Here is the complete, integrated radiology reference on pancreatic solid lesions. Given the breadth of the topic I've organized everything into 17 sections. Let me know if you'd like any section expanded further (e.g., EUS, staging tables, radiomics, specific case scenarios, or treatment planning CT for radiation therapy).
Pancreatic Solid Lesions: Comprehensive Radiology Reference
SECTION 1: PANCREATIC CT AND MRI PROTOCOLS
Dedicated Pancreatic CT (MDCT)
The gold standard is multiphasic contrast-enhanced MDCT using water as oral contrast (hydro-CT). Four phases are used:
| Phase | Timing (post-injection) | Primary Purpose |
|---|
| Non-contrast | Baseline | Calcification, hemorrhage, baseline density |
| Pancreatic parenchymal phase (late arterial) | 40-50 sec | PDAC detection (max parenchyma vs. hypoenhancing tumor); hyperenhancing PNETs; vascular anatomy |
| Portal venous phase | 65-70 sec | Liver metastases, venous invasion, lymphadenopathy |
| Delayed phase | 3-5 min | PDAC desmoplastic delayed enhancement; AIP halo; SPN progressive enhancement |
- Slice thickness: 0.6-1.0 mm for multiplanar reconstruction (coronal, sagittal, curved planar)
- Vessel assessment: detailed thin-section reconstructions of SMA, celiac trunk, SMV, portal vein, CHA
- Water as oral contrast prevents masking of hyperdense lesions or vascular blush
MRI Protocol
| Sequence | Key Role |
|---|
| T1W fat-saturated (pre-contrast) | Pancreas is normally T1 bright (zymogen granules); PDAC is T1 dark - single best sequence for detection |
| T2W TSE/HASTE | Cystic lesions, ductal dilation, splenic signal matching (IPAS); SPN capsule |
| DWI (b=0, 500, 800-1000) | Restricted diffusion in malignancy; ADC maps |
| Dynamic post-Gd (arterial, venous, delayed) | Enhancement kinetics: hyper = PNET/IPAS; hypo = PDAC; progressive = fibrous |
| MRCP | Ductal anatomy; double duct sign; BD-IPMN communication; branch duct disease |
| In/out-of-phase (GRE) | Fat content in SPN, lipid lesions |
The most sensitive MRI sequence for pancreatic cancer is T1W fat-saturated immediate post-gadolinium SGE, which shows the hypoenhancing tumor against the brightly enhancing normal parenchyma (Yamada's Gastroenterology, p. 2783).
Split Bolus Technique
Principle: Two contrast boluses injected with a ~75-90 second delay, then one CT acquisition that captures two enhancement phases simultaneously:
- First bolus provides portal venous phase liver enhancement
- Second bolus provides pancreatic parenchymal phase enhancement
- One acquisition = two phases = reduced radiation dose
- Particularly useful in young patients, surveillance protocols, dose-reduction settings
- Limitation: timing is less precise than dedicated dual-phase; not ideal when maximum quality is needed for staging
SECTION 2: PANCREATIC DUCTAL ADENOCARCINOMA (PDAC)
Pathophysiology
PDAC arises from ductal epithelium via a PanIN (pancreatic intraepithelial neoplasia) → PDAC sequence, driven by KRAS mutation (>90%), TP53, SMAD4, CDKN2A. The hallmark is abundant desmoplastic stroma (fibrous tissue > tumor cells) - this produces the imaging signatures of hypoenhancement and delayed enhancement, impedes drug delivery, and confers the aggressive biology. Early spread is perivascular, perineural, and lymphatic. At diagnosis, only 10-20% have resectable disease; 5-year survival ~5-12% (Grainger & Allison, p. 695).
