explain rectus sheath along with anterior abdinal wall
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have comprehensive material. Let me compile the full, well-structured answer.
Anterior Abdominal Wall and Rectus Sheath
Overview
The anterior abdominal wall is a multi-layered musculoaponeurotic structure that protects abdominal viscera, supports the trunk, assists in respiration, and facilitates defecation, micturition, and parturition. It is composed of skin, superficial fascia (two layers), three flat lateral muscles with their aponeuroses, two vertical (strap) muscles, deep fascia (transversalis fascia), extraperitoneal fat, and parietal peritoneum.
Layers of the Anterior Abdominal Wall (Superficial to Deep)
| Layer | Details |
|---|---|
| Skin | Lax and mobile, except at the umbilicus |
| Camper's fascia | Superficial fatty layer; contains superficial epigastric and superficial circumflex iliac vessels; continuous with dartos of scrotum |
| Scarpa's fascia | Deep membranous layer; forms fundiform ligament of penis; fuses with fascia lata below inguinal ligament |
| Fascia innominata | Invests the external oblique; bound to inguinal ligament inferiorly |
| External oblique | Most superficial flat muscle |
| Internal oblique | Middle flat muscle |
| Transversus abdominis | Deepest flat muscle |
| Rectus abdominis (+ pyramidalis) | Vertical strap muscles enclosed in rectus sheath |
| Transversalis fascia | Deep investing fascia; lines the abdominal cavity |
| Extraperitoneal fat | Preperitoneal loose connective tissue |
| Parietal peritoneum | Innermost layer |
- Mulholland and Greenfield's Surgery, 7e
Muscles of the Anterior Abdominal Wall
1. External Abdominal Oblique
- Most superficial of the three flat muscles
- Arises from the posterior aspects of the lower 8 ribs; interdigitates with serratus anterior and latissimus dorsi at its origin
- Fibers run inferomedially ("hands in pockets" direction)
- Its aponeurosis forms the anterior rectus sheath above the arcuate line and contributes to the inguinal ligament (the inferior free edge of its aponeurosis, running from ASIS to pubic tubercle)
- The superficial inguinal ring is a triangular gap in the aponeurosis
2. Internal Abdominal Oblique
- Middle layer; fibers run superomedially (perpendicular to external oblique)
- Arises from the thoracolumbar fascia, iliac crest, and lateral inguinal ligament
- Its aponeurosis splits at the lateral border of the rectus abdominis - the anterior lamina joins the external oblique aponeurosis; the posterior lamina joins the transversus abdominis aponeurosis
- The inferior free edge loops over the spermatic cord to form the cremaster muscle
- Below the arcuate line, both laminae pass anterior to the rectus
3. Transversus Abdominis
- Deepest flat muscle; fibers run transversely
- Arises from the thoracolumbar fascia, iliac crest, lateral inguinal ligament, and inner aspect of lower 6 costal cartilages
- Its aponeurosis forms the posterior rectus sheath above the arcuate line
- Below the arcuate line, it passes anterior to the rectus
- The aponeuroses of all three muscles decussate at the midline to form the linea alba
The skin of the anterior abdominal wall is segmentally innervated by the anterior and lateral cutaneous branches of the ventral rami of the 7th-12th intercostal nerves and the 1st and 2nd lumbar nerves. - Mulholland and Greenfield's Surgery, 7e
4. Rectus Abdominis
- Paired vertical strap muscle running from the pubic symphysis/pubic crest to the 5th-7th costal cartilages
- Wider superiorly and narrows as it descends
- Intersected by 3-4 tendinous intersections (at xiphoid, umbilicus, and midway between them), which are adherent to the anterior sheath - these form the visible "six pack"
- The lateral edge is demarcated by the semilunar line (linea semilunaris)
- Blood supply: superior epigastric artery (from internal thoracic) and inferior epigastric artery (from external iliac), which anastomose just above the umbilicus; also anterior branches of intercostal arteries
- Innervation: 7th-12th intercostal nerves pierce the lateral aponeurotic sheath
5. Pyramidalis
- Small triangular muscle; may be absent
- Base on pubis; apex attached superiorly to the linea alba
- Lies anterior to the rectus abdominis, inside the rectus sheath
- Tenses the linea alba
The Rectus Sheath
The rectus sheath is an aponeurotic fibrous compartment formed by the interlacing aponeuroses of all three flat lateral muscles. It encloses the rectus abdominis, pyramidalis, superior and inferior epigastric vessels, and the terminal parts of the lower 6 intercostal nerves.
