Blood supply of heart
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have more than enough material to write a comprehensive, well-cited answer. Let me compile the full response.
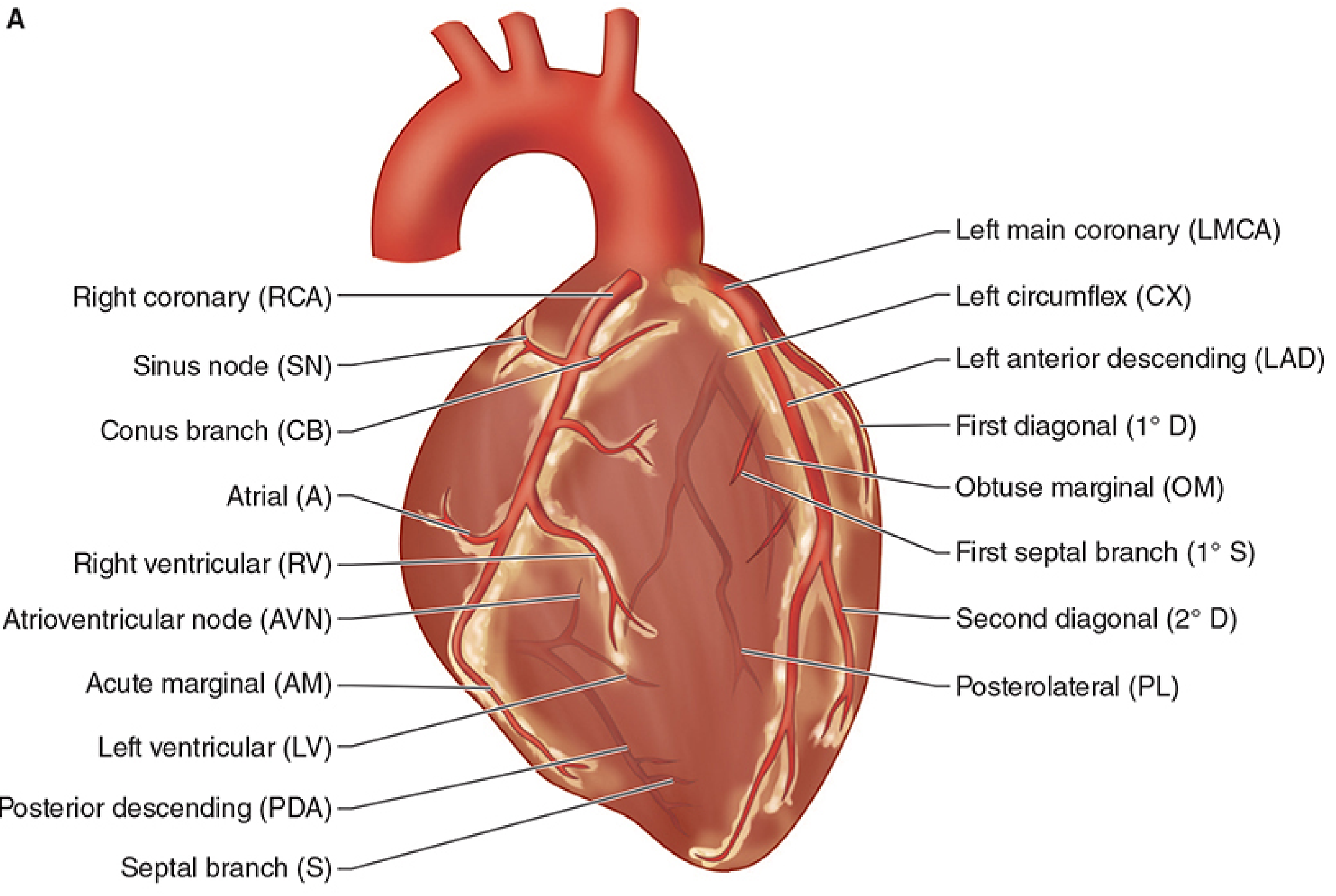
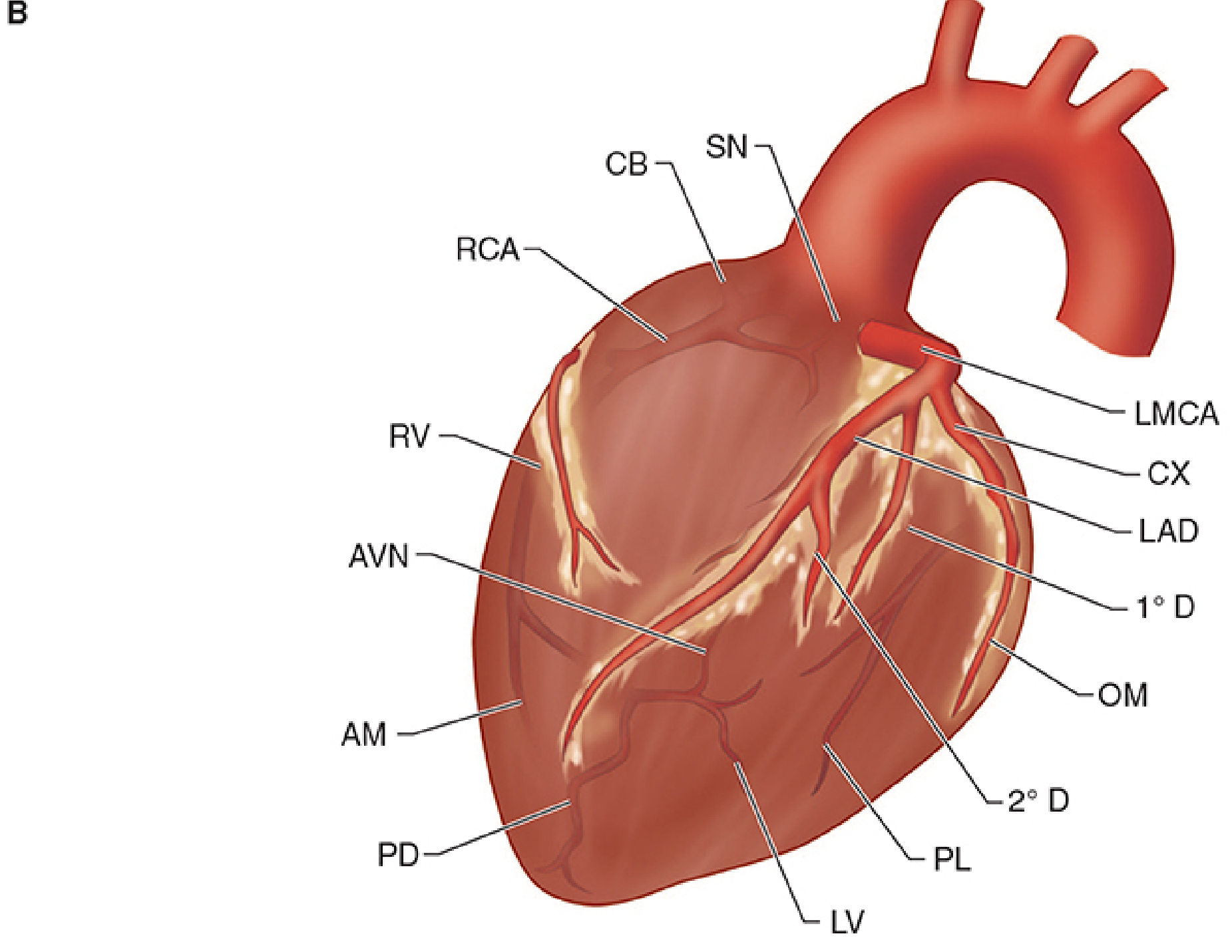
Blood Supply of the Heart
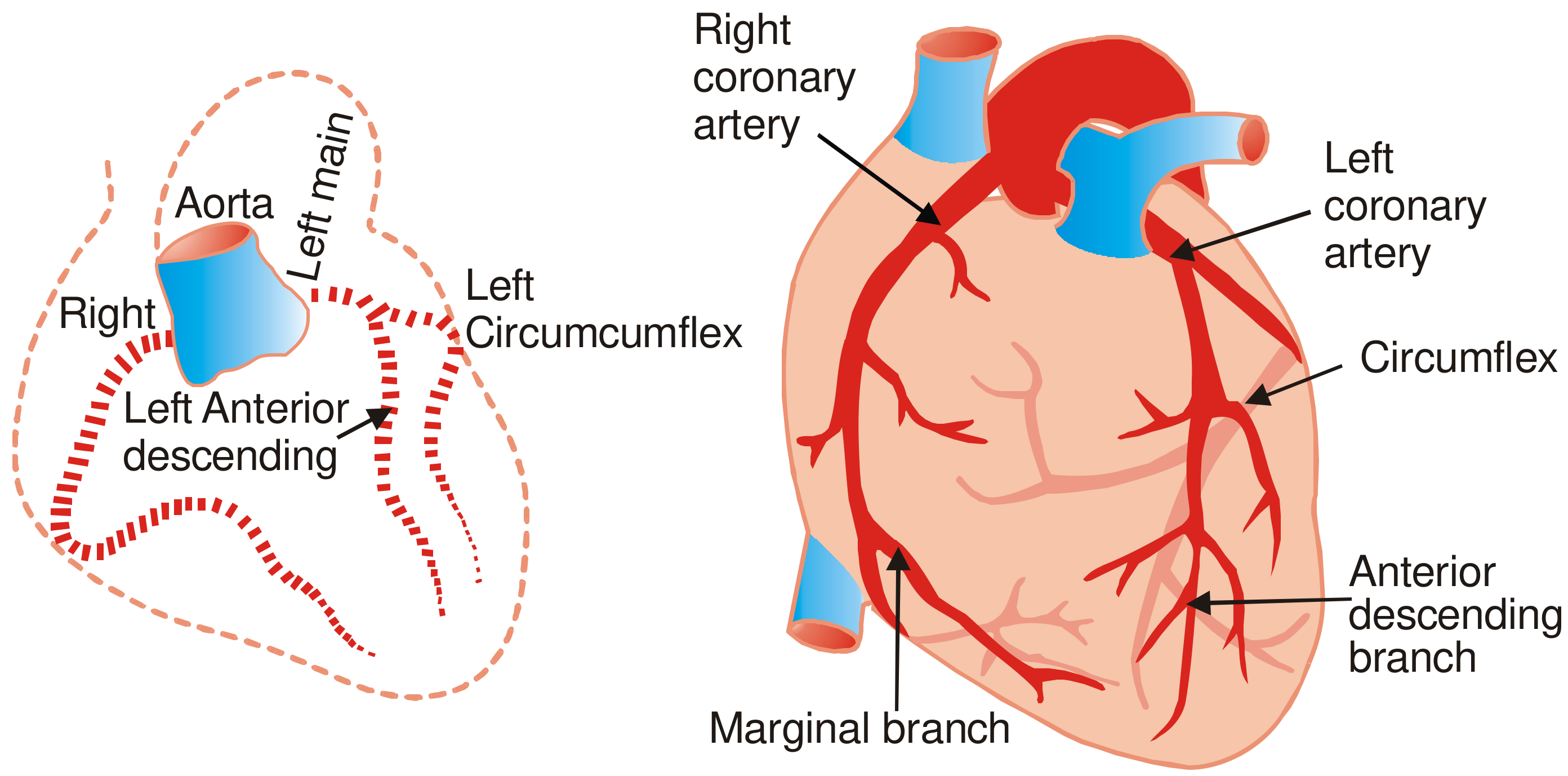
The heart receives its entire arterial supply from two vessels - the right coronary artery (RCA) and the left coronary artery (LCA) - both arising from the aortic sinuses at the root of the ascending aorta. Blood flows from epicardial to endocardial vessels. As blood recoils after ventricular contraction and fills the aortic sinuses, it is automatically directed into the coronary ostia.
(Morgan and Mikhail's Clinical Anesthesiology, 7e; Gray's Anatomy for Students)
Arterial Supply
A. Right Coronary Artery (RCA)
- Arises from the right aortic sinus of the ascending aorta
- Passes behind the pulmonary trunk and descends in the right atrioventricular (coronary) sulcus between the right atrium and right ventricle
- On reaching the inferior border, it turns posteriorly and continues toward the posterior surface
Branches of the RCA:
| Branch | Territory Supplied |
|---|---|
| Sinus node (SA nodal) artery | SA node (in ~60% of people; LAD supplies it in ~40%) |
| Conus branch | Infundibulum (outflow tract) of right ventricle |
| Right ventricular (acute marginal) branch | Anterior and lateral walls of right ventricle |
| Right marginal branch | Right border of heart; anterior RV surface, posterior third of interventricular septum |
| Posterior descending artery (PDA) | Posterior interventricular septum; inferior wall of LV |
| AV nodal artery | AV node (in 85-90% of people - "right dominant") |
In right dominant circulation (85% of people), the RCA gives rise to the PDA. The RCA thus supplies: right atrium, most of the right ventricle, and the inferior wall of the left ventricle.
