Fever
Reading File
Asking for Preferences
All
Finding Sources
Searching PubMed
fever pathophysiology management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compose the full response.
Fever: A Comprehensive Overview
1. Definition and Normal Temperature
Fever is an abnormal elevation of core body temperature above the usual range of normal. A universally accepted cutoff does not exist, but common thresholds are:
- Adults: ≥38.3°C (≥101°F) is the most widely used clinical threshold
- Infants: ≥38°C (100.4°F) warrants concern; in neonates <2-3 months, hypothermia (<36°C / 96.8°F) is equally alarming
- Hyperpyrexia: >41°C (105.8°F) - associated with increased risk of serious bacterial infection and tissue damage
The usual range of normal is approximately 36-38°C (97-100.4°F). Temperature measurement matters: axillary readings are ~0.6°C lower than oral, which is ~0.6°C lower than rectal; infrared thermometers have variable reliability.
2. Pathophysiology
The Hypothalamic Set-Point Mechanism
Fever is not simply uncontrolled heat - it is a regulated increase in the hypothalamic thermostat set-point. Normal thermoregulation involves the anterior hypothalamic-preoptic area, which compares core temperature to the set-point and activates either heat-loss or heat-gain mechanisms accordingly.
The cascade:
- Exogenous pyrogens (bacteria, bacterial endotoxins/LPS, viruses, fungi, toxins, tumor antigens) enter the body
- They are phagocytized by leukocytes, tissue macrophages, and large granular killer lymphocytes
- These cells digest the bacterial products and release cytokines (endogenous pyrogens):
- Interleukin-1 (IL-1) - the most important; also called leukocyte pyrogen or endogenous pyrogen; can raise temperature within 8-10 minutes; as little as 1/10,000,000 gram of bacterial LPS (acting with leukocytes) can trigger it
- Interleukin-6 (IL-6)
- Tumor necrosis factor (TNF)
- These cytokines act on the anterior hypothalamus → stimulate local prostaglandin E2 (PGE2) synthesis via cyclooxygenase (COX)
- PGE2 raises the hypothalamic set-point temperature
Costanzo Physiology, 7th Ed., p. 184; Guyton & Hall, Medical Physiology, p. 900
Chills and the "Crisis" (Flush)
When the set-point suddenly rises (e.g., to 39.4°C / 103°F):
- Core temp is now below the new set-point
- The body activates heat-conservation mechanisms: cutaneous vasoconstriction (cold skin), shivering (heat production)
- The patient feels intensely cold ("chills" or "rigors") even though body temperature may already be elevated
When the causative factor is removed (or antipyretics given):
- The set-point drops back to normal
- Core temp is now above the set-point
- The body activates heat-loss mechanisms: vasodilation (flushed skin) and sweating
- This is the "crisis" or "flush" - historically a good prognostic sign
Guyton & Hall, Medical Physiology, p. 901
How Antipyretics Work
Aspirin, acetaminophen, ibuprofen, and other NSAIDs inhibit cyclooxygenase (COX), blocking prostaglandin synthesis. This interrupts the pyrogen pathway and lowers the set-point back toward normal. When fever is treated, the hypothalamus now "reads" core temperature as too high relative to the (now-lowered) set-point and initiates heat dissipation (vasodilation and sweating).