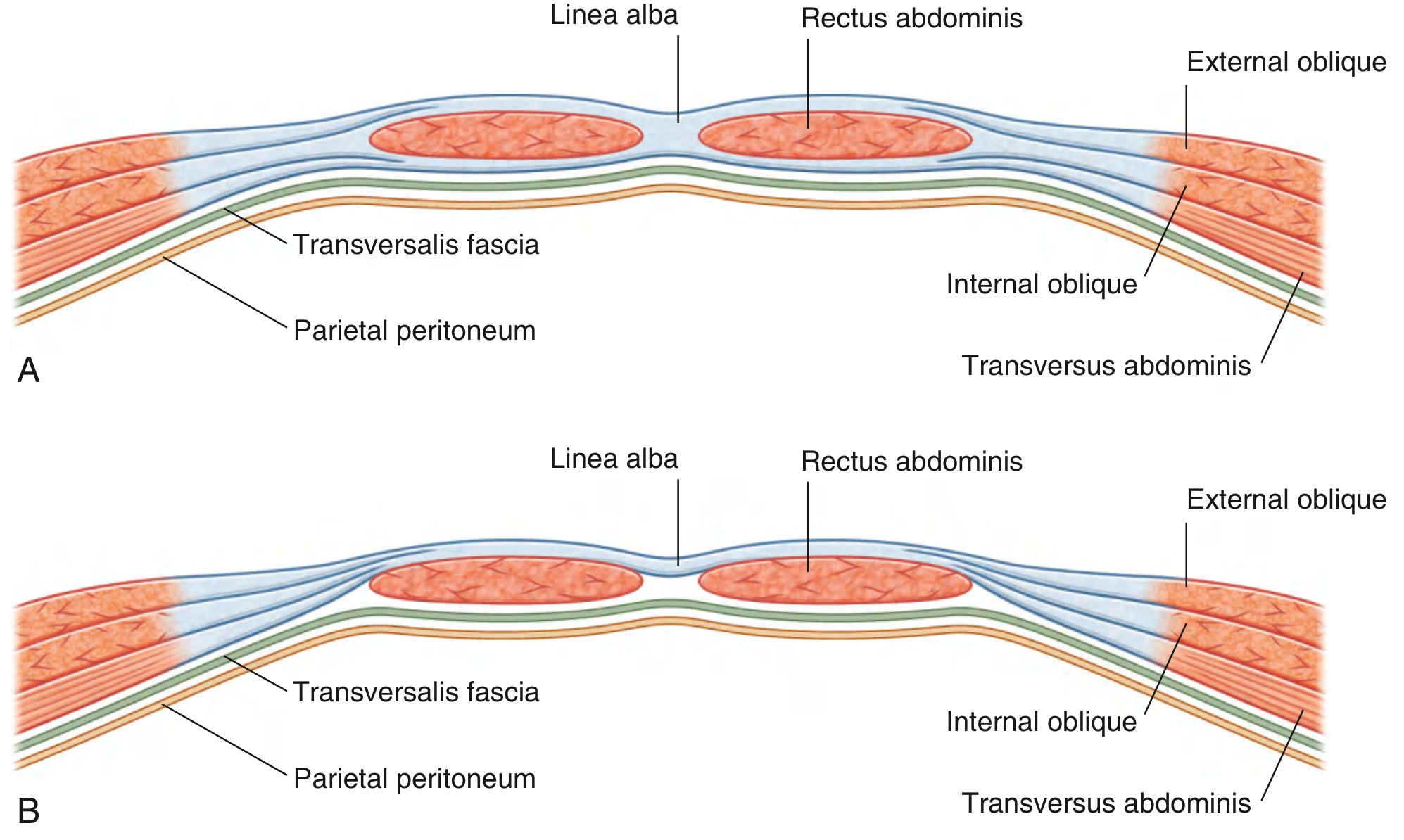
Fig. A = Above arcuate line (upper 3/4 of rectus). Fig. B = Below arcuate line (lower 1/4 of rectus)
Formation - Two Key Levels
Above the Arcuate Line (upper 3/4 of rectus abdominis)
| Wall | Composition |
|---|---|
| Anterior wall | Aponeurosis of external oblique + anterior lamina of internal oblique |
| Posterior wall | Posterior lamina of internal oblique + aponeurosis of transversus abdominis |
The rectus abdominis is completely enclosed - it has both anterior and posterior walls.
