Describe Nerve supply of uterus and cervix.pain pathways and management of labour pain
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I have all the necessary information to compose a thorough, well-cited answer. Let me now compile the complete response.
Nerve Supply of the Uterus and Cervix, Pain Pathways, and Management of Labour Pain
1. Nerve Supply of the Uterus and Cervix
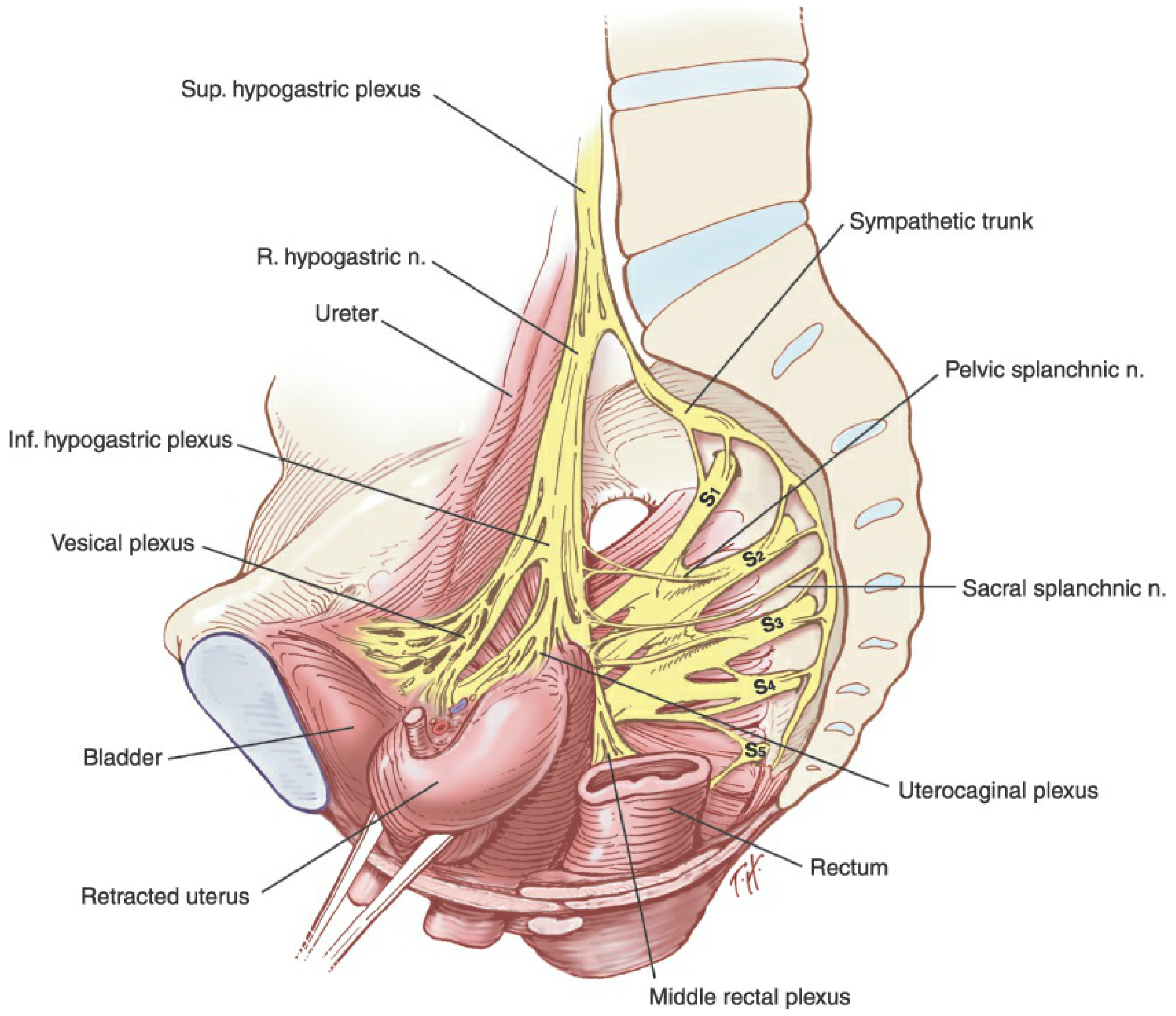
The uterus and cervix receive a dual innervation - autonomic (sympathetic + parasympathetic) and somatic - primarily through the uterovaginal plexus (Frankenhäuser ganglion).
The Uterovaginal Plexus (Frankenhäuser Ganglion)
This is the final common pathway for innervation of the uterus, vagina, clitoris, and vestibular bulbs. It is part of the inferior hypogastric plexus (pelvic plexus), a dense network of nerves and ganglia lying along the lateral pelvic sidewall overlying branches of the internal iliac vessels. The course of the uterovaginal plexus runs along the uterine vessels and through the cardinal and uterosacral ligaments.
The inferior hypogastric plexus has three functional subdivisions:
| Subdivision | Target | Course |
|---|---|---|
| Vesical plexus | Bladder + urethra | Along vesical vessels |
| Middle rectal plexus | Rectum | Along middle rectal vessels |
| Uterovaginal plexus | Uterus, vagina, clitoris, vestibular bulbs | Along uterine vessels via cardinal/uterosacral ligaments |
(Berek & Novak's Gynecology, p. 174)
Sympathetic Supply
The superior hypogastric plexus (presacral nerve) is the continuation of the aortic plexus, lying beneath the peritoneum in front of the terminal aorta and L5 vertebra at the sacral promontory. It is composed of two or three incompletely fused trunks containing:
- Preganglionic fibers from lumbar nerves (L1-L2)
- Postganglionic fibers from higher sympathetic ganglia and sacral sympathetic trunks
- Visceral afferent fibers
Just below the sacral promontory, it divides into two hypogastric nerves, which course inferiorly and laterally to connect with the inferior hypogastric plexuses (pelvic plexuses). Sympathetic/sensory fibers to the uterus and cervix ultimately derive from T10-L1 spinal segments.