Imaging Findings
Ultrasound:
- Poorly marginated hypoechoic solid mass
- Dilated CBD and/or pancreatic duct (double duct sign in head lesions)
- Loss of normal lobular architecture; parenchymal atrophy upstream
- Doppler: perivascular encasement in advanced disease
- Limitation: body/tail often obscured by bowel gas; insufficient for staging
CT (Pancreatic Parenchymal Phase):
- Pathognomonic: poorly defined hypoenhancing (hypodense) mass against the avidly enhancing normal parenchyma
- Tumor HU typically < 40 vs. normal parenchyma > 80-100 HU in pancreatic phase
- Location: ~70% pancreatic head/uncinate; 20% body; 10% tail
- Upstream pancreatic ductal dilation with parenchymal atrophy distal to obstruction
- Delayed enhancement (3-5 min phase): tumor enhances more due to desmoplastic stroma
- Isoattenuating PDAC (~10-15%): no visible mass but indirect signs present (duct cutoff, atrophy, contour deformity)
- Vascular invasion: encasement, irregularity, or occlusion of SMA, celiac, SMV, portal vein
CT Signs:
- Double duct sign - simultaneous CBD + MPD dilation (head/periampullary tumors) - pathognomonic for head PDAC
- Duct cutoff sign - abrupt termination of dilated MPD at tumor
- Upstream atrophy sign - parenchymal atrophy proximal to obstructed duct
- Teardrop sign - flattening/distortion of SMV by adjacent tumor contact
- Perivascular cuffing - soft tissue encasing mesenteric vessels
MRI:
- T1W fat-sat (pre-contrast): markedly hypointense vs. bright normal pancreas - the most sensitive sequence
- T2W: mildly hyperintense or isointense; desmoplastic stroma = T2 hypointense areas
- DWI: restricted diffusion (ADC ~1.0-1.4 × 10⁻³ mm²/s)
- Post-Gd arterial/venous: hypoenhancing (same as CT)
- Post-Gd delayed: progressive enhancement of desmoplastic stroma
- MRCP: double duct sign, upstream MPD dilation, duct cutoff, stenosis
Differentiating PDAC from Mimics:
| Feature | PDAC | Mass-forming Pancreatitis | AIP | PNET |
|---|
| Enhancement | Hypo, delayed | Iso/hypo, earlier | Delayed + halo | Arterial hyper |
| MPD involvement | Abrupt cutoff, upstream dilation | Gradual, irregular | Long stricture, no upstream dilation | Displacement only |
| Vascular invasion | Common | Uncommon | Uncommon | Encasement (large NF-PNET) |
| Upstream atrophy | Yes | Not always | No (sausage shape) | No |
| IgG4 | Negative | Negative | Elevated (Type I) | Negative |
| Steroid response | No | No | Yes (dramatic) | No |
| CA 19-9 | High | Mild | Mild/negative | Variable |
SECTION 3: VARIANTS OF PANCREATIC CARCINOMA
1. Acinar Cell Carcinoma (ACC)
- ~1-2% of pancreatic malignancies; arises from acinar cells
- Unlike PDAC: typically large, well-circumscribed, exophytic mass
- CT: heterogeneous, partially cystic or necrotic; may show arterial hyperenhancement
- Crucially: often lacks upstream ductal dilation (no desmoplastic duct obstruction) - key differentiator
- Liver metastases common at presentation
- Paraneoplastic - Lipase Hypersecretion Syndrome: subcutaneous fat necrosis (panniculitis), polyarthritis, eosinophilia - pathognomonic for ACC
- AFP may be elevated
- Prognosis better than PDAC but still aggressive
2. Medullary Carcinoma
- Rare variant; syncytial growth pattern with prominent lymphocytic infiltrate (resembling medullary carcinoma of breast/colon)
- MSI-H (microsatellite instability-high) and KRAS wild-type - critical molecular feature
- Imaging: tends to be better-defined, less desmoplastic than conventional PDAC; may be less hypoenhancing; geographic pushing margins
- Clinical significance: responds to immune checkpoint inhibitors (pembrolizumab) due to MSI-H - must not miss this diagnosis
3. Hepatoid Variant of Pancreatic Carcinoma
- Extremely rare; morphologically resembles hepatocellular carcinoma (HCC)
- Produces AFP (alpha-fetoprotein) - paraneoplastic marker
- Imaging: may show arterial hyperenhancement followed by washout pattern, mimicking HCC metastases
- Key differentiator from metastatic HCC: AFP elevation + pancreatic primary + no cirrhosis/liver disease context
- High malignant potential; often diagnosed late
4. Signet Ring Cell Carcinoma of the Pancreas
- Very rare as a primary; must exclude metastatic signet ring carcinoma from stomach, colon, or breast first
- Imaging: diffusely infiltrative, poorly defined, hypodense; may cause diffuse pancreatic enlargement mimicking AIP or lymphoma
- Peritoneal dissemination common at presentation
- Look for co-existing gastric linitis plastica (check stomach carefully on CT/MRI)
- Very poor prognosis
SECTION 4: PANCREATIC NEUROENDOCRINE TUMORS (PNETs)
WHO 2017 Classification
| Grade | Ki-67 | Mitoses/10 HPF | Behavior |
|---|
| NET G1 | <3% | <2 | Benign/low malignant |
| NET G2 | 3-20% | 2-20 | Intermediate |
| NET G3 | >20% | >20 | Malignant (well-differentiated) |
| NEC (large/small cell) | >20% | >20 | Highly malignant |
10-20% associated with genetic syndromes: MEN-1 (most common), VHL, tuberous sclerosis, NF-1 (Yamada's, p. 675).
Functional PNETs - Types and Syndromes
| Tumor | Hormone | Clinical Syndrome | Key Features |
|---|
| Insulinoma | Insulin | Whipple's triad: fasting hypoglycemia, neuroglycopenic symptoms, relief with glucose | Commonest PNET; 90% benign; small (<2 cm); solitary; intrapancreatic; hard to find on CT (occult in ~30%) |
| Gastrinoma | Gastrin | Zollinger-Ellison: refractory peptic ulcers, secretory diarrhea | 60-90% malignant; "Gastrinoma triangle" location; 30-50% in MEN-1 |
| Glucagonoma | Glucagon | 4D syndrome: Dermatitis (necrolytic migratory erythema), Diabetes, DVT, Depression | 70-80% malignant; large; body/tail |
| VIPoma | VIP | WDHA/Verner-Morrison: Watery Diarrhea, Hypokalemia, Achlorhydria | 50-80% malignant |
| Somatostatinoma | Somatostatin | Diabetes, cholelithiasis, steatorrhea, hypochlorhydria | Periampullary; NF-1 association |
| ACTHoma | ACTH | Ectopic Cushing's syndrome | PNET or NEC |
Gastrinoma triangle (boundaries): (1) junction cystic duct/CBD, (2) junction duodenum 2nd/3rd portion, (3) neck of pancreas. Gastrinomas may be extrapancreatic (duodenal wall - common!).
