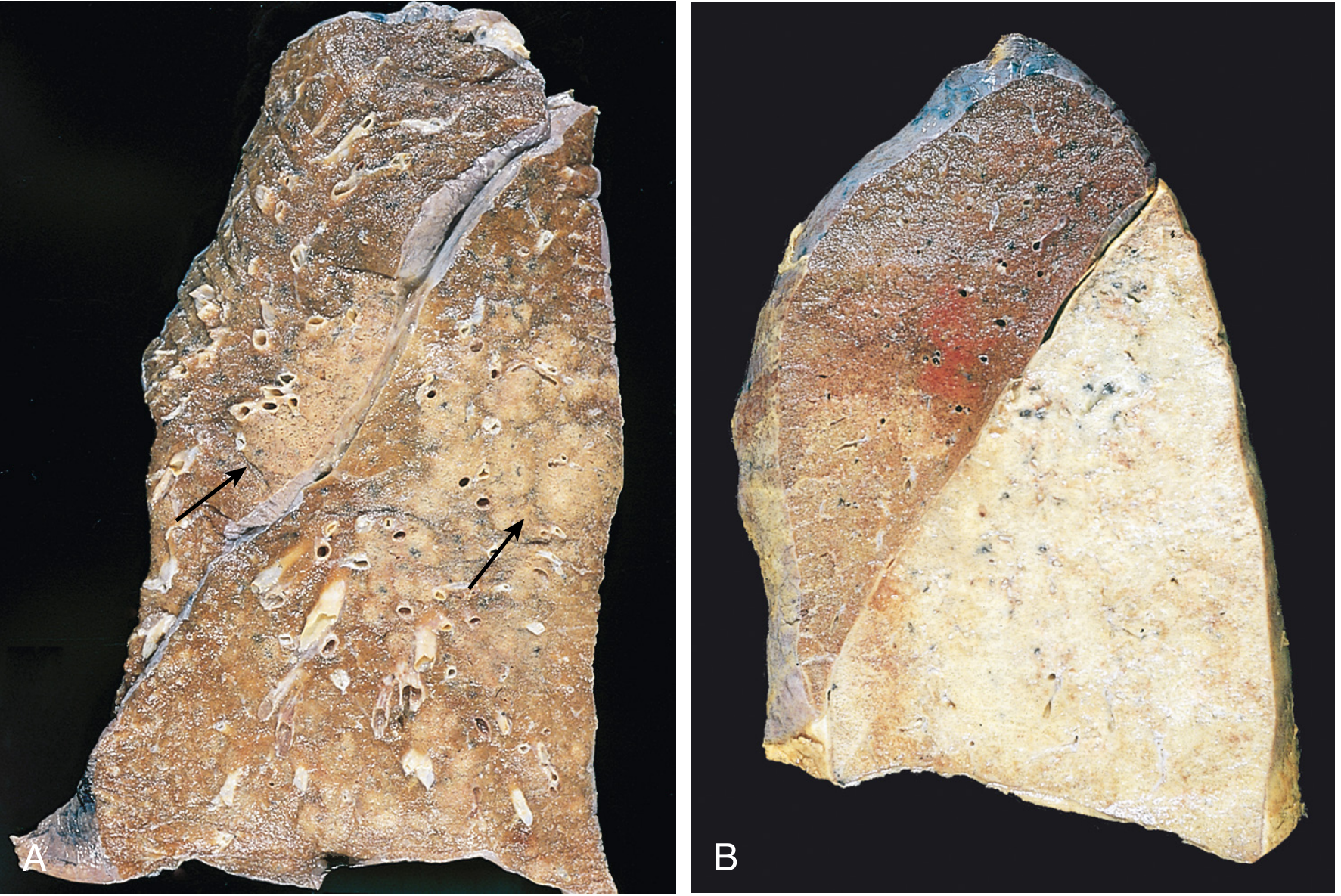
| Stage | Timing | Gross Appearance | Microscopy |
|---|---|---|---|
| 1. Congestion | Days 1–2 | Heavy, boggy, red lung | Vascular engorgement; intra-alveolar oedema fluid; few neutrophils; bacteria present |
| 2. Red Hepatization | Days 3–4 | Red, firm, airless, liver-like consistency | Alveolar spaces packed with neutrophils + red cells + fibrin — massive confluent exudation |
| 3. Gray Hepatization | Days 5–7 | Gray-brown, still firm | Progressive RBC disintegration; fibrinopurulent exudate persists; no red cells |
| 4. Resolution | Day 8+ | Normal aeration restored | Enzymatic digestion of exudate → granular semifluid debris → resorbed / ingested by macrophages / expectorated |
Pleural fibrinous reaction (pleuritis) is often present in the early stages when consolidation reaches the lung surface — may resolve or organize into fibrous adhesions.