Below the Arcuate Line (lower 1/4 of rectus abdominis)
| Wall | Composition |
|---|---|
| Anterior wall | Aponeuroses of all three muscles (external oblique + both laminae of internal oblique + transversus abdominis) |
| Posterior wall | Absent |
Below the arcuate line, the posterior sheath disappears. The rectus abdominis lies directly on the transversalis fascia, which now provides the only posterior covering before the peritoneum.
The THIEME Atlas describes the two layers blending 3-5 cm below the umbilicus (at the arcuate line) to form a single, more stable sheet passing in front of the rectus. - General Anatomy and Musculoskeletal System, THIEME Atlas
The Arcuate Line (Linea Semicircularis / Douglas' Line)
- The point of transition between the two arrangements described above
- Located at the midpoint between the umbilicus and pubic symphysis (approximately 3-5 cm below the umbilicus)
- Marks the inferior free edge of the posterior rectus sheath
- Below this line, the inferior epigastric vessels enter the rectus sheath
Contents of the Rectus Sheath
- Rectus abdominis muscle
- Pyramidalis muscle (when present)
- Superior epigastric artery and veins
- Inferior epigastric artery and veins
- Anterior rami of thoracoabdominal nerves (T7-T12)
- Lymphatics
Important Surface Landmarks
- Linea alba: Midline confluence/decussation of aponeuroses of both sides; extends from xiphoid to pubic symphysis; a relatively avascular area used for midline surgical incisions
- Linea semilunaris (semilunar line): Curved line on the surface marking the lateral edge of rectus abdominis; site where the aponeuroses of lateral muscles begin to form the sheath
- Linea semicircularis (arcuate line): Inferior curved free edge of the posterior rectus sheath
Neurovascular Supply Summary
| Structure | Supply |
|---|---|
| Arterial | Superior epigastric (from internal thoracic), inferior epigastric (from external iliac), lower 5-6 intercostal arteries, superficial epigastric and superficial circumflex iliac (from femoral) |
| Venous | Parallels arteries; drains to internal thoracic, external iliac, and azygos systems |
| Lymphatic | Above umbilicus → axillary nodes; below umbilicus → superficial inguinal nodes |
| Nerve | Anterior rami T7-T12 (thoracoabdominal nerves) + L1 (iliohypogastric, ilioinguinal) |
Clinical Relevance
- Rectus sheath hematoma: Rupture of inferior epigastric artery (e.g., after coughing, anticoagulation, trauma) causes blood to collect within the sheath. Below the arcuate line, blood can spread freely since there is no posterior sheath containing it.
- Rectus sheath block: Regional anesthesia technique - local anesthetic injected between rectus abdominis and posterior sheath at the level above the arcuate line; used for midline incision analgesia.
- Midline (linea alba) incision: Standard surgical access - avascular, easily opened and closed, but weaker healing (higher dehiscence risk).
- Posterior rectus sheath release (Transversus abdominis release - TAR): A hernia repair technique that utilizes the plane behind the rectus sheath.
- Pfannenstiel incision: Transverse incision through the rectus sheath for gynecologic and urologic procedures; the anterior sheath is separated from the underlying rectus muscles using the tendinous intersections as landmarks.