Costanzo Physiology, 7th Ed., p. 184
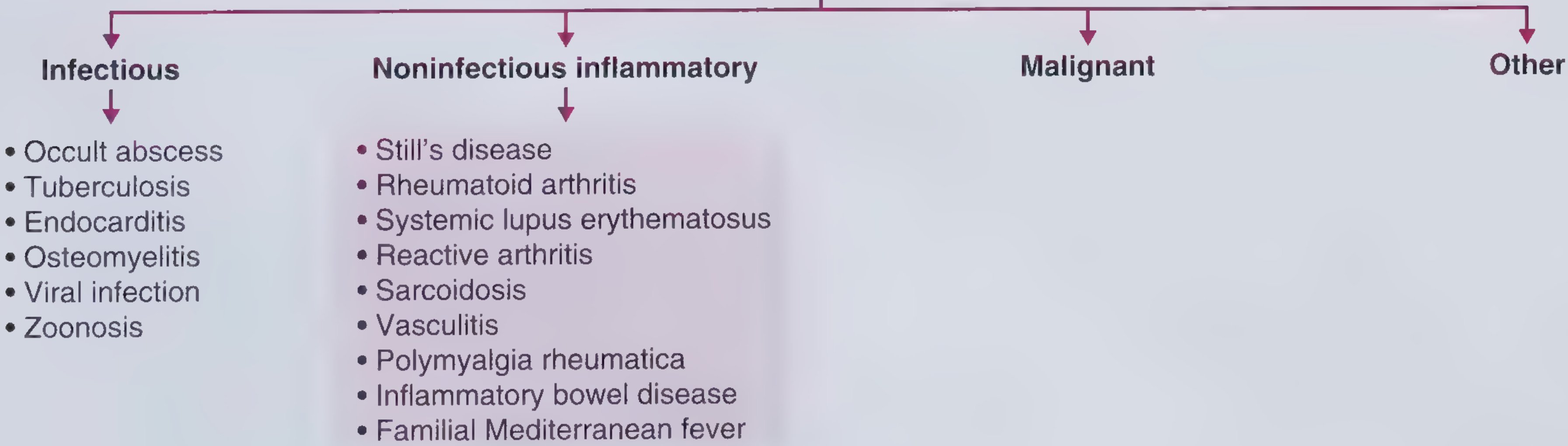
3. Causes and Differential Diagnosis
Fever is caused by a vast range of conditions. A practical framework organizes causes as:
Infectious (Most Common)
- Bacterial: pneumonia, UTI, meningitis, septicemia, endocarditis, osteomyelitis, intra-abdominal abscess, tuberculosis, typhoid
- Viral: influenza, COVID-19, EBV, CMV, HIV, hepatitis viruses, dengue
- Parasitic: malaria, leishmaniasis, toxoplasmosis
- Fungal: candidiasis, histoplasmosis, cryptococcosis (especially in immunocompromised)
- Other: Lyme disease, rickettsial infections, zoonoses
Inflammatory / Autoimmune
- Rheumatoid arthritis, SLE, Adult-onset Still's disease (AOSD)
- Vasculitides (giant cell arteritis, polyarteritis nodosa)
- Polymyalgia rheumatica
- Inflammatory bowel disease (Crohn's, UC)
- Sarcoidosis, Reactive arthritis, Familial Mediterranean fever (FMF)
Malignant
- Lymphoma (both Hodgkin's and non-Hodgkin's), leukemia
- Solid tumors (renal cell carcinoma - "internist's tumor," hepatocellular carcinoma)
- Hemophagocytic lymphohistiocytosis (HLH)
Drug Fever
- Many drugs can cause fever through hypersensitivity mechanisms
- Common offenders: beta-lactam antibiotics, sulfonamides, phenytoin, allopurinol, procainamide, quinidine
Other / Miscellaneous
- DVT/pulmonary embolism
- Transfusion reactions
- Factitious fever
- Brain lesions (hypothalamic)
- Endocrine: thyroid storm, adrenal insufficiency
- Postoperative fever (see below)
Postoperative Fever - The "Five Ws"
A classic surgical mnemonic:
| W | Cause | Typical Timing |
|---|---|---|
| Wind | Atelectasis / pneumonia | <24 h / 2-7 d |
| Water | UTI | 2-5 days |
| Wound | Wound infection | 5+ days |
| Walking | DVT / PE | 5+ days |
| Wonder drugs | Drug fever / C. diff colitis | Any time |
Tintinalli's Emergency Medicine, p. 597; Bailey & Love's Surgery, p. 346
4. Clinical Evaluation and Workup
History
Key elements:
- Onset, duration, pattern - sustained, remittent, intermittent, relapsing
- Associated symptoms - localizing symptoms (cough, dysuria, headache, rash, arthralgia)
- Travel history - malaria, typhoid, leishmaniasis, arboviral infections
- Animal / occupational exposure - zoonoses
- Immunosuppression - medications, HIV, transplant status
- Social history - IV drug use (endocarditis risk), sexual history
For suspected non-infectious inflammatory causes, ask specifically about: morning stiffness >1 hour, ocular symptoms, skin rash, bowel changes, family history of periodic fever syndromes, response to glucocorticoids.