2. Bronchopneumonia (Lobular Pneumonia)
- Patchy consolidation — typically multilobar, bilateral, and basal (secretions gravitate to lower lobes)
- Lesions slightly elevated, dry, granular, gray-red to yellow, poorly delimited
- Histology: neutrophil-rich exudate filling bronchi, bronchioles, and adjacent alveolar spaces
- Pattern of involvement depends on the causative organism AND host susceptibility — the same organism can produce either pattern
Causative Organisms — Key Points
Community-Acquired Bacterial (CAP)
S. pneumoniae (Pneumococcus)
- Most common cause of CAP
- Distribution: usually lobar
- Gram stain of sputum: gram-positive, lancet-shaped diplococci in neutrophils
- Capsular polysaccharide vaccines available
- Blood cultures positive in only 20–30% early in illness
Other organisms and associations:
| Organism | Association/Clue |
|---|---|
| H. influenzae, M. catarrhalis | Acute exacerbations of COPD |
| S. aureus | Secondary to viral (influenza) pneumonia |
| Klebsiella pneumoniae | Chronic alcoholics; thick "currant-jelly" sputum |
| Pseudomonas aeruginosa | Cystic fibrosis, neutropenia |
| Legionella pneumophila | Heart/lung disease, transplant recipients, contaminated water (air conditioning) |
| Mycoplasma pneumoniae | "Atypical/walking pneumonia" in young adults; interstitial pattern |
| Chlamydia pneumoniae | Mild atypical pneumonia |
Community-Acquired Viral Pneumonia
- Influenza A & B, RSV, metapneumovirus, adenovirus, COVID-19
- Viruses attach to and enter respiratory epithelial cells → cytopathic changes → cell death → secondary inflammation
- Damage to mucociliary clearance predisposes to bacterial superinfection (often more serious than the primary viral illness)
- Histology: interstitial lymphocytic inflammation (vs. intraalveolar neutrophilic inflammation in bacterial pneumonia)
Atypical Pneumonias
Caused by Mycoplasma, Chlamydia, Legionella, viruses:
- Moderate fever, non-productive cough
- X-ray: patchy interstitial infiltrates disproportionate to clinical findings
- Interstitial inflammation, diffuse alveolar damage
Aspiration Pneumonia
- Debilitated patients with impaired gag/swallowing reflexes (stroke, unconscious, vomiting)
- Chemical + bacterial — gastric acid irritation + oral flora
- Multiple organisms (aerobes > anaerobes)
- Typically necrotizing, fulminant course
- Common complication: lung abscess
Hospital-Acquired (Nosocomial) Pneumonia
- Severely ill, immunosuppressed, prolonged antibiotics, ventilator-dependent patients
- Dominant organisms: gram-negative rods (Klebsiella, Serratia, E. coli, Pseudomonas) + MRSA
- Ventilator-associated pneumonia (VAP): gram-negatives predominate
- High mortality; antibiotic resistance common
Healthcare-Associated Pneumonia
- Risk factors: hospitalization within 90 days, nursing home, IV antibiotics/chemotherapy
- Organisms: MRSA, P. aeruginosa most common
- Higher mortality than CAP; requires broad-spectrum empirical antibiotics
Clinical Features
Acute bacterial pneumonia:
- Abrupt onset of high fever, shaking chills
- Cough with mucopurulent sputum ± haemoptysis
- Pleuritic chest pain + pleural friction rub (if pleuritis present)
- CXR: radiopaque entire lobe (lobar) or focal opacities (bronchopneumonia)
- Appropriately treated patients become afebrile within 48–72 hours of antibiotics
- <10% of hospitalised patients now die (usually from complications or comorbidities)
Atypical/viral pneumonia:
- Gradual onset, moderate fever, non-productive ("dry") cough, headache, myalgia
- CXR: patchy interstitial bilateral infiltrates
Complications
- Lung abscess — tissue destruction/necrosis; especially with S. aureus, Klebsiella, anaerobes
- Empyema — spread to pleural cavity → intrapleural fibrinopurulent reaction
- Bacteraemia/septicaemia → metastatic abscesses, endocarditis, meningitis, suppurative arthritis
- Pleuritis / fibrous adhesions — organizing fibrinous exudate
- Respiratory failure in severe cases
Viral Pneumonia — Histological Distinction
| Feature | Bacterial Pneumonia | Viral Pneumonia |
|---|---|---|
| Inflammation type | Intra-alveolar neutrophilic | Interstitial lymphocytic |
| Exudate | Fibrinopurulent in alveoli | Widened alveolar walls |
| Pattern | Lobar or lobular consolidation | Diffuse, patchy interstitial |
| Sputum | Purulent, coloured | Scanty, mucoid |
Quick Summary Table
| Feature | Lobar Pneumonia | Bronchopneumonia |
|---|---|---|
| Distribution | Entire lobe | Patchy, multilobar, basal |
| Organism | S. pneumoniae | Mixed organisms, S. aureus, gram-negatives |
| Gross | Uniform consolidation | Discrete foci, poorly delimited |
| Stages | 4 stages (congestion → resolution) | No classical stages |
| Age group | Young adults | Extremes of age, debilitated |
| CXR | Lobar opacity with air bronchogram | Patchy bilateral infiltrates |
— Robbins, Cotran & Kumar: Pathologic Basis of Disease
Occupational diseases
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.