functional MRI - 20 MARKS
Reading File
Finding Sources
Searching the Web
functional MRI BOLD signal principles applications clinical neuroscience
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile a thorough 20-mark answer on functional MRI.
Functional MRI (fMRI) - Comprehensive Review
1. Introduction and Overview
Functional magnetic resonance imaging (fMRI) is the dominant method for measuring biological processes in the human brain and linking them to behavior. It is non-invasive (no surgery, ionizing radiation, or disruptive intervention), measures brain function over short periods (seconds), and images activity across the whole brain simultaneously - making it ideal for studying how multiple regions interact during complex behaviors. Since its development in the early 1990s, it has become a pillar of both neurocognitive research and clinical neuroscience.
- Eric Kandel, Principles of Neural Science, 6th Ed.
- Bradley & Daroff's Neurology in Clinical Practice
2. Physical Basis - Magnetic Resonance
At the core of every fMRI machine is a powerful magnet (most modern machines are 3 Tesla; research systems may be 7T). The technique exploits the magnetic properties of hydrogen atom protons.
Key physics principles:
| Concept | Detail |
|---|---|
| Proton spin | Protons have angular momentum and intrinsically rotate, giving them a magnetic dipole |
| Alignment | In a strong external magnetic field, protons align with the field direction |
| Larmor precession | A perpendicular RF pulse tips protons out of alignment; they precess at the Larmor frequency (field strength × gyromagnetic ratio) |
| Signal emission | Precessing protons emit RF signals detected by the head coil |
| Relaxation | After the RF pulse ends, protons return to alignment (T1 relaxation) and lose phase coherence (T2/T2* relaxation); these decay rates differ between tissue types and produce image contrast |
The gradient coils superimpose a spatially varying magnetic field on the main field, giving each location in the brain a unique Larmor frequency. This frequency-encoding allows spatial localization of the MR signal.
3. The BOLD Signal - Blood Oxygen Level Dependent Contrast
fMRI does not directly image electrical neural activity. Instead it uses the BOLD effect as an indirect surrogate for neuronal activity.
The Neurovascular Coupling Mechanism
When neural activity increases in a region, there is a local increase in energy (oxygen) demand. Paradoxically, cerebral blood flow (CBF) rises far in excess of the actual oxygen extraction. The result is a local surplus of oxygenated hemoglobin at the active site.
This matters because:
- Deoxyhemoglobin is paramagnetic - it distorts the local magnetic field, causing T2* signal loss (darker on T2*-weighted images)
- Oxyhemoglobin is diamagnetic - it does not disturb the field, so the signal is brighter
When a brain region is activated:
- Neural firing → local oxygen demand
- Neurovascular coupling → disproportionate increase in CBF
- Local deoxyhemoglobin concentration falls
- T2* signal increases (~1-5% signal change)
- This is detected as the positive BOLD response
This counterintuitive relationship (more activity = less deoxyhemoglobin = brighter signal) is central to understanding fMRI.
Hemodynamic Response Function (HRF)
The BOLD response to a brief neural event follows a characteristic shape:
- Initial dip (optional, not always seen): transient increase in deoxyhemoglobin before CBF rises
- Peak: BOLD signal peaks ~4-6 seconds after the neural event
- Undershoot: prolonged post-stimulus reduction in BOLD below baseline before return to rest
The delay between neural activity and BOLD peak (~4-6 sec) means fMRI has limited temporal resolution compared to EEG/MEG, but excellent spatial resolution (~1-3 mm).