Imaging of PNETs
CT:
- Small PNETs: arterial/pancreatic phase hyperenhancement - the hallmark (hypervascular)
- Larger NF-PNETs: heterogeneous, cystic degeneration, necrosis, calcification (~20%); may be less hypervascular
- Detected best on pancreatic parenchymal phase CT
- On portal venous phase: can become iso/hypoattenuating (wash-out pattern)
- Insulinoma: small, isoattenuating on non-contrast; bright arterial blush; EUS required if CT negative
- Liver metastases from PNET: hypervascular (arterial blush) - distinguish from hypovascular PDAC mets
MRI:
- T1W: hypointense
- T2W: mildly to moderately hyperintense (vs. PDAC T2 iso/hypointense due to fibrosis) - key differential
- Post-Gd: arterial hyperenhancement (discriminating from PDAC)
- DWI: restricted diffusion
Nuclear Medicine:
- Ga-68 DOTATATE PET-CT (somatostatin receptor PET): high sensitivity for SSTR2-expressing tumors; superior to CT for occult primary, staging, and metastases
- Insulinoma: SSTR2-negative → Ga-68 DOTATATE may be negative; use EUS or arterial calcium stimulation test or 18F-DOPA PET
- FDG-PET: positive in poorly differentiated NEC (G3/NEC); inversely correlates with SSTR expression ("flip-flop" phenomenon)
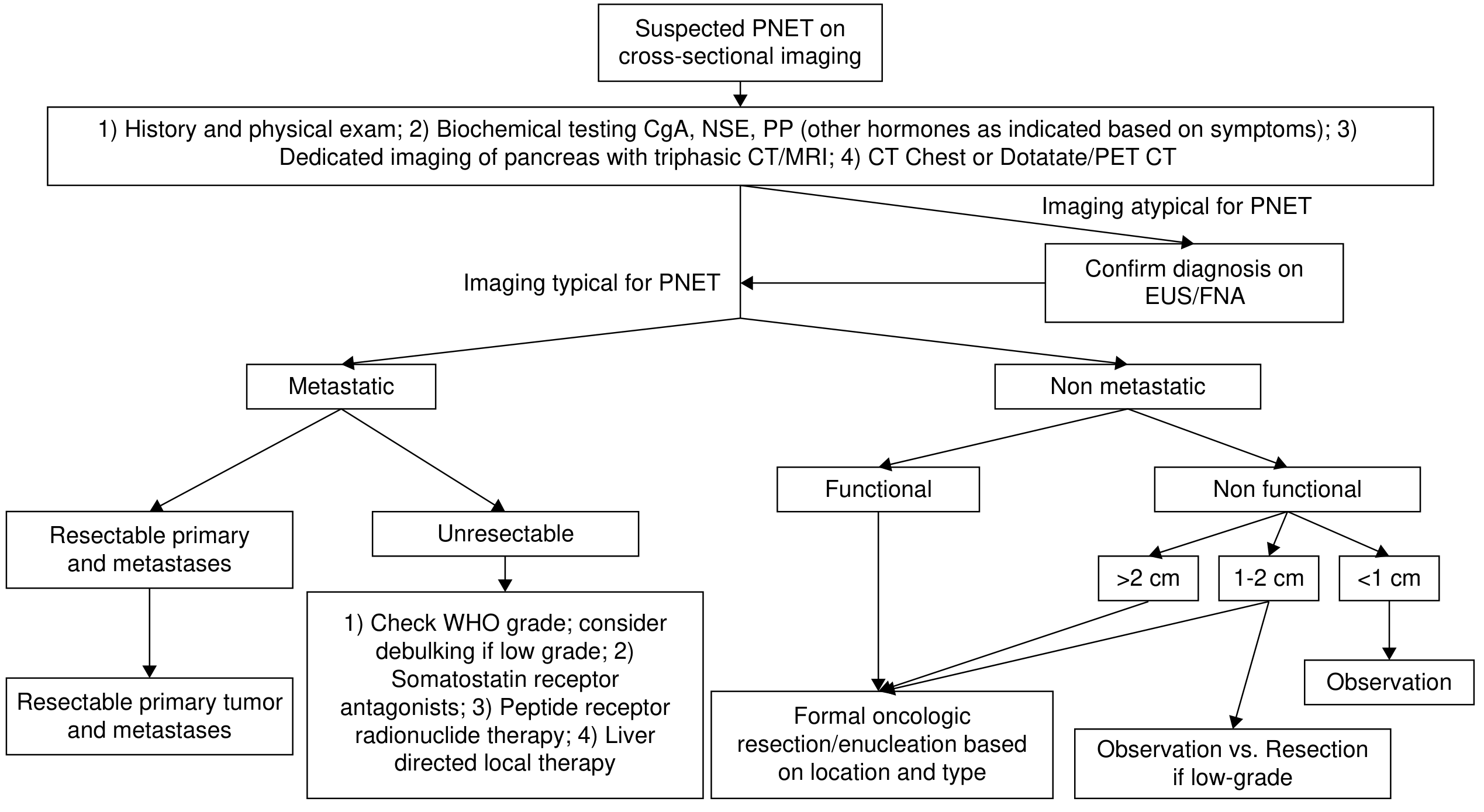
Diagnostic and treatment pathway for suspected PNETs (Current Surgical Therapy 14e)
Non-Functional PNETs (NF-PNETs)
- 60-90% of all PNETs; detected incidentally on cross-sectional imaging
- Presentation: abdominal pain, mass effect, biliary obstruction (head lesions), or incidental finding
- Imaging: same hyperenhancing pattern but larger at discovery; liver mets at presentation ~40%
- Small incidental NF-PNETs <2 cm, no worrisome features: active surveillance is acceptable
SECTION 5: HYPERENHANCING PANCREATIC TUMORS - DIFFERENTIAL DIAGNOSIS
| Diagnosis | Key Differentiating Features |
|---|
| PNET | Most common; T2 bright; Ga-68 DOTATATE positive; hormonal syndromes |
| Metastasis (RCC) | Known renal cell carcinoma history; solitary or multiple; check kidneys; arterial blush |
| Acinar cell carcinoma | Large, heterogeneous; lipase hypersecretion syndrome |
| Solid pseudopapillary neoplasm | Young women; mixed solid-cystic; T1 hemorrhage; encapsulated |
| Intrapancreatic accessory spleen | Exact density/signal match with spleen; pancreatic tail; SPIO/sulfur colloid scan confirms; DOTATATE negative |
| Pancreatic paraganglioma | T2 "light bulb" bright; catecholamine excess; MIBG positive |
| Hepatoid carcinoma | AFP elevated; arterial enhancement + washout |
| PEComa | Fat-containing; tuberous sclerosis; TFE3 fusion |
| Angiosarcoma | Extremely rare; aggressive vascular |
SECTION 6: SOLID PSEUDOPAPILLARY NEOPLASM (SPN / Frantz Tumor)
- <3% of pancreatic neoplasms; young women (20s-30s), F:M = 10:1; low malignant potential (~15% metastatic potential)
- Body/tail predominance; typically large (>4 cm) at presentation
- Mutations: CTNNB1 (beta-catenin) - nuclear accumulation on immunohistochemistry
CT:
- Well-encapsulated mixed solid-cystic mass with thick fibrous capsule
- Peripheral solid component + central cystic/necrotic/hemorrhagic areas
- Capsule: eggshell calcification (characteristic when present)
- Heterogeneous enhancement of solid components; capsule enhances