B. Left Coronary Artery (LCA)
- Arises from the left aortic sinus of the ascending aorta
- The left main coronary artery (LMCA) is short (a few centimeters) and then bifurcates into two major branches:
1. Left Anterior Descending (LAD) - "Anterior Interventricular Artery"
- Descends in the anterior interventricular sulcus toward the cardiac apex
- Supplies: Anterior wall of left ventricle, anterior two-thirds of the interventricular septum (via septal perforators), and the apex
Branches of LAD:
- Septal perforating branches - supply the anterior interventricular septum and the bundle of His (dual supply with PDA)
- Diagonal branches (1st diagonal, 2nd diagonal) - supply the anterolateral LV wall
The LAD is the most commonly occluded coronary artery (45-64% of fatal coronary stenoses), hence called the "widow maker". (P C Dikshit Textbook of Forensic Medicine)
2. Left Circumflex Artery (CX / LCx)
- Wraps posteriorly around the left AV groove
- Supplies: Left atrium and the lateral wall of the left ventricle
Branches of LCx:
- Obtuse marginal branches - supply the lateral LV wall
- AV nodal artery (in ~10-15% of people where LCx is dominant)
Coronary Dominance
The concept of dominance is determined by which artery gives rise to the posterior descending artery (PDA):
| Dominance | Frequency | PDA origin |
|---|---|---|
| Right dominant | ~85% | RCA |
| Left dominant | ~15% | Circumflex (CX) - wraps around AV groove and continues as PDA |
| Co-dominant | Rare | Both RCA and LCx contribute |
In left dominant circulation, the CX also supplies most of the posterior septum and inferior wall (in addition to the left atrium and lateral wall).
(Morgan and Mikhail's Clinical Anesthesiology, 7e; Gray's Anatomy for Students)
Blood Supply to the Conduction System
| Structure | Primary supply | Notes |
|---|---|---|
| SA node | RCA (60%) or LAD (40%) | Variability is common |
| AV node | RCA (85-90%), rarely LCx (10-15%) | Most vulnerable in right coronary occlusion |
| Bundle of His | Dual: PDA + LAD (septal perforators) | Protected by dual supply |
| Right bundle branch | LAD (septal perforators) | |
| Left bundle branch | LAD + PDA | Dual supply |
| Anterior papillary muscle (mitral) | Dual: diagonal branches of LAD + marginal branches of CX | Relatively protected |
| Posterior papillary muscle (mitral) | PDA only (single supply) | Most vulnerable to ischemic dysfunction |
(Morgan and Mikhail's Clinical Anesthesiology, 7e; Tintinalli's Emergency Medicine)
Venous Drainage
The coronary venous system mirrors the arterial supply. Three pathways exist:
1. Coronary Sinus (~85% of venous return)
- The coronary sinus is the main venous collecting vessel, located in the posterior coronary sulcus between the left atrium and left ventricle
- Drains into the right atrium between the IVC opening and the right AV orifice
- Main tributaries feeding it:
- Great cardiac vein - runs alongside the LAD (anterior interventricular vein) then alongside the CX
- Middle cardiac vein - runs in the posterior interventricular groove alongside PDA
- Small cardiac vein - runs with the right marginal artery
- Posterior vein of the left ventricle
- Oblique vein of Marshall (small - remnant of left common cardinal vein)
2. Anterior Cardiac Veins
- 2-3 small veins draining the anterior RV surface
- Drain directly into the right atrium (do not use the coronary sinus)
3. Thebesian Veins (Smallest Cardiac Veins)
- Tiny vessels that drain directly into the cardiac chambers (mainly right side)
- A small amount of blood returns directly this way, creating a small physiological right-to-left shunt
(Morgan and Mikhail's Clinical Anesthesiology, 7e; Gray's Anatomy for Students)
Coronary Perfusion - Key Physiology Points
- Coronary perfusion is intermittent, not continuous like other organs
- The left ventricle is perfused almost entirely during diastole (systolic contraction compresses intramural vessels and nearly occludes them)
- The right ventricle is perfused during both systole and diastole (lower RV pressures)
- Coronary perfusion pressure = Aortic diastolic pressure - Left ventricular end-diastolic pressure (LVEDP)
- Three functional compartments: large conductive epicardial arteries (0.5-5 mm) → prearterioles (100-500 μm) → intramural arterioles (<100 μm, major resistance vessels)
- Capillary-to-myocyte ratio is approximately 1:1 - the heart has one of the highest capillary densities of any organ
(Barash Clinical Anesthesia, 9e)
Clinical Relevance: Coronary Stenosis Frequency
Atherosclerotic stenosis most commonly affects the first 2 cm of the vessel origin. Frequency of fatal involvement:
- Anterior interventricular (LAD) - 45-64%
- Right main coronary (RCA) - 24-46%
- Left circumflex (LCx) - 3-10%
- Left main coronary - 0-10%
- Right marginal and posterior interventricular branches - relatively immune
(P C Dikshit Textbook of Forensic Medicine and Toxicology)
This is a shared conversation. Sign in to Orris to start your own chat.