Signal Sources and Field Strength
The BOLD signal has multiple contributors depending on vessel size:
-
Large vessels (>20 μm): static dephasing from deoxyhemoglobin; can be eliminated with spin-echo sequences
-
Capillaries/small vessels: intravascular and extravascular dynamic dephasing (water molecules diffusing through distorted magnetic field)
-
At 1.5T: intravascular dynamic dephasing dominates
-
At 7T: intravascular contribution becomes negligible; extravascular capillary signal dominates, improving spatial specificity to the actual site of activation
-
Kaplan & Sadock's Comprehensive Textbook of Psychiatry, p. 1111-1112
4. fMRI Equipment and Experimental Setup
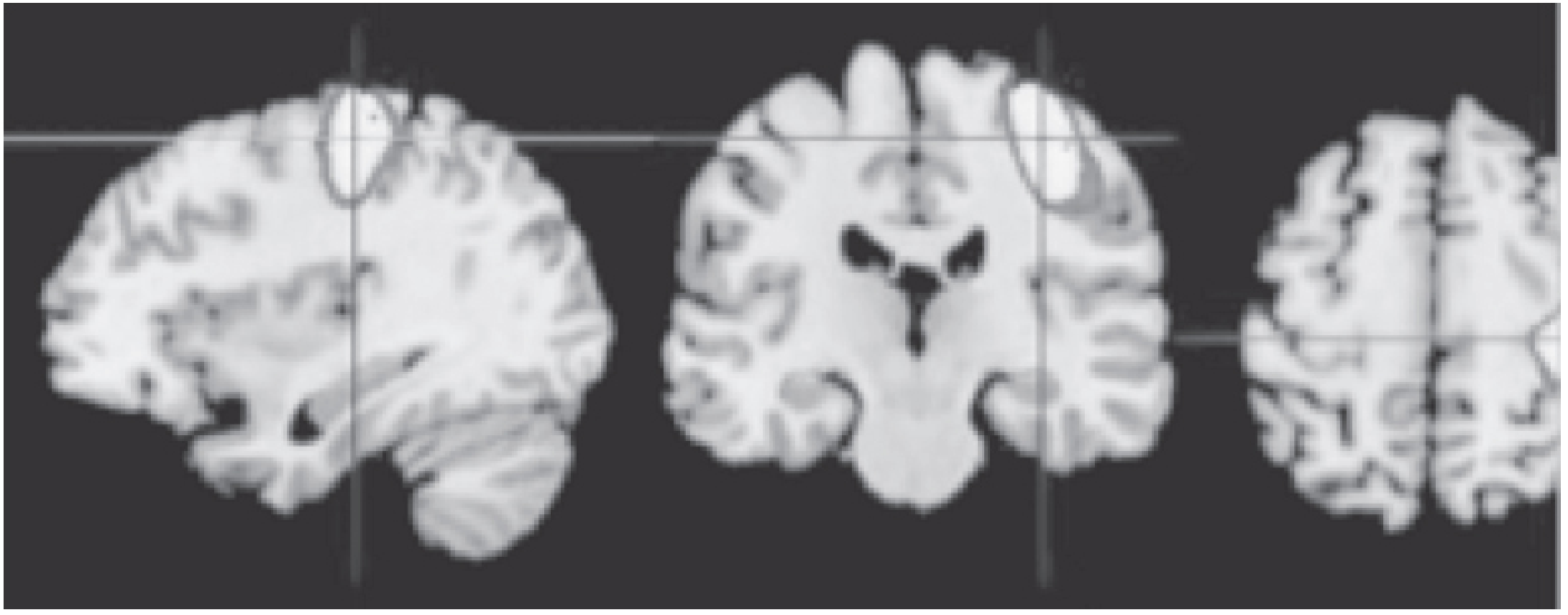
Functional MRI at 3T during right-hand movement. The left motor cortex shows activation, highlighted as regions of most intense T2* signal change. (Kaplan & Sadock)
Hardware:
- MRI bore (tunnel) with subject lying supine
- Head coil (helmet-like) receives RF signals from brain
- Visual stimuli presented via mirror angled toward a screen at back of bore
- Auditory stimuli via MRI-compatible headphones
- Responses collected via button box; eye movements via eye tracker
Pulse sequences used:
- Gradient Echo (GRE) EPI (Echo Planar Imaging) - the standard workhorse; fast, T2*-sensitive, susceptible to signal dropout near air-tissue interfaces (frontal/temporal)
- Spin Echo EPI - less susceptible to large-vessel artifacts; better spatial specificity at high fields
- Multiband/simultaneous multi-slice - acquires multiple slices simultaneously, improving temporal resolution
5. Experimental Designs
| Design Type | Description | Advantages | Disadvantages |
|---|---|---|---|
| Block design | Alternating epochs of task (20-30s) and rest | High statistical power, simple analysis | Cannot separate individual trials |
| Event-related design | Brief trials (~2-10s), jittered intervals, counterbalanced | Separates individual trial types, captures transient responses | Lower SNR than block design |
| Subtraction paradigm | Experimental condition minus control condition isolates one cognitive process | Identifies task-specific activations | Assumes pure insertion of cognitive components |
| Resting state (Rs-fMRI) | Subjects lie still; spontaneous BOLD fluctuations analyzed | No task compliance required; reveals intrinsic network organization | Higher inter-scanner and longitudinal variability |
- Bradley & Daroff's Neurology in Clinical Practice, p. 836
6. Data Analysis
Preprocessing Steps
Before analysis, raw data must undergo preprocessing:
- Slice timing correction - accounts for the time difference between slices acquired within each volume
- Head motion correction - realignment of volumes to a reference; motion is a major source of artifact
- Spatial smoothing - Gaussian kernel applied to improve SNR and normalize across subjects
- Temporal filtering - removes low-frequency drift and high-frequency noise
- Spatial normalization (co-registration) - aligning each subject's brain to a standard template (e.g., MNI space) for group analysis
Three Major Analytical Approaches
A. Localization (Univariate Analysis - GLM)
- The General Linear Model (GLM) models each voxel's time course as a linear combination of predictors
- The HRF is convolved with the experimental design to predict expected BOLD responses
- Statistical maps (t-maps, F-maps) identify voxels where BOLD activity differs significantly between conditions
- Result: activation maps showing which brain regions participate in a task
B. Multivoxel Pattern Analysis (MVPA) - Decoding
- Rather than testing one voxel at a time, MVPA examines patterns of activity across multiple voxels
- Classifier-based MVPA: trains a machine learning classifier (e.g., support vector machine, regularized logistic regression) on a subset of data, then tests its ability to decode conditions from held-out data
- Representational Similarity Analysis (RSA): computes pairwise similarity/distance matrices between patterns evoked by different stimuli; can compare neural similarity to behavioral similarity or to computational model predictions
- Can reveal what information is represented in a region, not just whether it is active
C. Functional Connectivity Analysis
- Examines correlations of BOLD time courses between regions over time
- Regions with correlated activity are said to form functional networks
- Methods include:
- Seed-based correlation: extract time course from a seed ROI, correlate with all other voxels
- Independent Component Analysis (ICA): data-driven decomposition into independent spatial maps
- Graph theory: characterizes network topology (hubs, clustering coefficient, path length)
- Dynamic Causal Modeling (DCM) and Granger causality: test directed (effective) connectivity