Physical Examination
- Vital signs (temperature pattern, heart rate, blood pressure)
- Lymphadenopathy, hepatosplenomegaly
- Skin: rashes, petechiae, Janeway lesions, Osler nodes
- Joints: swelling, warmth, range of motion
- Fundoscopy, ENT, dental (occult abscesses)
- Heart: new murmurs (endocarditis)
Initial Investigations
- CBC with differential - leukocytosis (bacterial), lymphocytosis (viral), pancytopenia (HLH, marrow involvement, SLE)
- CRP, ESR, procalcitonin - infection vs. inflammation markers
- Blood cultures (x2-3 sets before antibiotics)
- Urinalysis + urine culture
- Chest X-ray
- LFTs, renal function, electrolytes
- HIV serology if indicated
- Specific serology based on clinical clues
In Children (Special Considerations)
The evaluation is age-stratified, because younger children cannot localize symptoms. In infants <3 months with fever, a full sepsis workup including CSF examination is standard. The most common serious bacterial illness in children with fever is UTI (3-8% of febrile children <24 months). Tintinalli's Emergency Medicine, p. 788
5. Management and Treatment
Antipyretic Therapy
| Drug | Dose (Adults) | Dose (Children) | Notes |
|---|---|---|---|
| Acetaminophen | 500-1000 mg q4-6h (max 4g/day) | 15 mg/kg/dose q4-6h (max 80 mg/kg/day) | Safe in liver disease at normal doses; also available IV |
| Ibuprofen | 200-400 mg q4-8h | 10 mg/kg/dose q6-8h (max 40 mg/kg/day) | Not for children <6 months; avoid in renal impairment |
| Aspirin | 325-650 mg q4-6h | AVOID in children (Reye syndrome risk) | COX inhibitor; not first-line for fever |
Should fever always be treated?
- Fever in itself is generally not dangerous at levels below ~41°C (105.8°F)
- However, fever causes discomfort, increases metabolic demand, and may lower the seizure threshold in susceptible children (febrile seizures)
- Treating fever does not clear the underlying infection faster - it provides symptomatic relief
Causal Treatment
- Antibiotics for bacterial infections (guided by cultures and sensitivities)
- Antivirals (e.g., aciclovir, oseltamivir) for specific viral infections
- Antifungals for fungal infections, especially in immunocompromised patients
- Antimalarials, antiparasitics as appropriate
- Immunosuppressants/DMARDs for inflammatory/autoimmune causes
Supportive Care
- Adequate hydration (fever increases insensible losses)
- Nutrition (prolonged fever increases metabolic rate significantly)
- Cooling measures for hyperpyrexia (>41°C): tepid sponging, cooling blankets, cool IV fluids
6. Fever of Unknown Origin (FUO)
Definition (Harrison's 22nd Ed., 2025)
FUO is strictly defined as:
- Fever ≥38.3°C (≥101°F) on at least two occasions
- Illness duration of at least 3 weeks
- No known immunocompromised state
- Diagnosis uncertain despite a minimum standard diagnostic workup (originally: 1 week of inpatient evaluation; now increasingly outpatient-based)
Harrison's Principles of Internal Medicine 22E, p. 197
Etiology (by broad category across large studies)
| Category | Western Europe | China/Asia |
|---|---|---|
| Infections | ~15.5% (range 4-36%) | Higher |
| Noninfectious inflammatory | Variable | Lower |
| Malignancy | ~7% | ~15% |
| No diagnosis | ~40-50% | ~20% |
Infectious causes of FUO:
- Intra-abdominal abscess (liver, spleen, intraperitoneal) - most common in industrialized world
- Tuberculosis (especially extrapulmonary, miliary, or in immunocompromised)
- Culture-negative endocarditis (HACEK organisms, Bartonella, Coxiella/Q fever, Brucella, fungi)
- Osteomyelitis (vertebral osteomyelitis is the most common site in FUO)
- CMV, EBV (most common viral causes)
- Zoonoses: cat-scratch disease (Bartonella) - consider in young patients with pet exposure and tender lymphadenopathy
Noninfectious inflammatory causes:
| Clue | Diagnosis |
|---|---|
| Ferritin dramatically elevated (>2000 ng/mL) | Adult-onset Still's disease (AOSD) |
| Symmetric polyarticular arthritis (wrist, MCP, PIP) | Rheumatoid arthritis |
| Pancytopenia, low complement, young woman | SLE |
| Sterile inflammatory arthritis after treated STI | Reactive arthritis |
| Bilateral hilar lymphadenopathy | Sarcoidosis |
| Hepatitis B, testicular pain, livedo reticularis | Polyarteritis nodosa |
| PMR + temporal headache in elderly | Giant cell arteritis |
| Recurrent fever since childhood (Mediterranean descent) | Familial Mediterranean fever |
| Colonoscopy needed for diagnosis | Inflammatory bowel disease |
Malignant causes: Lymphoma, leukemia, renal cell carcinoma, hepatocellular carcinoma, intravascular lymphoma (rare but notorious for causing FUO)
FUO Workup Approach
- First line: CBC, ESR, CRP, LFTs, LDH, ferritin, blood cultures x3, urinalysis/culture, CXR, HIV, CMV/EBV serology, ANA, RF, ANCA
- CT chest/abdomen/pelvis - high yield; early identification of lymphadenopathy, masses, abscesses
- Echocardiography - if endocarditis suspected
- Bone marrow biopsy - if hematologic malignancy or miliary TB suspected
- PET-CT - increasingly used to identify occult foci of infection or malignancy
- Molecular testing - PCR panels for blood/body fluids have greatly expanded pathogen detection
- Tissue biopsy - of accessible lymph nodes, liver, skin lesions
Goldman-Cecil Medicine, p. 2941; Harrison's 22E, p. 198