MRI:
- T1W: hyperintense foci (intratumoral hemorrhage) - the hallmark on MRI
- T2W: heterogeneous; fibrous capsule = T2 hypointense rim
- In/out-of-phase: no signal drop (no intracellular fat)
- Post-Gd: progressive solid component enhancement
- DWI: restricted diffusion in solid parts
- The triad of T1 hyperintense hemorrhage + T2 hypointense capsule + young woman = near-diagnostic
SECTION 7: MUCINOUS CYSTIC NEOPLASM (MCN)
- Exclusively in women (>95%); body/tail predominance
- Does NOT communicate with the main pancreatic duct - key differentiator from IPMN
- Histological hallmark: ovarian-type stroma in the wall
- Malignant potential: ~15% (mucinous cystadenocarcinoma)
- Cyst fluid: CEA > 192 ng/mL supports mucinous etiology
Imaging:
- Unilocular or oligolocular macrocystic mass with thick wall, septa, possible mural nodules
- Peripheral eggshell calcification (when present - suggests malignancy in context of MCN)
- CT: macrocystic lesion in body/tail, thin-to-thick septations, fluid-filled
- MRI T2W: high signal fluid; T1W: proteinaceous content may be T1 bright
- Mural nodule + enhancement: worrisome for malignant transformation → resection
Mucinous cystadenoma: macrocystic body/tail mass with thin septations on CT and T2W MRI (Grainger & Allison)
SECTION 8: SEROUS CYSTIC NEOPLASM (SCN)
- Almost always benign (serous cystadenocarcinoma exceedingly rare)
- More common in older women (7th decade); pancreatic head
- VHL syndrome association (pancreatic cysts + SCN)
Pathognomonic features:
- Microcystic (honeycomb) pattern: innumerable small cysts (<1-2 cm each)
- Central stellate scar with sunburst/radiating calcification (30-40%) - pathognomonic
- CT: lobulated mass, hypodense microcysts, central enhancing scar
- MRI T2W: markedly hyperintense microcysts clustered around central scar; septations enhance
- Macrocystic (oligocystic) variant: larger cysts; can mimic MCN or pseudocyst - diagnostic challenge
- No mural nodules; no ductal communication
Serous cystadenoma: microcystic mass with enhancing central scar, no solid nodule (Grainger & Allison)
SECTION 9: IPMN - INTRADUCTAL PAPILLARY MUCINOUS NEOPLASM
Three Types (Grainger & Allison, p. 706)
| Type | Features | Malignancy Risk |
|---|
| Main duct (MD-IPMN) | Diffuse/segmental MPD dilation >5 mm; mucin from patulous ampulla ("fish mouth" ampulla endoscopically); no mass | 57-92% |
| Branch duct (BD-IPMN) | Sac-like cyst communicating with MPD; grape-cluster cysts; no MPD dilation | 15-25% |
| Mixed type | Both MD + BD involvement | ~MD risk |
- MRCP: ideal for showing MPD communication (MinIP reconstructions; grape-like cluster = BD-IPMN)
- CT/MRI have similar diagnostic performance for malignant vs. benign IPMN
Malignant Transformation - Imaging Warning Signs (Fukuoka Guidelines)
"Worrisome features" (→ EUS evaluation):
- Cyst ≥ 3 cm
- Enhancing mural nodule < 5 mm
- Thickened/enhanced cyst wall
- MPD 5-9 mm caliber
- Abrupt MPD change with upstream atrophy
- Lymphadenopathy
- Rapid growth > 5 mm/2 years
- Elevated CA 19-9
"High-risk stigmata" (→ direct surgical resection):
- Obstructive jaundice + cystic head lesion
- Enhancing mural nodule ≥ 5 mm
- MPD ≥ 10 mm caliber
Which IPMN types undergo malignant transformation most?