Software packages: AFNI, FSL, SPM (all open-source)
- Kandel, Principles of Neural Science, p. 163-168
- Bradley & Daroff, p. 833-836
7. Resting-State fMRI and Intrinsic Brain Networks
Rs-fMRI analyzes spontaneous BOLD fluctuations when no task is performed. This has revealed consistent, reproducible large-scale networks of intrinsically correlated regions:
| Network | Key Regions | Function |
|---|---|---|
| Default Mode Network (DMN) | Medial prefrontal cortex, posterior cingulate, precuneus, hippocampus, lateral temporal cortex | Active at rest, suppressed during externally directed tasks; implicated in self-referential thought, memory consolidation |
| Frontoparietal (Executive) Network | Lateral PFC, posterior parietal cortex | Working memory, cognitive control |
| Salience Network | Anterior insula, dorsal anterior cingulate | Detection of salient stimuli; switches between DMN and frontoparietal networks |
| Sensorimotor Network | Primary motor/somatosensory cortex | Sensorimotor processing |
| Visual Network | Occipital cortex | Visual processing |
The DMN is the most studied; it is deactivated during externally directed cognitive tasks and shows disrupted connectivity in Alzheimer's disease, schizophrenia, and depression.
- Kandel, Principles of Neural Science
- Bradley & Daroff, p. 835
8. Fundamental Scientific Insights from fMRI
Face Perception and the Fusiform Face Area (FFA)
- fMRI identified the fusiform face area (FFA) in the right lateral fusiform gyrus as highly selective for face stimuli vs. other visual categories
- Adaptation designs showed the FFA represents intact faces differently from scrambled configurations
- Patients with prosopagnosia (impaired face recognition) showed that FFA adaptation was absent, linking its activity to behavioral recognition
- These human findings inspired invasive neuronal recording studies in non-human primates that mapped the face patch system
Memory
- fMRI has challenged purely modular theories of memory; the hippocampus is active not only during encoding/retrieval but also in imagination of future events ("episodic future thinking")
Decision-Making and Reward
-
Reward prediction error (difference between expected and received reward) correlates with BOLD activity in the ventral striatum - consistent with the role of midbrain dopaminergic neurons in reinforcement learning
-
This was discovered using computational models (Rescorla-Wagner learning models) whose trial-by-trial outputs were included as parametric regressors in fMRI analyses
-
Kandel, Principles of Neural Science, p. 168-170
9. Clinical Applications
| Application | Details |
|---|---|
| Pre-surgical mapping | Mapping eloquent cortex (motor, language, memory) before tumor resection or epilepsy surgery; identifies critical areas to spare (replaces or supplements Wada test) |
| Language lateralization | Determines dominant hemisphere for language in epilepsy surgery candidates |
| Epilepsy | EEG-fMRI: simultaneous EEG + resting-state BOLD; interictal spikes correlated with BOLD changes localize the seizure focus |
| Brain tumors | Maps functional cortex near tumor; note: BOLD may be attenuated adjacent to gliomas due to loss of autoregulation in tumor neovasculature |
| Cerebrovascular disease | Breath-holding or CO₂ challenge maps cerebrovascular reactivity; regions failing to show BOLD rise indicate poor vascular reserve (useful in moyamoya, atherosclerosis) |
| Dementia | Rs-fMRI detects disrupted functional connectivity in prodromal/manifest Alzheimer's disease (DMN disruption) |
| Psychiatry | Research tool for schizophrenia, depression, autism (abnormal functional connectivity); potential future diagnostic biomarker |
- ASFNR; Bradley & Daroff; Kaplan & Sadock
10. Limitations and Interpretive Challenges
Technical Limitations
- Temporal resolution: BOLD peaks ~4-6 seconds after neural events (poor temporal resolution vs. EEG/MEG)
- Spatial resolution: typically ~2-3 mm voxels; layer-specific imaging (~0.5 mm) only possible at 7T
- Signal dropout: gradient-echo EPI suffers from susceptibility artifacts near air-tissue interfaces (orbitofrontal cortex, inferior temporal lobes)
- BOLD is not neural activity directly: it is a hemodynamic surrogate; neurovascular coupling may be disrupted in disease (brain tumors, cerebrovascular disease, aging)
- Motion artifacts: head movement corrupts data; requires motion correction and quality control; problematic in children, cognitively impaired patients, or those with involuntary movements
- Low SNR: typical BOLD signal change is only 1-5%
Conceptual/Statistical Challenges
Forward inference (most fMRI studies): manipulate a process, find which brain regions differ between conditions → can validly infer regional involvement.
