Describe in details about the interaction between the spine, pelvic, hip, knee,ankle,foot, and upper limbs in gait
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a comprehensive, detailed answer. Let me compile this.
Interactions of the Spine, Pelvis, Hip, Knee, Ankle, Foot, and Upper Limbs in Gait
The Gait Cycle: Foundation
One full gait cycle runs from heel strike (initial contact) of one foot to the next heel strike of the same foot - this is called a stride. It is divided into:
- Stance phase: ~62% of the cycle (heel strike to toe-off) - the foot is in contact with the ground
- Swing phase: ~38% of the cycle (toe-off to heel strike) - the foot is in the air
Walking is uniquely defined by always having at least one foot on the ground and including periods of double-limb support. Ground reaction forces (GRF) reach approximately 1.5x body weight during walking and 3-4x body weight during running.
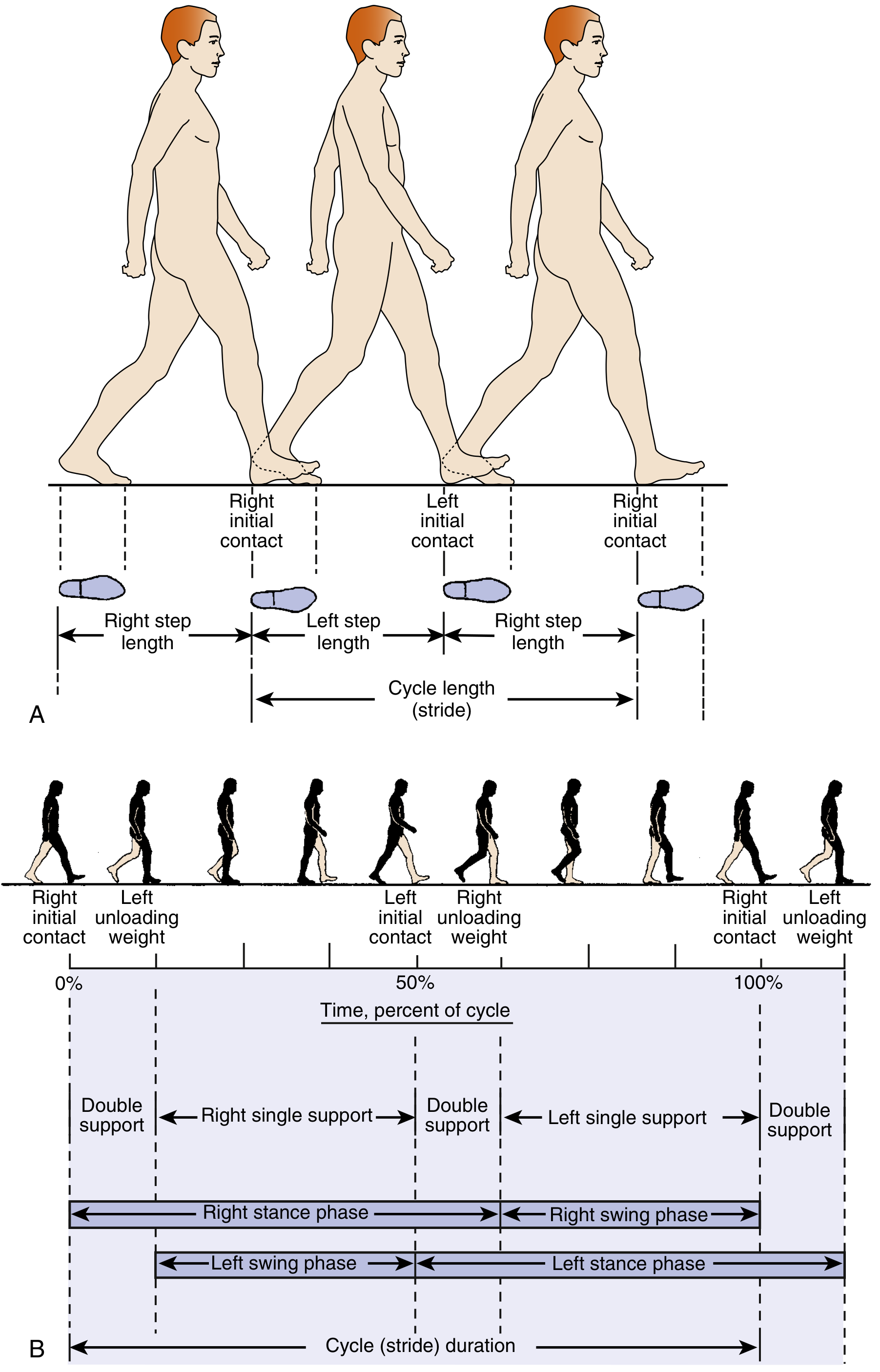
Gait cycle dimensions: stride length, step length, stance/swing phases (Miller's Review of Orthopaedics, 9th Ed.)