- Main duct type >> Branch duct type in malignant risk
- Management: MD-IPMN → surgery; BD-IPMN < 3 cm in asymptomatic patients → serial imaging surveillance
SECTION 10: PANCREATIC METASTASES
- Most common primaries: RCC (~70% of pancreatic mets), lung, breast, colon, melanoma
- RCC mets: arterial hyperenhancing, multiple, can be solitary; arterial blush; can occur decades after nephrectomy
- Lung/colon/breast mets: hypovascular, hypodense
- Melanoma mets: may be T1 hyperintense (melanin); can be hypervascular
- Key imaging clue: known primary elsewhere + interval appearance + multiple lesions + no upstream ductal changes unless infiltrative
- Solitary hypervascular met from RCC can perfectly mimic PNET - clinical history is decisive
SECTION 11: INFLAMMATORY PANCREATIC MASSES
Mass-Forming Pancreatitis (MFP) / Chronic Pancreatitis with Mass
- Background of chronic pancreatitis (alcohol, stones, duct changes)
- CT: ill-defined, iso/hypodense mass; calcifications common; irregular duct dilation (not abrupt cutoff)
- Differentiators from PDAC:
- Gradual/irregular ductal dilation (not abrupt cutoff)
- Calcifications more common
- No vascular encasement
- Pseudocysts may coexist
- Less markedly elevated CA 19-9
- Clinical: chronic alcohol use, recurrent pancreatitis
Groove Pancreatitis (Paraduodenal Pancreatitis)
- Fibro-inflammatory process in the groove between the pancreatic head, duodenum, and CBD
- Associated with chronic alcohol use and cystic dystrophy of the duodenal wall
- CT: sheet-like hypodense soft tissue plaque in the groove; can cause CBD/PD narrowing; no vascular invasion
- MRI T2W: cystic spaces within the duodenal wall (Santorini duct cysts) - pathognomonic
- MRCP: smooth CBD narrowing; no duct invasion
- Key distinguishing features: groove location; T2 duodenal wall cysts; no vascular involvement; alcohol history
Autoimmune Pancreatitis (AIP)
Two types:
| Feature | Type I (IgG4-related) | Type II (IDCP) |
|---|
| Serum IgG4 | Elevated (×2 ULN = highly specific) | Normal |
| Extrapancreatic | Yes: bile ducts, kidney, salivary, aorta | No |
| Histology | LPSP (lymphoplasmacytic sclerosing) | IDCP with GEL (granulocyte epithelial lesion) |
| Age/Sex | Older males | Younger; IBD association |
| Focal mass | Less common | Up to 35% |
Imaging (Current Surgical Therapy 14e, p. 599; Grainger & Allison, p. 647-648):
Classic diffuse form:
- Sausage-shaped diffusely enlarged pancreas with homogeneous attenuation and loss of normal lobulations
- Halo/capsule sign: hypoattenuating rim around the pancreas (periductal fibrosis) - characteristic
- Little to no visible pancreatic duct
- No upstream ductal dilation
Focal form (mimics PDAC in head):
- Mass with disproportionately mild upstream ductal dilation relative to mass size (vs. PDAC)
- Halo sign still present
- No vascular encasement
- Long-segment or multiple duct strictures without upstream dilation (MRCP/ERCP)
- IgG4-related extrapancreatic signs: biliary strictures (PSC-like), renal hypodense masses, retroperitoneal fibrosis, lymphadenopathy, salivary/lacrimal gland enlargement
CEUS differentiation: AIP = isoenhancement arterial + hyperenhancement late phase vs. PDAC = hypoenhancing throughout.