FUO Treatment
- Rational treatment is based on final diagnosis
- Empirical trials should generally be avoided - they can obscure the diagnosis (antibiotics destroy cultures; glucocorticoids mask lymphoma)
- Exceptions for empirical therapy:
- Hemodynamic instability or neutropenia → empirical broad-spectrum antibiotics
- Positive TST/IGRA, or endemic area + clinical picture → empirical antituberculars (after collecting mycobacterial cultures/PCR)
- Supportive: acetaminophen or NSAIDs for symptomatic relief
- Colchicine: highly effective prophylaxis for FMF; may be tried in suspected FMF
- IL-1 inhibitors (anakinra): effective for autoinflammatory syndromes (FMF, CAPS, TRAPS, AOSD) once infection and malignancy are excluded
- Glucocorticoids: dramatic effect in giant cell arteritis/PMR, but avoid until infection and lymphoma are excluded
- Prognosis: ~40-50% of FUO in developed countries remain undiagnosed; the majority of these resolve spontaneously with a favorable long-term outcome
Harrison's Principles of Internal Medicine 22E, p. 198
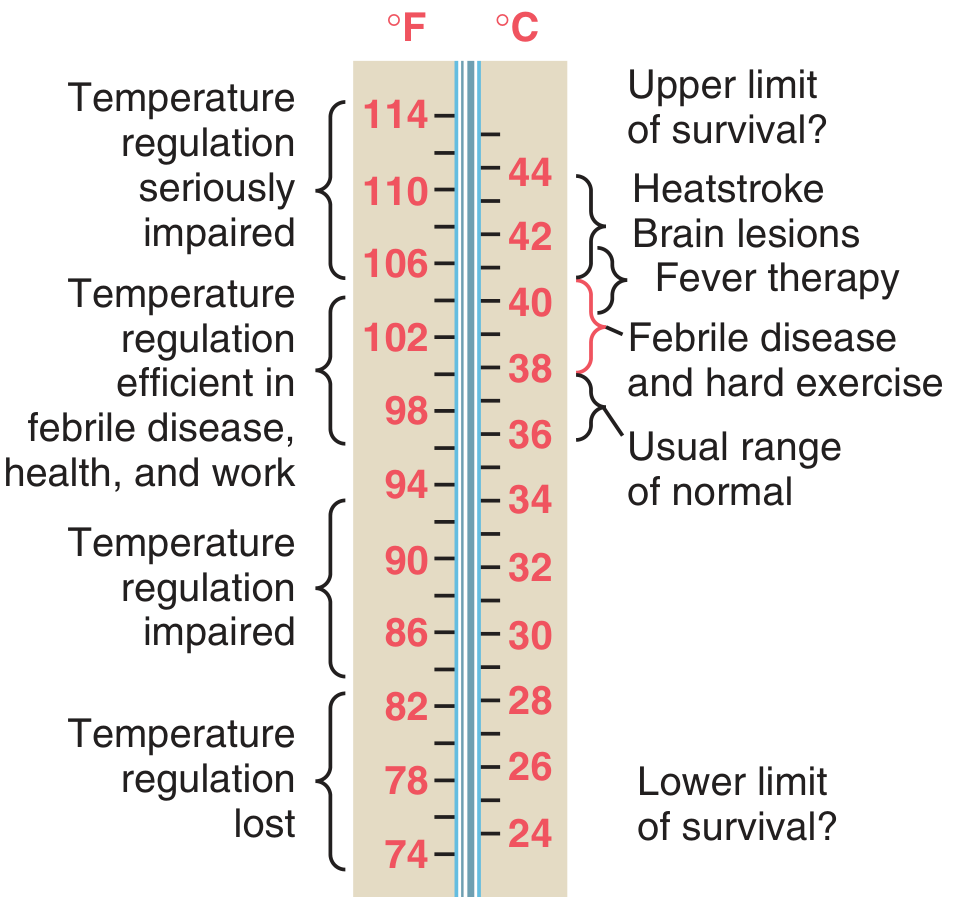
7. Dangerous Temperature Thresholds
| Temperature | Clinical State |
|---|---|
| 36-38°C (97-100.4°F) | Normal range |
| 38-41°C (100.4-105.8°F) | Fever - thermoregulation intact |
| >41°C (>105.8°F) | Hyperpyrexia - risk of brain damage, multiorgan failure |
| >42-44°C (>107.6-111.2°F) | Heatstroke range - tissue damage, hemorrhagic lesions in brain, liver, kidney failure |
| >44°C (>111°F) | Upper limit of survival? |
Heatstroke differs from fever in that it is due to failure of thermoregulation (e.g., overwhelming heat exposure, inability to sweat), NOT a raised hypothalamic set-point. Treatment: rapid cooling (tepid sponging + cool air, cold-water immersion in severe cases).
Malignant hyperthermia - triggered by inhalation anesthetics in genetically susceptible individuals → massive skeletal muscle metabolic rate increase → fatal hyperthermia if untreated. Treatment: dantrolene (skeletal muscle relaxant).
Guyton & Hall, p. 901; Costanzo Physiology, p. 184
Key Sources:
- Guyton and Hall, Textbook of Medical Physiology - Chapters 73-74 (thermoregulation)
- Costanzo, Physiology, 7th Ed., p. 184
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 22 (FUO)
- Goldman-Cecil Medicine, Chapter 259 (fever approach and FUO)
- Frameworks for Internal Medicine - FUO categories and causes
- Tintinalli's Emergency Medicine - fever in children, postoperative fever
- Bailey & Love's Short Practice of Surgery, 28th Ed. - postoperative fever
This is a shared conversation. Sign in to Orris to start your own chat.