The Six Determinants of Gait
Six principal processes work together to minimize the vertical and lateral displacement of the center of mass, making gait energy-efficient. Three occur at the pelvis; the others involve the knee, ankle, and foot. The entire system functions like a sinusoidal curve, with the body's center of mass oscillating smoothly rather than bobbing up and down wastefully.
The trunk's center of gravity sits just anterior to T10, approximately 33 cm above the hip joints, and the whole body's center of mass lies 2 cm anterior to S2.
| Determinant | Structure | Mechanism |
|---|---|---|
| Pelvic rotation | Pelvis | External rotation at initial contact → internal rotation at preswing; reduces total vertical displacement needed for limb advancement |
| Pelvic list (lateral tilt) | Pelvis + hip abductors | Non-weight-bearing side drops 5°, reducing upward deviation of center of mass |
| Early knee flexion | Knee | 15° flexion at loading response dampens impact |
| Foot/ankle motion | Ankle/subtalar joint | Shock absorption at loading, stability at midstance, propulsion at push-off |
| Knee motion in concert with foot/ankle | Knee | Flexes at initial contact, extends at midstance to minimize unnecessary limb excursion |
| Control of pelvic lateral displacement | Hip abductors + pelvis | 5 cm lateral shift over the weight-bearing limb narrows base of support and increases stance stability |
- Miller's Review of Orthopaedics, 9th Ed.
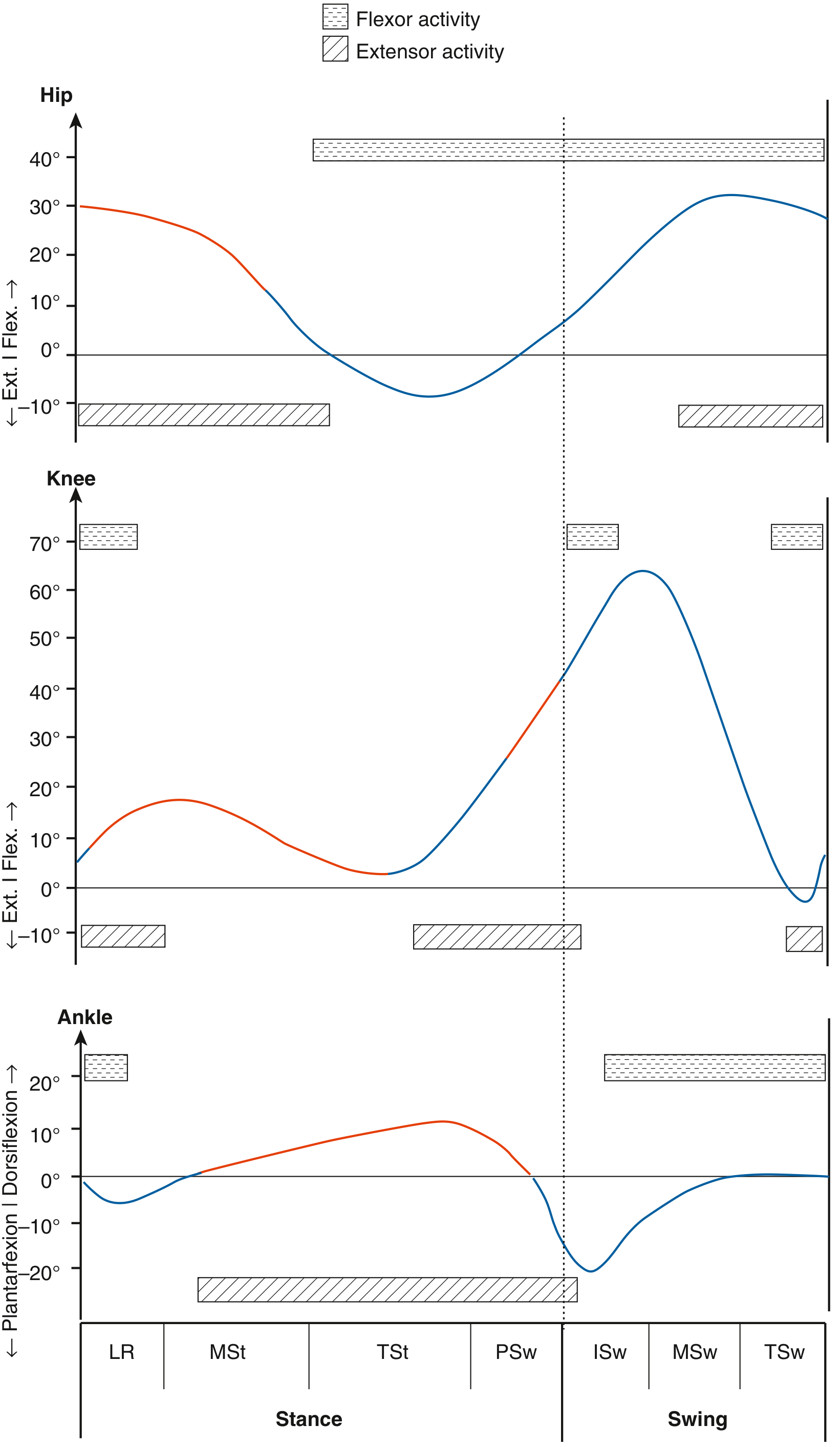
Joint angles and muscle activity (flexor vs. extensor) at the hip, knee, and ankle across the phases: LR = Loading Response, MSt = Midstance, TSt = Terminal Stance, PSw = Preswing, ISw = Initial Swing, MSw = Midswing, TSw = Terminal Swing. (Miller's Review of Orthopaedics, 9th Ed.)
1. Spine
The lumbar spine and trunk play a counterrotation role relative to the pelvis. As the pelvis rotates forward on one side during swing, the thoracic spine and upper trunk rotate in the opposite direction. This oppositional rotation:
- Reduces angular momentum of the body as a whole
- Allows smooth, energy-efficient forward progression
- Maintains the head and visual field oriented forward
The center of gravity of the head, neck, trunk, and arms accounts for 70% of total body weight. Trunk control is therefore central to overall gait stability. Any lumbar spine pathology (e.g., lumbar stenosis producing a flexed posture, or lateral trunk lean from muscle weakness) directly disturbs the sinusoidal excursion of the center of mass, increasing energy cost.