Sources: Gray's Anatomy for Students | Mulholland and Greenfield's Surgery, 7e | General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy | Berek & Novak's Gynecology
explain rectus sheath along with anterior abdinal wall+ applied aspect subject anatomy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
I now have all the material needed for a thorough, exam-ready anatomy answer. Let me compose the full response.
Anterior Abdominal Wall and Rectus Sheath - Complete Anatomy with Applied Aspects
1. Overview
The anterior abdominal wall is a multi-layered musculoaponeurotic structure bounded superiorly by the costal margins and xiphoid, inferiorly by the inguinal ligaments and pubic symphysis, and laterally by the mid-axillary lines. Its functions include:
- Protection of abdominal viscera
- Assistance with respiration, defecation, micturition, parturition, and vomiting (by raising intra-abdominal pressure)
- Postural support and trunk flexion/rotation
2. Layers of the Anterior Abdominal Wall (Superficial to Deep)
| # | Layer | Key Details |
|---|---|---|
| 1 | Skin | Lax and mobile; adherent only at the umbilicus |
| 2 | Camper's fascia | Superficial fatty layer (panniculus adiposus); contains superficial epigastric and superficial circumflex iliac vessels; continuous with dartos of scrotum |
| 3 | Scarpa's fascia | Deep membranous layer; forms fundiform ligament of penis; fuses with fascia lata below inguinal ligament |
| 4 | Fascia innominata | Invests the external oblique; fuses to inguinal ligament inferiorly |
| 5 | Muscles | Three flat (external oblique, internal oblique, transversus abdominis) + two vertical (rectus abdominis, pyramidalis) |
| 6 | Transversalis fascia | Deep investing fascia lining the abdominal cavity; forms deep ring of inguinal canal |
| 7 | Extraperitoneal fat | Loose connective tissue containing variable fat |
| 8 | Parietal peritoneum | Innermost layer |
- Mulholland and Greenfield's Surgery, 7e
3. Muscles of the Anterior Abdominal Wall
Muscle Summary Table
| Muscle | Origin | Insertion | Nerve | Action |
|---|---|---|---|---|
| External oblique | Outer surface of ribs V-XII | Iliac crest, linea alba | T7-T12 | Compress abdomen; flex trunk; rotate trunk to opposite side |
| Internal oblique | Thoracolumbar fascia, iliac crest, lateral inguinal ligament | Lower 3-4 ribs, linea alba, pubic crest | T7-T12, L1 | Compress abdomen; flex trunk; rotate to same side |
| Transversus abdominis | Thoracolumbar fascia, medial iliac crest, lateral inguinal ligament, costal cartilages VII-XII | Linea alba, pubic crest | T7-T12, L1 | Compress abdominal contents |
| Rectus abdominis | Pubic crest, pubic tubercle, pubic symphysis | Costal cartilages of V-VII, xiphoid | T7-T12 | Flex vertebral column, compress abdomen, tense abdominal wall |
| Pyramidalis | Front of pubis, pubic symphysis | Linea alba | T12 | Tenses the linea alba |
- Gray's Anatomy for Students
3.1 External Abdominal Oblique
- Most superficial flat muscle; arises from the outer surfaces of the lower 8 ribs (V-XII); interdigitates with serratus anterior and latissimus dorsi at its origin
- Fiber direction: inferomedially ("hands in pockets")
- Aponeurosis contributes to the anterior rectus sheath and forms the inguinal ligament (inferior folded free edge from ASIS to pubic tubercle)