Reverse inference (problematic): observe BOLD activation → infer which mental process was engaged. This is logically weak because most brain regions support multiple functions (the problem of non-uniqueness).
Multiple comparisons: testing hundreds of thousands of voxels creates a severe multiple comparisons problem; requires corrections (familywise error rate, false discovery rate, cluster-based thresholding).
Publication bias and replication: fMRI studies have been criticized for underpowered designs; the field has moved toward larger samples, open data sharing (OpenNeuro.org), and pre-registration.
- Kandel, Principles of Neural Science, p. 170
11. Comparison with Other Neuroimaging Modalities
| Modality | Spatial Resolution | Temporal Resolution | Invasiveness | What It Measures |
|---|---|---|---|---|
| fMRI | ~2-3 mm | ~1-2 sec (limited by HRF) | Non-invasive | Hemodynamic surrogate of neural activity (BOLD) |
| PET | ~5-7 mm | ~30-60 sec | Radiotracer injection | Cerebral blood flow, metabolism, receptor binding |
| EEG | Poor (~cm) | Excellent (~ms) | Non-invasive (scalp electrodes) | Direct electrical activity (scalp-averaged) |
| MEG | ~5 mm | Excellent (~ms) | Non-invasive | Magnetic fields from neuronal currents |
| NIRS | Poor | Moderate (~sec) | Non-invasive | Hemoglobin oxygenation (cortical surface) |
fMRI is preferred for whole-brain coverage, spatial detail, and non-invasiveness. EEG/MEG are preferred when millisecond temporal resolution is needed.
12. Technical Advances and Future Directions
- Ultra-high field (7T): greater SNR, laminar-specific imaging, reduced intravascular artifact
- Multiband/multiecho sequences: faster acquisition, reduced venous signal contribution
- Real-time fMRI neurofeedback: subjects shown their own BOLD signal in real time to self-regulate brain activity (therapeutic applications in chronic pain, depression)
- Quantitative/calibrated fMRI: combines BOLD with CBF (ASL) and CMRO₂ measurements to provide absolute physiological parameters rather than relative signal changes
- Machine learning and AI: deep learning for automated analysis, brain fingerprinting, prediction of behavior and clinical outcomes
- Standardization and open data: OpenNeuro.org enables mega-analyses across thousands of datasets
Summary Table (Key Facts for Exam)
| Feature | Value/Concept |
|---|---|
| Contrast mechanism | BOLD (blood oxygen level dependent) |
| Magnetic property exploited | Deoxyhemoglobin is paramagnetic; oxyhemoglobin is diamagnetic |
| Signal change | ~1-5% increase in T2* signal with activation |
| Temporal resolution | Seconds (limited by hemodynamic response ~4-6 sec peak) |
| Spatial resolution | ~2-3 mm at 3T; ~0.5 mm at 7T |
| Main experimental designs | Block, event-related, resting-state |
| Main analysis approaches | GLM (localization), MVPA (decoding), functional connectivity |
| Key resting-state network | Default Mode Network (DMN) |
| Key clinical use | Pre-surgical cortical mapping (motor/language) |
| Key limitation | Hemodynamic surrogate; poor temporal resolution; motion artifact |
Sources:
- Eric Kandel, Principles of Neural Science, 6th Edition - Chapter 6 (fMRI)
- Kaplan & Sadock's Comprehensive Textbook of Psychiatry - Functional MRI Methodology (pp. 1111-1112)
- Bradley & Daroff's Neurology in Clinical Practice - Functional Neuroimaging (pp. 833-836)
- American Society of Functional Neuroradiology (ASFNR) - What is BOLD fMRI?
This is a shared conversation. Sign in to Orris to start your own chat.