2. Pelvis
The pelvis is the kinematic bridge between the spine and lower limbs. It participates in three of the six gait determinants:
Stance phase:
- The pelvis shifts laterally over the weight-bearing limb (approximately 5 cm)
- The hip abductors (gluteus medius and minimus) contract to prevent the contralateral side from dropping excessively
- Failure of hip abductors produces the Trendelenburg gait: the pelvis drops to the contralateral side, and the person leans the trunk over the weak hip to compensate - seen as side-to-side shoulder movement while walking
Swing phase:
- At toe-off, the pelvis drops on the swing side (Trendelenburg position, controlled)
- Then performs forward rotation to advance the swing limb
Pelvic rotation (horizontal plane):
- The pelvis externally rotates from initial contact through the onset of preswing
- Then internally rotates during preswing and swing
- This symmetric rotation effectively lengthens the functional step length without requiring additional hip flexion or extension range
- Miller's Review of Orthopaedics, 9th Ed.; Rheumatology, 2-Volume Set (Elsevier, 2022)
3. Hip
The hip is a triplanar joint essential for limb advancement, weight-bearing, and energy transfer.
Stance phase:
- At initial contact (heel strike), the hip is flexed approximately 20-30°
- As stance progresses, the hip extends progressively to reach approximately 10° of extension at terminal stance/push-off
- Hip extensors (gluteus maximus, hamstrings) contract eccentrically at initial contact to control forward fall of the trunk
- Hip abductors work isometrically to stabilize the pelvis throughout single-limb stance
Swing phase:
- Hip flexors (iliopsoas, rectus femoris) contract concentrically to advance the limb forward during initial swing
- The motion trajectory of the advancing limb is refined by eccentric contraction of the hip extensors during terminal swing to decelerate the limb before initial contact
In the transverse plane:
- Hip external rotation predominates at initial contact
- The limb progressively internally rotates through midstance
Leg length inequality causes tilting of the pelvis during the gait cycle. The person may alternately flex the knee of the longer limb to clear the ground during swing, creating a characteristic dipping pattern.
- Miller's Review of Orthopaedics, 9th Ed.; Bradley and Daroff's Neurology in Clinical Practice
4. Knee
The knee undergoes two cycles of flexion and extension per gait cycle - one during stance and one during swing.