Steroid response: dramatic, near-complete resolution within weeks - both diagnostic and therapeutic.
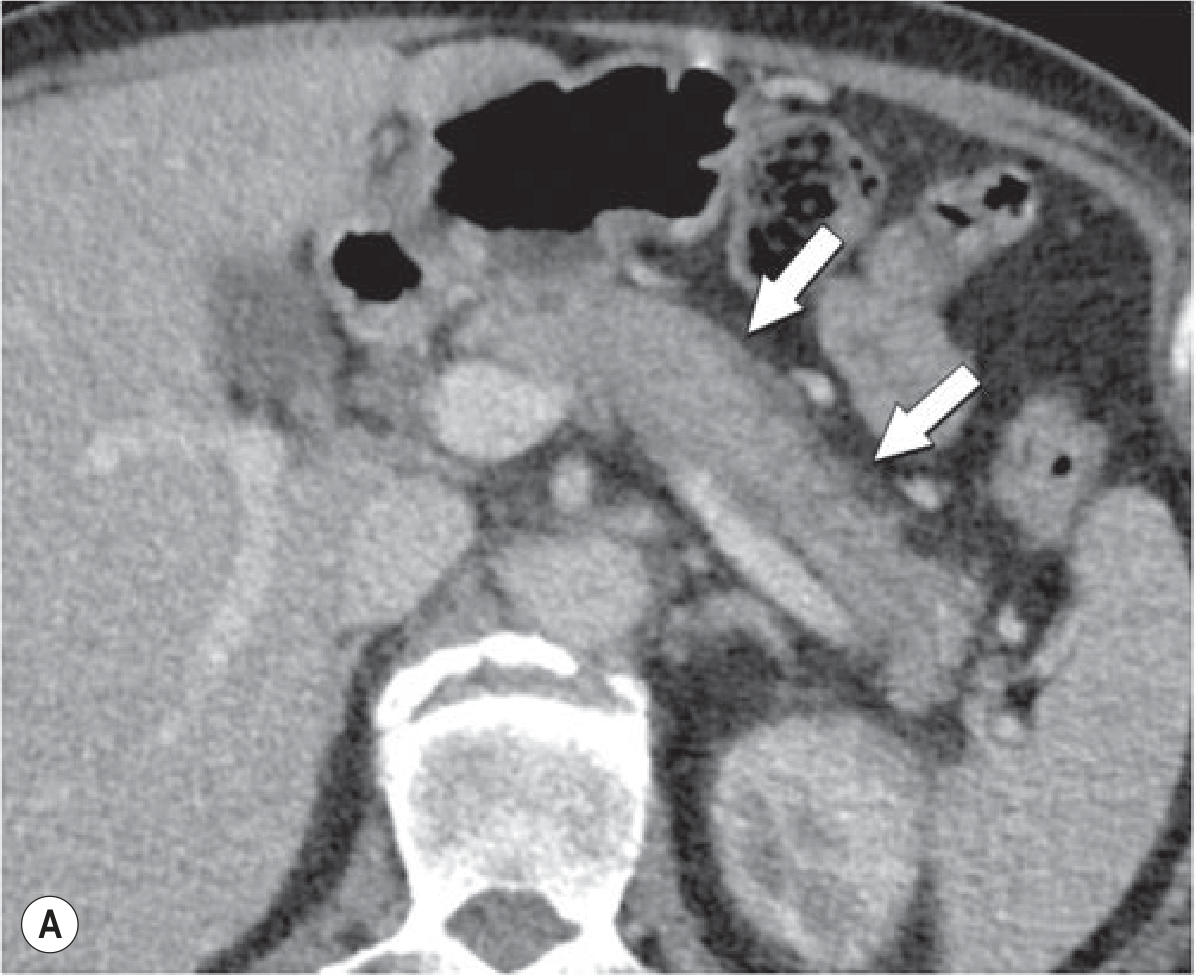
AIP: lobulated hypodense head mass mimicking PDAC (left: CT; right: sagittal) (Current Surgical Therapy 14e)
AIP diffuse form: sausage-shaped gland with hypoattenuating peripheral halo on MDCT (Grainger & Allison)
SECTION 12: ECTOPIC SPLENIC TISSUE IN PANCREAS
Intrapancreatic Accessory Spleen (IPAS)
- Located in pancreatic tail (>95%); benign; asymptomatic
- Most important clinical issue: do not mistake for a hypervascular PNET
Imaging:
- CT/MRI: exact density/signal match with splenic parenchyma on every phase - follows splenic enhancement curve perfectly (non-contrast, arterial, portal, delayed all identical to spleen)
- MRI T2W: isointense to spleen; in/out-of-phase: no fat drop
- SPIO-enhanced MRI: Kupffer cell/RES uptake identical to spleen
- Tc-99m sulfur colloid scan or heat-damaged RBC scan: uptake in pancreatic tail mass = spleen - confirmatory
- Ga-68 DOTATATE PET: negative in IPAS vs. positive in PNET - most useful differentiator
SECTION 13: PANCREATIC PARAGANGLIOMA
- Extremely rare; arises from paraganglia within or adjacent to pancreas
- Symptoms: hypertension, headache, palpitations (catecholamine excess) OR incidental
- CT: well-defined, arterial hyperenhancing mass; cystic degeneration possible
- MRI: T2W markedly hyperintense ("light bulb" sign) - identical to adrenal pheochromocytoma
- MIBG scintigraphy: positive in secretory tumors
- Ga-68 DOTATATE PET: often positive (SSTR expression)
- Biochemistry: elevated plasma/urine metanephrines - differentiates from PNET
- Caution: pre-operative alpha-blockade MANDATORY before biopsy or surgery; biopsy without blockade can cause hypertensive crisis
SECTION 14: ASSOCIATED SYNDROMES AND SIGNS
Hereditary/Genetic Syndromes
| Syndrome | Pancreatic Lesion |
|---|
| MEN-1 | Multiple PNETs (gastrinoma most common), insulinoma; pancreatic involvement in 80% |
| VHL | Non-functional PNETs (often clear cell); pancreatic cysts (>70%); SCN |
| Tuberous Sclerosis | PNETs (rare); pancreatic hamartomas |
| NF-1 | Periampullary somatostatinoma; GIST |
| Familial PDAC (BRCA1/2, PALB2, ATM, CDKN2A) | Elevated PDAC risk; screen with annual EUS/MRI |
| Peutz-Jeghers (STK11) | High PDAC lifetime risk (~36%) |
| Lynch syndrome (MSI-H) | Medullary carcinoma variant of PDAC |
| Hereditary pancreatitis (PRSS1/SPINK1) | Chronic pancreatitis → PDAC (up to 40% lifetime risk) |
Radiological Signs
| Sign | Lesion | Description |
|---|
| Double duct sign | PDAC (head) | Simultaneous CBD + MPD dilation on MRCP/CT |
| Duct cutoff sign | PDAC | Abrupt termination of dilated MPD at tumor |
| Upstream atrophy | Obstructing mass | Parenchymal atrophy proximal to obstruction |
| Sausage sign | AIP | Diffuse pancreatic enlargement, smooth outline, loss of lobulations |
| Halo/capsule sign | AIP | Hypoattenuating peripancreatic rim on CT |
| Teardrop sign | PDAC | Distortion/flattening of SMV profile by tumor |
| Santorini duct cysts | Groove pancreatitis | Cystic spaces within duodenal wall on T2W MRI |
| Fish-mouth/patulous ampulla | Main duct IPMN | Mucin extruding from gaping ampulla |
