Lidocaine
Reading File
Finding Sources
Finding Sources
Searching PubMed
lidocaine clinical use pharmacology
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a comprehensive overview of lidocaine drawn from multiple authoritative sources.
Lidocaine
Class: Vaughan-Williams Class IB antiarrhythmic / Amide local anesthetic
1. Mechanism of Action
As an Antiarrhythmic (Class IB)
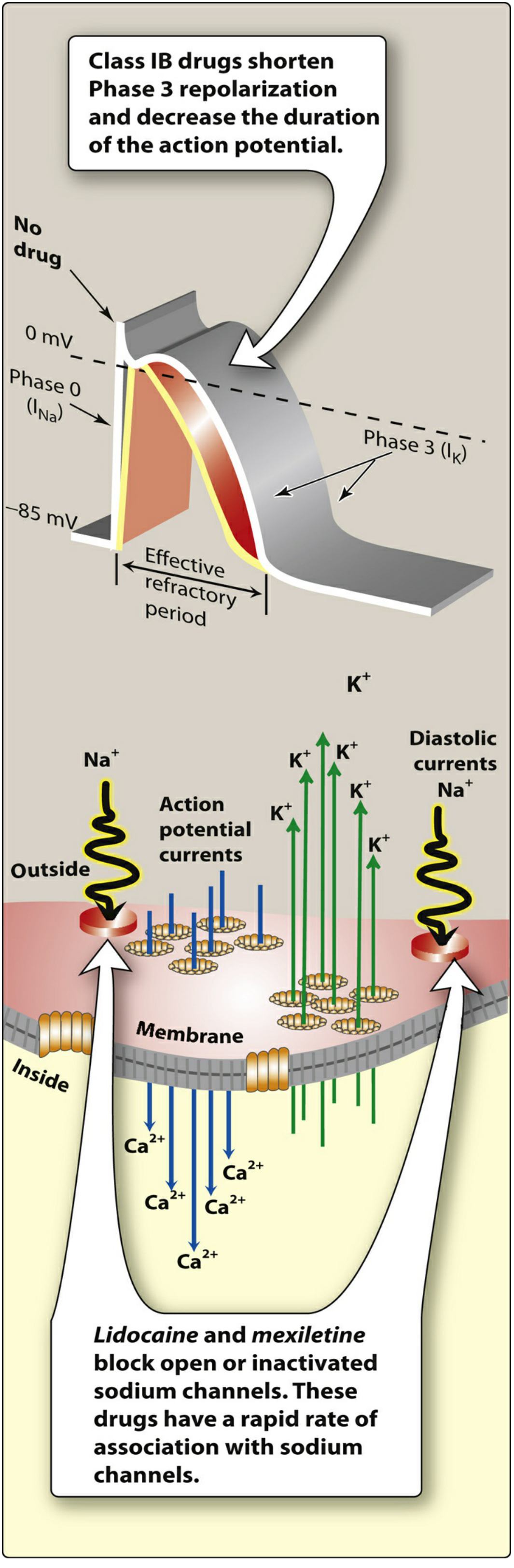
Lidocaine blocks cardiac sodium channels (INa) preferentially in the open or inactivated state, with rapid association and dissociation kinetics ("fast on / fast off"). This means its effects are most pronounced when cells are depolarized or firing rapidly - exactly the conditions of ischemia-driven ventricular arrhythmias.
Key electrophysiologic effects (Braunwald's Heart Disease):
- Shortens phase 3 repolarization and decreases action potential duration (APD) in Purkinje fibers
- Depresses abnormal automaticity (ectopic pacemakers, triggered activity from EADs/DADs) without significantly affecting the normal sinus node at therapeutic doses
- Does not affect atrial tissue or accessory pathways at usual concentrations
- Does not prolong the QT interval
- At higher doses, can convert unidirectional block to bidirectional block during ischemia, preventing VF
- No negative inotropy at therapeutic concentrations
As a Local Anesthetic
Lidocaine blocks voltage-gated Na+ channels on peripheral nerve membranes, preventing depolarization and propagation of action potentials. It works on all nerve fibers (sensory, motor, autonomic), though small unmyelinated C-fibers (pain) are blocked first. Adding epinephrine to the solution causes vasoconstriction, reduces systemic absorption, prolongs duration, and allows a higher maximum dose.
2. Pharmacokinetics
| Parameter | Detail |
|---|---|
| Bioavailability (oral) | Very poor - extensive first-pass hepatic metabolism; oral route is not used for systemic effect |
| Route | IV (antiarrhythmic), IM, topical, subcutaneous/nerve block |
| Metabolism | Hepatic; primarily CYP1A2 (minor CYP3A4) - produces active metabolites that can contribute to toxicity |
| Half-life | ~1-2 h in healthy individuals; >4 h post-MI; >10 h with heart failure; even longer in cardiogenic shock |
| Protein binding | ~70% |
| Hepatic blood flow dependence | YES - heart failure, shock, and beta-blockers all reduce hepatic blood flow and increase lidocaine levels |
Dose reductions of one-third to one-half are required in low cardiac output states. Prolonged infusions also reduce clearance over time.