- The medial fibers of the aponeurosis split to form the superficial (external) inguinal ring
- The lacunar ligament is a fan-shaped extension of the inguinal ligament to the pectineal line; it blends laterally with Cooper's (pectineal) ligament
3.2 Internal Abdominal Oblique
- Middle layer; fiber direction is superomedially (perpendicular to external oblique)
- Arises from thoracolumbar fascia, iliac crest, and lateral inguinal ligament
- Its aponeurosis splits (above the umbilicus) into anterior and posterior laminae to envelop the rectus abdominis - anterior lamina joins external oblique; posterior lamina joins transversus abdominis
- Below the umbilicus, aponeurosis does not split; runs entirely anterior to rectus
- Lower fibers arch over spermatic cord; some join transversus to form cremaster muscle
3.3 Transversus Abdominis
- Deepest flat muscle; fibers run transversely
- Arises from thoracolumbar fascia, iliac crest, lateral inguinal ligament, and costal cartilages VII-XII
- Aponeurosis forms the posterior rectus sheath above the arcuate line
- Below the arcuate line, passes entirely anterior to rectus
- The aponeurosis of all three muscles decussates at the midline to form the linea alba
3.4 Rectus Abdominis
- Long flat vertical muscle; extends the full length of the anterior abdominal wall
- Origin: pubic crest, pubic tubercle, pubic symphysis
- Insertion: costal cartilages of ribs V-VII, xiphoid process
- Wider superiorly, narrows as it descends to the pubis
- Has 3-4 tendinous intersections (at level of xiphoid, umbilicus, and midway between them) - adherent to the anterior sheath only (not the posterior sheath), hence pus/blood does not track upward across them but can spread freely below the arcuate line
- Lateral edge demarcated by a surface depression - the linea semilunaris (semilunar line)
- Blood supply: superior epigastric artery (from internal thoracic) + inferior epigastric artery (from external iliac); these two vessels anastomose just above the umbilicus within the rectus sheath
- Innervation: anterior rami of T7-T12 intercostal nerves, piercing the lateral aponeurotic sheath
3.5 Pyramidalis
- Small triangular muscle; may be absent in ~20% of individuals
- Base on pubis; apex attaches superiorly to linea alba
- Lies anterior to rectus abdominis, within the rectus sheath
- Tenses the linea alba; supplied by T12
4. The Rectus Sheath
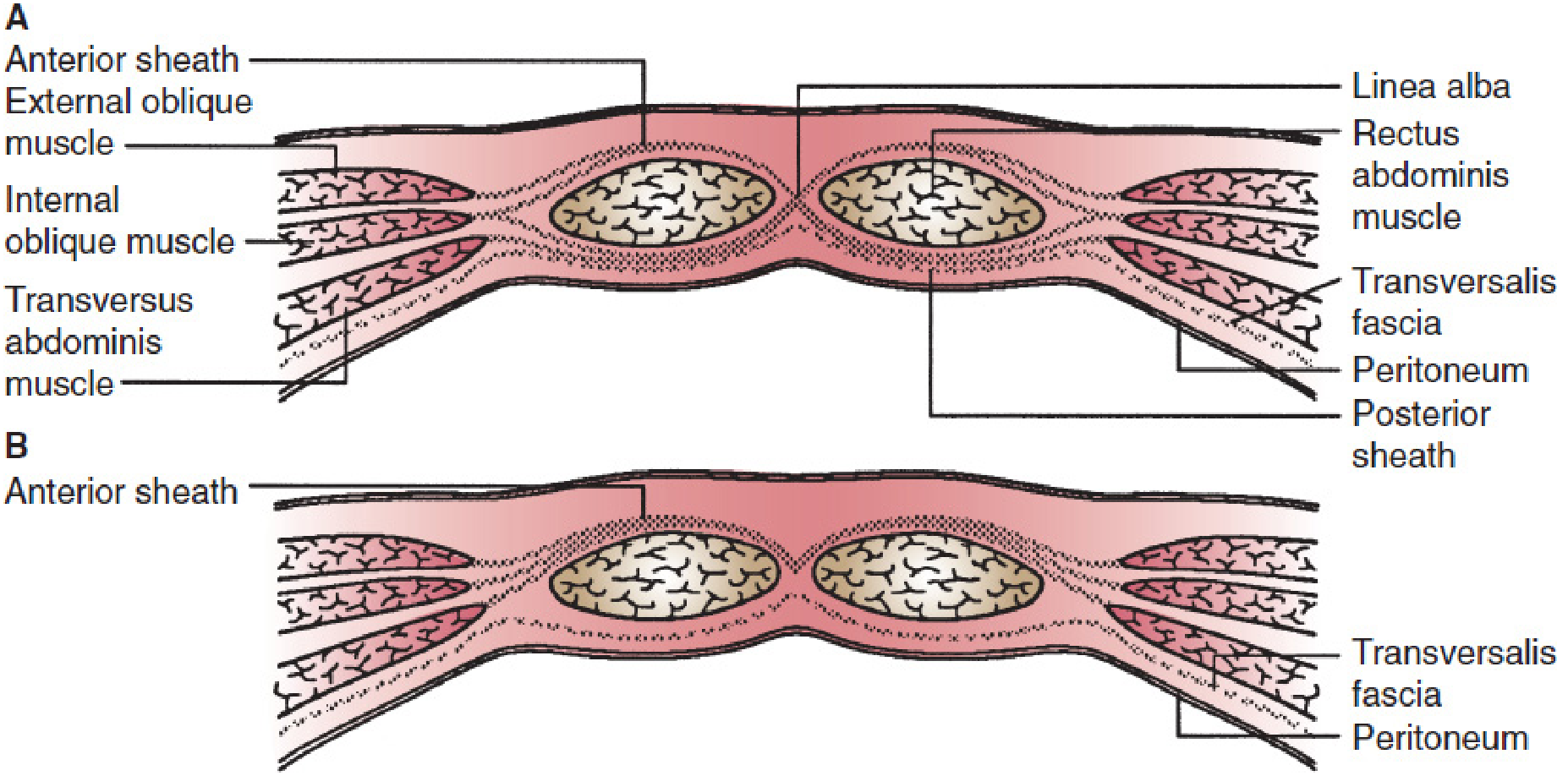
The rectus sheath is an aponeurotic fibrous compartment formed by the unique layering of aponeuroses of the three flat lateral muscles. It encloses the rectus abdominis, pyramidalis, superior and inferior epigastric vessels, and the terminal parts of T7-T12 intercostal nerves and lymphatics.
Fig. A = Above arcuate line (upper 3/4 of rectus) - both anterior AND posterior walls present. Fig. B = Below arcuate line (lower 1/4) - anterior wall only, no posterior wall.
A: Above arcuate line showing anterior and posterior sheath with all three muscle layers. B: Below arcuate line - only anterior sheath present; rectus lies directly on transversalis fascia.
4.1 Formation of the Rectus Sheath at Two Key Levels
ABOVE the Arcuate Line (upper 3/4 of rectus abdominis)
