Ecg changes in mi
Reading File
Finding Sources
Searching Images
ECG changes in myocardial infarction ST elevation T wave Q wave
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of ECG changes in myocardial infarction (MI):
ECG Changes in Myocardial Infarction
Pathophysiological Basis
Three major membrane abnormalities underlie the ECG changes in acute MI (Ganong's Review of Medical Physiology, Table 29-3):
| Defect in Infarcted Cells | Current Flow | ECG Change (leads over infarct) |
|---|---|---|
| Rapid repolarization (accelerated K⁺ channel opening) | Out of infarct | ST segment elevation |
| Decreased resting membrane potential (loss of intracellular K⁺) | Into infarct | TQ depression → manifests as ST elevation |
| Delayed depolarization | Out of infarct | ST segment elevation |
Ischemia lowers resting membrane potential and shortens action potential duration, creating a voltage gradient between normal and ischemic zones — these "currents of injury" appear on the surface ECG as ST deviation.
Chronological Evolution of ECG Changes
1. Hyperacute Phase (Minutes — First Hour)
- Tall, peaked (hyperacute) T waves — earliest change; broad-based, asymmetric
- Represents the very first electrical response to acute transmural ischemia before ST elevation develops
2. Acute Phase (Hours to Days) — STEMI
- ST segment elevation in leads overlying the infarct
- Transmural ischemia shifts the ST vector toward the epicardial/outer layers
- Often convex ("tombstone") or coved morphology
- Reciprocal ST depression in leads on the opposite side of the heart
- Q waves begin forming as myocardial necrosis sets in — electrically silent dead tissue causes loss of R-wave forces
3. Evolving Phase (Days to Weeks)
- T-wave inversions develop in the same leads as ST elevation (as ST returns toward baseline)
- Pathological Q waves deepen and become permanent
- R-wave loss / poor R-wave progression in precordial leads
4. Chronic Phase (Weeks to Months)
- Persistent Q waves (marker of old infarct)
- ST segment typically normalizes
- T waves may remain inverted or gradually normalize
- Persistent ST elevation (>4–6 weeks) suggests ventricular aneurysm
Current of Injury Diagram

Panel A: Subendocardial ischemia → ST vector directed inward → ST depression in overlying leads. Panel B: Transmural/epicardial ischemia → ST vector directed outward → ST elevation in overlying leads. — Harrison's Principles of Internal Medicine 22E, Fig. 247-11
STEMI vs NSTEMI
| Feature | STEMI | NSTEMI / Unstable Angina |
|---|---|---|
| ST changes | Elevation ≥1 mm (limb leads) or ≥2 mm (precordial) | Depression or no change |
| Q waves | Often develop | Usually absent |
| T waves | Hyperacute → inversion | May show inversion |
| Troponin | Elevated | Elevated (NSTEMI) / normal (UA) |
| Reperfusion urgency | Immediate (PCI/thrombolysis) | Urgent but tiered |
Localization by Lead Distribution
| Territory | Culprit Artery | Leads with ST Elevation | Reciprocal Changes |
|---|---|---|---|
| Anterior | LAD (proximal) | V1–V4 | II, III, aVF |
| Anterolateral | LAD / LCx | V3–V6, I, aVL | II, III, aVF |
| Lateral | LCx | I, aVL, V5–V6 | II, III, aVF |
| Inferior | RCA (80%) / LCx (20%) | II, III, aVF | I, aVL |
| Posterior | RCA / LCx | Tall R in V1–V2 (reciprocal) | ST↑ in V7–V9 |
| Right ventricular | Proximal RCA | V1, V4R | — |
| Septal | LAD (septal branches) | V1–V2 | — |
Key Specific ECG Patterns
- Wellens T-wave sign: Deep, symmetric T-wave inversions in V1–V4 (± I, aVL) → critical LAD stenosis, high risk for anterior STEMI
- de Winter T-waves: Upsloping ST depression with tall, symmetric T waves in precordial leads → LAD occlusion equivalent (no classic ST elevation)
- Posterior MI: Tall broad R waves and ST depression in V1–V2 (mirror image of posterior ST elevation); confirmed with posterior leads V7–V9
- RV MI: ST elevation in V4R (right-sided chest lead); seen with inferior STEMI; important as nitrates are contraindicated
- Bundle branch block: New LBBB with chest pain = STEMI equivalent. Sgarbossa criteria help identify STEMI with LBBB: (1) concordant ST elevation ≥1 mm, (2) concordant ST depression ≥1 mm in V1–V3, (3) discordant ST elevation ≥5 mm
Example ECG: Inferior STEMI
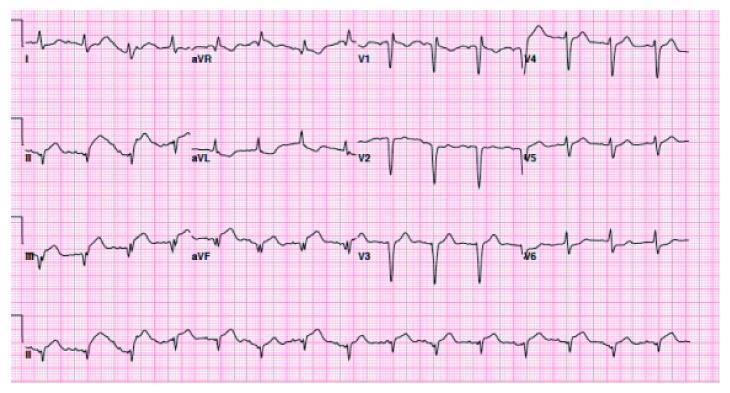
ST elevation in inferior leads (II, III, aVF) with reciprocal ST depression in aVL; Q waves visible in inferior leads consistent with evolving/established infarction.
Important Limitations
- A normal ECG does not exclude MI — serial ECGs are essential
- LBBB, ventricular pacing, and WPW may mask ischemic changes
- ST elevation mimics: pericarditis, early repolarization, Brugada pattern, takotsubo syndrome, hyperkalemia, myocarditis
- Q wave mimics: LVH, LBBB, hypertrophic cardiomyopathy, WPW, myocarditis
Sources: Harrison's Principles of Internal Medicine, 22E (Chap. 247); Ganong's Review of Medical Physiology, 26E (Chap. 29)
This is a shared conversation. Sign in to Orris to start your own chat.