| Sunburst calcification | SCN | Central scar + radiating calcification on CT |
| Eggshell calcification | MCN/SPN | Peripheral capsular calcification |
| Whirlpool sign | SPN/any | Capsule + internal architecture |
Paraneoplastic Syndromes
| Syndrome | Tumor | Mechanism |
|---|
| Trousseau syndrome (migratory thrombophlebitis) | PDAC (classic) | Tumor procoagulant, mucin |
| Lipase hypersecretion syndrome (fat necrosis, polyarthritis, eosinophilia) | Acinar cell carcinoma | Circulating lipase/trypsin |
| Necrolytic migratory erythema (NME) | Glucagonoma | Excess glucagon |
| Cushing syndrome (ectopic ACTH) | ACTHoma, NEC | Ectopic ACTH secretion |
| Hypoglycemia | Insulinoma; IGF-2 tumor | Hyperinsulinism |
| Watery diarrhea/WDHA | VIPoma | VIP excess |
| Hypercalcemia | PTHrP-secreting PNET | Ectopic PTHrP |
| Carcinoid syndrome | Serotonin-secreting PNET (rare) | 5-HT excess |
SECTION 15: RESECTABILITY CRITERIA (NCCN 2024)
| Category | Arterial Criteria | Venous Criteria (SMV/PV) |
|---|
| Resectable | No solid tumor contact with SMA, celiac trunk, CHA | No contact OR ≤180° without vein contour irregularity |
| Borderline Resectable | SMA ≤180° contact; CHA contact without extension to celiac or hepatic bifurcation; celiac ≤180° (body/tail tumors) | >180° contact; OR ≤180° with contour irregularity/thrombosis but vessel is reconstructable |
| Locally Advanced / Unresectable | SMA or celiac >180° contact; aortic involvement; unreconstructable CHA | SMV/PV occlusion without reconstructable vessel |
Key principles:
- CT has >90% predictability for unresectable disease
- R0 resection predicted by preserved fat plane between tumor and adjacent vessels
- Arterial anatomical variants (replaced RHA, replaced LHA) must be documented - changes surgical approach
- Post-NAT: NCCN recommends against formal restaging as decrease in tumor size/vascular contact does not reliably equate to pathological downstaging; if no progression → trial dissection
Radiology reporting template essentials (PACT-UK/NCCN):
- Tumor size and exact location
- Distance/contact with SMA, celiac, CHA, GDA, splenic artery, SMV, PV, splenic vein
- Degree of circumferential contact (in degrees) for each vessel
- Contour irregularity, thrombosis, teardrop deformity
- Arterial variants (replaced RHA arising from SMA - ~20% of patients)
- Lymph node status
- Distant disease (liver, peritoneum, extra-abdominal)
SECTION 16: DUAL ENERGY CT (DECT) IN PANCREATIC PATHOLOGY
Principles
DECT acquires data at two photon energy levels simultaneously. Key outputs:
- Virtual monoenergetic images (VMI): at 40-50 keV, iodine contrast is amplified → better tumor conspicuity
- Iodine density maps (iodine material decomposition): quantify iodine concentration in each voxel → reflect vascularity
- Virtual non-contrast (VNC): subtract iodine to estimate non-contrast appearance → reduces need for true non-contrast scan
Applications
1. PDAC Detection
- Low keV VMI (40-50 keV): amplifies the hypoenhancing tumor against brighter parenchyma - PDAC conspicuity significantly improved
- Iodine maps: PDAC has low iodine concentration (reflects desmoplastic hypovascular stroma); normal parenchyma has high iodine