Stance phase:
- At initial contact, the knee is near full extension (approximately 5° flexion)
- As the limb is loaded, the knee flexes to approximately 15° (early stance knee flexion) - this critical flexion wave absorbs impact and prevents excessive joint loading
- The knee then returns to extension at midstance as the body's center of mass passes over the limb
- At approximately 50% of the gait cycle (contralateral foot contact), the knee begins flexing again in preparation for push-off
- This second flexion wave progresses into swing phase
Swing phase:
- The knee flexes to approximately 65° to functionally shorten the limb and allow the foot to clear the ground
- Peak knee flexion occurs in early swing
- The knee then returns to near full extension just before heel contact
The knee acts in concert with the foot and ankle to minimize unnecessary limb excursion. Quadriceps activity (eccentric) controls the loading response knee flexion wave; gastrocnemius activity bridges knee and ankle in terminal stance.
Triaxial motion of the normal knee during walking includes approximately 70° flexion-extension during swing and 20° during stance, with an additional ~10° of axial rotation.
- Firestein & Kelley's Textbook of Rheumatology; Miller's Review of Orthopaedics, 9th Ed.; Campbell's Operative Orthopaedics, 15th Ed.
5. Ankle
The ankle operates as a series of three rockers through the stance phase, each serving a distinct biomechanical role:
| Rocker | Phase | Mechanism | Muscle Activity |
|---|---|---|---|
| 1st - Heel rocker | Initial contact → foot flat | Heel contacts ground, foot pivots forward over heel | Tibialis anterior eccentric: controls rate of forefoot lowering |
| 2nd - Ankle rocker | Foot flat → midstance | Tibia advances over the fixed foot | Gastrocnemius-soleus eccentric: controls forward tibial progression |
| 3rd - Forefoot/toe rocker | Terminal stance → push-off | Heel rises, body vaults over the metatarsal heads | Gastrocnemius-soleus concentric: active push-off propulsion |
At initial contact: The foot is dorsiflexed, and the tibialis anterior contracts eccentrically. In patients with foot drop (tibialis anterior weakness), this control is lost and the foot "slaps" the ground.
At midstance: The ankle dorsiflexes to approximately 10° as the shank advances over the planted foot. The gastrocnemius-soleus complex contracts eccentrically to control this forward tibial progression.
At terminal stance/push-off: The ankle plantarflexes approximately 20° as the calf muscles contract concentrically. This generates the critical propulsive push-off that drives the body forward and upward, initiating swing phase.
In swing: The tibialis anterior contracts concentrically to dorsiflex the ankle to neutral (~10°), clearing the foot from the ground.
- Imaging Anatomy, Bones, Joints, Vessels and Nerves; Bradley and Daroff's Neurology; Miller's Review of Orthopaedics
6. Foot (Including Subtalar Joint and Arch)
The foot transitions between two critical functional states during gait: a flexible shock absorber during loading and a rigid propulsive lever at push-off.
Subtalar Joint: Locking and Unlocking Mechanism
At heel strike (subtalar everted/unlocked):
- The subtalar joint is everted, which unlocks the transverse tarsal joint (talonavicular and calcaneocuboid joints)
- This allows transverse-plane motion to absorb the weight-bearing forces
- The foot is compliant and adaptable to uneven terrain
From midstance to toe-off (subtalar inverting → locked):
- As terminal stance progresses, the subtalar joint progressively inverts
- This locks the transverse tarsal joint, converting the midfoot from flexible to rigid
- Maximum rigidity is achieved at toe-off
- The posterior tibial tendon (PTT) drives hindfoot supination to lock the joint
- The rigid lever arm allows the gastrocnemius-soleus to generate an efficient, powerful push-off
The Windlass Mechanism
As the metatarsophalangeal (MTP) joints dorsiflex at terminal stance, the plantar fascia is pulled taut (like a windlass). This:
- Elevates the longitudinal arch
- Supinates the hindfoot
- Stiffens the foot further for push-off propulsion
Insufficiency of the PTT (adult flatfoot deformity) prevents locking of the transverse tarsal joint, dramatically diminishing push-off power and causing fatigue and pain.
Hindfoot Orientation
- Heel strike: hindfoot is locked/inverted at initial contact
- Loading response: hindfoot passively everts to accommodate the ground
- In patients with cavovarus deformity, failure of hindfoot eversion redirects forces to the lateral foot, increasing risk of fifth metatarsal stress fractures, callus formation, and ankle instability
- Miller's Review of Orthopaedics, 9th Ed.; Imaging Anatomy, Bones, Joints, Vessels and Nerves
7. Upper Limbs (Arm Swing)
The arms perform reciprocal, counterrotational swing relative to the lower limbs - contralateral to the leg swing. When the right leg swings forward, the right arm swings backward and the left arm swings forward.