| Wall | Composition |
|---|---|
| Anterior wall | Aponeurosis of external oblique + anterior lamina of internal oblique aponeurosis |
| Posterior wall | Posterior lamina of internal oblique aponeurosis + aponeurosis of transversus abdominis |
- The rectus is completely enclosed on all sides
BELOW the Arcuate Line (lower 1/4 of rectus abdominis)
| Wall | Composition |
|---|---|
| Anterior wall | Aponeuroses of all three muscles (external oblique + both laminae of internal oblique + transversus abdominis) |
| Posterior wall | ABSENT |
- The rectus abdominis lies directly on the transversalis fascia
- Only transversalis fascia (then extraperitoneal fat and peritoneum) posteriorly
4.2 The Arcuate Line (Linea Semicircularis / Douglas' Line)
- Curved free lower border of the posterior rectus sheath
- Located approximately midway between the umbilicus and pubic symphysis (about 3-5 cm below the umbilicus)
- Marks where all aponeuroses swing to the anterior aspect of the rectus
- Below the arcuate line, the inferior epigastric vessels enter and run within the rectus sheath
4.3 Contents of the Rectus Sheath
- Rectus abdominis muscle
- Pyramidalis muscle
- Superior epigastric artery and veins
- Inferior epigastric artery and veins
- Anterior rami of T7-T12 (thoracoabdominal nerves)
- Lymphatics
4.4 Surface Landmarks
| Landmark | Description |
|---|---|
| Linea alba | Midline confluence of all aponeuroses from both sides; xiphoid to pubic symphysis; relatively avascular; wider above umbilicus, narrow below |
| Linea semilunaris | Curved surface marking of the lateral border of rectus abdominis; where flat muscle aponeuroses begin to form the sheath |
| Linea semicircularis (Arcuate line) | Inferior free edge of posterior rectus sheath; Douglas' line |
| Tendinous intersections | 3-4 fibrous bands crossing the rectus; adherent to anterior wall only |
| Umbilicus | At the level of the L3/L4 disc; scarred remnant of umbilical cord |
5. Neurovascular Supply of the Anterior Abdominal Wall
Arterial Supply
- Deep vessels: Superior epigastric (from internal thoracic), inferior epigastric (from external iliac artery), lower 5-6 intercostal and subcostal arteries (from aorta), musculophrenic artery
- Superficial vessels: Superficial epigastric and superficial circumflex iliac (both tributaries of the femoral artery)
- Note: Superior and inferior epigastric arteries anastomose inside the rectus sheath just above the umbilicus
Venous Drainage
- Mirrors the arterial supply; drains to internal thoracic, external iliac, and azygos/hemiazygos systems
- The superficial veins form an important portosystemic anastomosis at the umbilicus (thoracoepigastric vein connects superior and inferior epigastric systems)
Lymphatic Drainage
- Above umbilicus → anterior axillary (pectoral) lymph nodes
- Below umbilicus → superficial inguinal lymph nodes
Nerve Supply
- T7-T11: Intercostal nerves (run between internal oblique and transversus)
- T12: Subcostal nerve
- L1: Iliohypogastric and ilioinguinal nerves
- Dermatomes: T6 = xiphoid level, T10 = umbilicus level, L1 = inguinal/suprapubic region
6. Applied / Clinical Anatomy
6.1 Rectus Sheath Hematoma