- Braunwald's Heart Disease, p. 461
- Lippincott Illustrated Reviews: Pharmacology, p. 393-395
3. Clinical Uses
Antiarrhythmic
- Ventricular tachycardia (VT) and ventricular fibrillation (VF): Amiodarone is first-line; lidocaine is the alternative when amiodarone is unavailable or can be used as an adjunct in VT storm (multiple episodes of VT/VF)
- Particularly effective when the mechanism is ischemia-driven (enhanced automaticity)
- No efficacy in SVT - does not affect atrial or AV junctional tissue meaningfully
- Contraindicated in Wolff-Parkinson-White and Stokes-Adams syndrome
Local/Regional Anesthesia
- Infiltration anesthesia, nerve blocks, epidural and spinal anesthesia, topical anesthesia
- Widely used for skin procedures, dental procedures, IV catheter placement, lumbar puncture
- Topical forms used for mucous membranes (oral, urethral), skin (cream, patch)
- Airway topicalization before intubation
Other Uses
- Intravenous lidocaine infusion for perioperative analgesia (multimodal pain management, ileus prevention after GI surgery)
- Topical patch (Lidoderm 5%) for postherpetic neuralgia
4. Dosing
Antiarrhythmic (IV) - Adults
- Loading: 1-2 mg/kg IV at 20-50 mg/min; may give additional boluses of 1 mg/kg at 5-minute intervals (max 3 mg/kg total)
- A second bolus of half the initial dose at 20-40 min helps maintain therapeutic concentration
- Maintenance infusion: 1-4 mg/min (targets plasma level 1-5 mcg/mL)
- Reduce infusion rate in heart failure/shock
Antiarrhythmic - Pediatric (Harriet Lane Handbook)
- Bolus: 1 mg/kg/dose IV (max 100 mg), may repeat in 10-15 min x2; max total 3-5 mg/kg in first hour
- ETT dose: 2-3x the IV dose
- Continuous infusion: 20-50 mcg/kg/min IV/IO (reduce to max 20 mcg/kg/min in shock, CHF, hepatic disease, or cardiac arrest)
Local Anesthetic (Maximum Doses)
- Without epinephrine: 4.5 mg/kg/dose (max 300 mg); do not repeat within 2 hours
- With epinephrine: 7 mg/kg/dose (max 500 mg); do not repeat within 2 hours
Note: For cardiac arrest, amiodarone is preferred over lidocaine; lidocaine is used only when amiodarone is not available. - Harriet Lane Handbook, p. 1213
5. Adverse Effects and Toxicity
CNS Toxicity (dose-related, most common)
Progression with rising plasma levels:
- Nystagmus (early indicator)
- Dizziness, perioral numbness, tinnitus, paresthesias
- Drowsiness, slurred speech, agitation
- Confusion, delirium
- Convulsions/seizures
- Coma, respiratory arrest
Cardiac Toxicity
- Sinus node depression, His-Purkinje block (especially with pre-existing conduction disease)
- Hemodynamically significant effects are rare at usual doses unless left ventricular function is severely impaired
- Asystole can occur, particularly in the setting of acute myocardial ischemia
- Rarely: malignant hyperthermia
Other
- Hypotension
- Anaphylaxis (rare)
- Methemoglobinemia (associated with topical local anesthetic use)
- Braunwald's Heart Disease; Lippincott Illustrated Reviews: Pharmacology
6. Drug Interactions
- Beta-blockers: Decrease hepatic blood flow, increasing lidocaine plasma levels
- CYP1A2 inhibitors (e.g., fluvoxamine, ciprofloxacin): Reduce lidocaine metabolism
- CYP3A4 inhibitors: Minor contribution to metabolism
- CYP 2D6 and 3A3/4 substrate interactions relevant to dosing adjustments
7. Contraindications
- Wolff-Parkinson-White (WPW) syndrome
- Stokes-Adams syndrome
- SA, AV, or intraventricular heart block without a functioning pacemaker
- Severe hepatic failure (relative - use with reduced dosing)
- Known hypersensitivity to amide-type local anesthetics
8. Formulations Available
| Form | Concentration/Strength |
|---|---|
| IV injection | 0.5%, 1%, 1.5%, 2%, 4% |
| IV infusion (pre-mixed in D5W) | 0.4% (4 mg/mL), 0.8% (8 mg/mL) |
| With epinephrine (1:100,000 or 1:200,000) | 0.5-2% lidocaine |
| Topical ointment | 4%, 5% |
| Topical cream | 3%, 4%, 5% |
| Topical gel | 2-5% |
| Transdermal patch | 3.5%, 4%, 5% (Lidoderm) |
| Oral viscous solution | 2%, 4% |
Key Clinical Pearls
- Lidocaine is class IB - the only class IB agent used for emergency rhythm management (Rosen's Emergency Medicine)
- Its usefulness in ischemia-driven VT is related to its state-dependent Na+ channel blockade: blocked, depolarized, or rapidly firing cells (as in ischemia) are more susceptible
- Unlike class IA and IC drugs, lidocaine does not prolong QT or cause torsades de pointes
- Unlike class IC agents, it has no negative inotropy and can be used in structural heart disease
- Oral use is not viable for systemic antiarrhythmic effect due to first-pass metabolism - this is why its oral analog mexiletine exists for chronic oral therapy
Sources: Braunwald's Heart Disease (10e) | Lippincott Illustrated Reviews: Pharmacology | Harriet Lane Handbook (23e) | Rosen's Emergency Medicine | Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.