Biomechanical roles of arm swing:
- Angular momentum cancellation: The counterrotational arm swing reduces the rotational momentum of the pelvis and trunk, smoothing forward progression
- Energy conservation: Reciprocal arm swing reduces the muscular work required of the lower limbs by as much as 10-12%
- Balance maintenance: The lateral displacement of the arms acts as a counterbalance to lateral body shifts during single-limb stance
Arm swing is involuntary and largely automatic - it is driven by spinal and supraspinal central pattern generators coordinated with lower limb motion. It is not a passive pendular motion; there is active muscle contribution, particularly from the shoulder girdle muscles.
Clinical significance of arm swing:
- Unilateral loss of arm swing is a valuable early sign of Parkinson's disease (PD) - as the asymmetric dopaminergic degeneration first reduces arm swing on the contralateral side to the more affected limb
- Unilateral reduced arm swing may also indicate acute unilateral cerebellar lesion or hemiparesis
- Exaggerated arm swing occurs in the "military two-step" gait (marche à petit pas)
- Parkinsonian tremor of the dependent upper limb is often most visible during walking
- Bradley and Daroff's Neurology in Clinical Practice
Integrated Segment-by-Segment Summary Table
| Structure | Stance Phase | Swing Phase | Key Muscles |
|---|---|---|---|
| Spine/Trunk | Counterrotates relative to pelvis; controls center of mass | Continues counterrotation; maintains forward head orientation | Paraspinals, abdominals |
| Pelvis | Lateral shift to weight-bearing side; slight contralateral drop (5°) | Drops at toe-off, then forward rotates to advance limb | Gluteus medius/minimus (abductors) |
| Hip | Flexed 20-30° at IC → extends to 10° at terminal stance | Flexes to ~20° to advance limb; decelerates at terminal swing | Gluteus maximus (eccentric IC), iliopsoas (concentric ISw), hamstrings (eccentric TSw) |
| Knee | Near extension at IC → 15° flexion (LR) → extends at MSt → flexes at PSw | Flexes to 65° (ISw) → extends before heel strike | Quadriceps (eccentric loading), gastrocnemius, hamstrings |
| Ankle | Dorsiflexes 10° at IC; dorsiflexes progressively at MSt; plantarflexes 20° at push-off | Dorsiflexes to 10° for foot clearance | Tibialis anterior (eccentric IC, concentric swing); gastrocnemius-soleus (eccentric MSt, concentric push-off) |
| Foot/Subtalar | Heel locked/inverted at IC → unlocks (everts) during LR → progressively inverts (locks) at TSt → maximally rigid at toe-off | Dorsiflexed, cleared from ground | PTT (supination/locking), plantar fascia (windlass mechanism) |
| Upper limbs | Contralateral arm forward as leg is back; cancel pelvic rotation | Reciprocal pendular swing continuing; active shoulder girdle stabilization | Shoulder girdle, biceps, triceps |
Key Pathological Consequences of Disrupted Segmental Interactions
- Trendelenburg gait (hip abductor weakness): pelvis drops to the swing side; trunk leans to weight-bearing side to compensate - appears as lateral shoulder sway
- Antalgic gait (pain): shortened stance on the painful limb, asymmetric cycle with rapid swing on the painful side
- Foot drop (tibialis anterior weakness): no eccentric control at heel strike (foot slap), then exaggerated hip and knee flexion (steppage gait) during swing to clear the foot
- Equinus deformity (fixed ankle plantarflexion): hyperextension moment at the knee in stance; steppage gait in swing
- PTT insufficiency (adult flatfoot): failure to lock transverse tarsal joint eliminates rigid push-off, producing weak propulsion and painful flatfoot collapse
- Loss of arm swing (Parkinsonism): increased energy cost, reduced counterbalancing, and loss of a clinically important early diagnostic sign
Sources:
- Miller's Review of Orthopaedics, 9th Ed. - Gait Cycle, Determinants of Gait, Muscle Action, Pathologic Gait
- Firestein & Kelley's Textbook of Rheumatology - Kinematics of the gait cycle
- Bradley and Daroff's Neurology in Clinical Practice - Gait, Arm Swing, Stepping, Turning
- Imaging Anatomy, Bones, Joints, Vessels and Nerves - Stance and swing phases, foot mechanics
- Rheumatology, 2-Volume Set (Elsevier, 2022) - Gait analysis and clinical patterns
- Campbell's Operative Orthopaedics, 15th Ed. - Knee triaxial motion in gait
This is a shared conversation. Sign in to Orris to start your own chat.