- Caused by disruption of the inferior epigastric artery or its branches, most commonly at or near the arcuate line, where the artery and its branches are relatively fixed and vulnerable to shearing forces
- Risk factors: trauma (including laparoscopic trocar placement), vigorous rectus contraction (coughing, sneezing, exercise), anticoagulation therapy, chronic pulmonary disease
- Above the arcuate line: Blood is contained within the sheath (bounded by posterior sheath), forms a localized hematoma
- Below the arcuate line: No posterior sheath, so blood can spread across the midline and bilaterally into the space of Retzius - hematoma can become very large
- Clinical features: Acute abdominal pain + palpable abdominal wall mass; can mimic appendicitis (right-sided)
- Fothergill's sign: A palpable mass that does NOT change position or disappear when the rectus is contracted (as it lies within the sheath itself) - distinguishes it from intraperitoneal pathology
- Diagnosis: Ultrasound or CT scan with IV contrast (gold standard)
- Management:
- Stable, small hematoma: conservative (rest, compression, reversal of anticoagulation)
- Enlarging hematoma: hospitalization, serial hemoglobin, transfusion if needed
- Haemodynamic shock: angiographic embolization (first line), surgical ligation if embolization fails
- Schwartz's Principles of Surgery, 11e
6.2 Inguinal Canal and Inguinal Hernia
- The inguinal canal is a passage through the anterior abdominal wall created by the descent of the testis during development; it runs parallel and just above the inguinal ligament
- Deep (internal) inguinal ring: Defect in transversalis fascia, lateral to inferior epigastric vessels
- Superficial (external) inguinal ring: Triangular gap in external oblique aponeurosis, above and medial to pubic tubercle
- Indirect inguinal hernia: Exits through the deep ring lateral to the inferior epigastric vessels, passes through the full length of the inguinal canal; enters through a patent processus vaginalis - the most common hernia, more common in males
- Direct inguinal hernia: Bulges directly through the posterior wall of the inguinal canal (Hesselbach's triangle - bounded by inferior epigastric vessels laterally, inguinal ligament inferiorly, rectus sheath medially); medial to inferior epigastric vessels; never descends into the scrotum; less prone to strangulation
- The groin is described as the weakest area in the anterior abdominal wall - Gray's Anatomy for Students
6.3 Diastasis Recti
- Abnormal separation of the two rectus abdominis muscles with laxity/stretching of the linea alba at the midline
- Not a true hernia - midline fascia is intact (no hernial sac); incarceration and strangulation do NOT occur
- Causes: Conditions that raise intra-abdominal pressure (obesity, pregnancy) or weaken the abdominal wall (connective tissue disorders, prior surgery)
- Presentation: Fusiform midline bulge, worsens with rectus contraction or Valsalva
- Diagnosis: Clinical exam; ultrasound or CT if needed
- Management: Usually conservative (weight loss, exercise); surgery (plication of rectus sheath, open or laparoscopic) only for significant functional disability or cosmesis
- Schwartz's Principles of Surgery, 11e
6.4 Umbilical and Paraumbilical Hernias
- Umbilical ring is a potential weak spot in the linea alba