- Normalized Iodine Concentration (NIC) tumor < parenchyma = supports PDAC
- Detects isoattenuating PDAC occult on conventional CT
- Improves margin sharpness and reproducibility of tumor measurements (Insights Imaging, 2022)
2. Differentiating PDAC from Mass-Forming Pancreatitis
- AIP/MFP: isoenhancing → higher iodine concentration on iodine map
- PDAC: lower iodine density → clear separation on iodine maps
3. PNETs
- Hyperenhancing PNETs: high iodine density on arterial phase iodine maps
- Treatment response: decrease in iodine density correlates with anti-tumor response (e.g., Lenvatinib) - better than size alone
4. Treatment Response Monitoring
- Iodine uptake by PDAC post-chemotherapy reflects vascular response before anatomical size change
- Quantitative iodine mapping may add value over conventional CT for monitoring NAT response (Johns Hopkins, Abdom Radiol 2018)
5. Radiation Dose Reduction
- VNC images eliminate need for true non-contrast phase in some protocols
- Split-detector or rapid kV-switching DECT allows single-acquisition dual-phase imaging
6. Photon-Counting Detector CT (PCD-CT, 2025)
- Next-generation DECT; thinner slices, reduced noise, superior iodine density maps
- Improved PDAC conspicuity vs. conventional DECT (Abdom Radiol, April 2025)
QUICK REFERENCE TABLE: Pancreatic Solid Lesions
| Lesion | CT Enhancement | Key MRI | Demographics | Hallmark Sign |
|---|
| PDAC | Hypo (pancreatic phase), delayed | T1 hypointense (fat-sat), DWI restrict | M>F, >60y | Double duct sign, upstream atrophy |
| PNET | Arterial hyper | T2 mildly bright, DWI restrict | Any age | Ga-68 DOTATATE positive |
| SPN | Progressive solid | T1 hyper (hemorrhage), T2 capsule | Young women F:M 10:1 | T1 bright hemorrhage + capsule |
| ACC | Variable/hyper | T2 heterogeneous | M>F | Lipase syndrome; no duct dilation |
| Hepatoid | Arterial hyper + washout | T1 hyper (bile-like) | Any | AFP elevated |
| MCN | Macrocystic, septated | T2 bright, T1 proteinaceous | Women, body/tail | No PD communication; ovarian stroma |
| SCN | Microcystic, central scar | T2 innumerable bright cysts | Older women, head | Sunburst calcification; central scar |
| IPMN (MD) | MPD dilation | MRCP: MPD >5 mm | Any, older | Patulous ampulla |
| AIP | Delayed + halo | T2 sausage, capsule hypointense | Older M (I); Young IBD (II) | Sausage sign; halo; steroid response |
| Groove pancreatitis | Groove plaque | T2 duodenal wall cysts | M, alcohol | Santorini duct cysts |
| IPAS | Identical to spleen all phases | Identical to spleen | Any | DOTATATE negative; sulfur colloid uptake |
| Paraganglioma | Arterial hyper | T2 light bulb bright | Any | Metanephrines elevated |
| RCC met | Arterial hyper | Heterogeneous | Prior RCC | Known primary; hypervascular |
| Lymphoma | Homogeneous, mild | Iso, minimal enhance | Any, systemic | No calcification, no necrosis, peripancreatic nodes |
Sources: Grainger & Allison's Diagnostic Radiology (pp. 695-710); Yamada's Textbook of Gastroenterology 7e (pp. 2771-2785); Current Surgical Therapy 14e (pp. 599, 675-682); NCCN Pancreatic Adenocarcinoma Guidelines v3.2024; Abdominal Radiology 2025 (PCD-CT PDAC); Insights into Imaging 2022 (DECT iodine maps PDAC); PMC 2024 (PACT-UK Radiology Template)