- Congenital umbilical hernia: Defect in umbilical ring; most close spontaneously by age 3-4 years
- Paraumbilical hernia (adults): Herniates through a defect just above or below the umbilicus in the linea alba; more common in multiparous, obese women
6.5 Epigastric Hernia
- Herniates through a defect in the linea alba between the xiphoid and umbilicus
- Usually contains extraperitoneal fat (pre-peritoneal fat)
- May be asymptomatic or cause epigastric pain
6.6 Surgical Incisions - Applied Anatomy
| Incision | Layer-by-Layer | Notes |
|---|---|---|
| Midline (linea alba) | Skin → Scarpa's fascia → linea alba → extraperitoneal fat → peritoneum | Avascular; quick; good access; higher dehiscence rate |
| Paramedian | Skin → anterior rectus sheath → retract/split rectus laterally → posterior sheath → peritoneum | More secure closure; better blood supply to wound |
| Pfannenstiel (transverse suprapubic) | Skin → anterior rectus sheath (transversely) → separate sheath off rectus muscle → midline incision of rectus/peritoneum | Used in gynecological/urological surgery; cosmetically superior; anterior sheath separated using tendinous inscriptions as landmarks |
| Kocher (subcostal) | Parallel to costal margin; through all layers | Used for cholecystectomy, splenectomy |
6.7 Rectus Sheath Block (Regional Anesthesia)
- An ultrasound-guided regional block targeting anterior cutaneous branches of T7-T12 as they pierce the posterior wall of the rectus sheath before entering the muscle
- Local anesthetic is deposited deep to the rectus abdominis (between rectus and posterior sheath) bilaterally
- Produces elliptical midline analgesia from xiphoid to symphysis pubis
- Indications: Umbilical hernia repair; analgesia after midline laparotomy; alternative to thoracic epidural
- Note: provides somatic (wall) analgesia only - no visceral coverage
- The needle is inserted from lateral to medial; local anesthetic hydrodissects the rectus sheath from the underlying transversalis fascia
- Morgan and Mikhail's Clinical Anesthesiology, 7e
6.8 Posterior Rectus Sheath Release (TAR Technique)
- Used in complex ventral hernia repair
- The posterior rectus sheath is incised and elevated off the transversalis fascia, creating a large retromuscular space for mesh placement
- Exploits the anatomical plane between posterior sheath and transversalis fascia
6.9 Portosystemic Anastomosis at the Umbilicus (Caput Medusae)
- The umbilical vein remnant (ligamentum teres) connects the portal system with the superficial epigastric veins at the umbilicus
- In portal hypertension, these veins dilate and become visible on the abdominal surface as caput medusae (dilated veins radiating from the umbilicus)
6.10 Referred Pain Dermatomal Patterns
- Visceral pain from the appendix (T10) is initially referred to the periumbilical region before localizing to the right iliac fossa
- T10 dermatome = umbilicus level - clinically important for dermatomal testing and segmental nerve injury assessment
Sources: Gray's Anatomy for Students | Mulholland and Greenfield's Surgery, 7e | Schwartz's Principles of Surgery, 11e | Morgan and Mikhail's Clinical Anesthesiology, 7e | General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy
This is a shared conversation. Sign in to Orris to start your own chat.