Parasympathetic Supply
Parasympathetic fibers arise from the pelvic splanchnic nerves (nervi erigentes) originating from S2-S4. These join the inferior hypogastric plexus and distribute via the uterovaginal plexus to supply the uterus and cervix.
Somatic Supply
The perineum and lower vagina receive somatic innervation from the pudendal nerve (S2-S4), which is important in the second stage of labour.
Summary Table: Nerve Supply of Female Pelvic Organs
| Organ | Spinal Segments | Nerves |
|---|---|---|
| Upper vagina, cervix, uterine corpus, inner 1/3 of fallopian tubes, broad ligament | T11-L2; S2-S4 | Thoracolumbar sympathetics via hypogastric plexus; sacral parasympathetics via pelvic nerve |
| Ovaries, outer 2/3 of fallopian tubes, upper ureter | T9-T10 | Thoracic sympathetics via renal and aortic plexus; celiac and mesenteric ganglia |
| Pelvic floor, anus, perineum, lower vagina | S2-S4; L1-L2 | Pudendal, inguinal, genitofemoral, posterior femoral cutaneous |
| Lower abdominal wall, anterior vulva, clitoris | L1-L2 | Ilioinguinal, genitofemoral |
(Berek & Novak's Gynecology, Table 12-2, p. 557)
Anatomical Diagram: Presacral/Pelvic Nerve Plexuses
2. Pain Pathways During Labour
Labour pain arises from three distinct sources:
- Contraction of the myometrium against the resistance of the cervix and perineum
- Progressive dilation of the cervix and lower uterine segment
- Stretching and compression of pelvic and perineal structures
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1607)
First Stage of Labour (Visceral Pain)
- Pain is primarily visceral from uterine contractions and cervical dilation
- Initially confined to T11-T12 dermatomes during the latent phase
- Expands to involve T10-L1 dermatomes during the active phase
- Pathway: Visceral afferent fibers travel with sympathetic nerve fibers → uterovaginal plexus → inferior hypogastric plexus → enter the spinal cord with T10-L1 nerve roots
Second Stage of Labour (Somatic + Visceral Pain)
- Onset of perineal pain signals fetal descent
- Stretching and compression of pelvic and perineal structures intensifies pain
- Sensory innervation of the perineum via the pudendal nerves (S2-S4)
- Total pain now spans T10-S4 dermatomes
Referred Pain
Because the upper vagina, cervix, and uterine corpus share visceral innervation (T11-L2; S2-S4) with the large intestine, rectum, bladder, lower ureter, and lower small intestine, pain from the reproductive organs can be referred to the same dermatomes as GI/GU pain. This overlap explains the lower abdominal cramping, back pain, and radiating leg pain commonly experienced during labour. (Berek & Novak's Gynecology, p. 557)
3. Management of Labour Pain
A. Psychological and Non-Pharmacological Techniques
- Bradley, Dick-Read, Lamaze, LeBoyer methods - patient education and positive conditioning
- Lamaze technique: deep breath at contraction onset, then rapid shallow breathing; cognitive distraction ("focal point")
- Other methods: hypnosis, transcutaneous electrical nerve stimulation (TENS), biofeedback, acupuncture
- Success varies considerably between patients; many require additional analgesia
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1607)
B. Parenteral Agents
Nearly all parenteral opioids and sedatives readily cross the placenta and can affect the fetus. Their use is therefore limited to early labour or when regional techniques are unavailable.
| Agent | Dose | Notes |
|---|---|---|
| Meperidine | 10-25 mg IV or 25-50 mg IM (up to 100 mg total) | Peak fetal depression: 10-20 min (IV), 1-3 h (IM); give only when delivery not expected within 4 h |
| Fentanyl | 25-100 mcg/h IV | Onset 3-10 min; analgesia ~60 min; respiratory depression outlasts analgesia |
| Remifentanil (PCA) | 40 mcg bolus, 2-min lockout | Ultra-short acting; equally or more efficacious than other parenteral opioids; requires 1:1 patient monitoring |
| Nitrous oxide | Inhaled 50% N₂O/O₂ | Mild labour pain; minimal effect on uterine blood flow or contractions |
(Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1608-1609)
C. Pudendal Nerve Block
- Combined with perineal infiltration of local anaesthetic for second stage perineal anaesthesia
- Technique: Koback needle or Iowa trumpet guide; needle placed transvaginally beneath the ischial spine on each side; advanced 1-1.5 cm through the sacrospinous ligament; 10 mL of 1% lidocaine or 2% chloroprocaine injected
- Paracervical blocks are no longer used - associated with a high rate of fetal bradycardia from uterine arterial vasoconstriction and increased fetal drug levels
(Morgan & Mikhail's Clinical Anesthesiology, 7e, p. 1609)
D. Regional Anaesthetic Techniques (Gold Standard)
Epidural or intrathecal techniques, alone or in combination, are currently the most popular and effective methods of pain relief during labour and delivery. Combinations of local anaesthetics and opioids provide synergistic analgesia, reduce dose requirements, minimise maternal side effects, and cause little to no neonatal depression.
1. Spinal (Intrathecal) Opioids Alone
- Useful for high-risk patients who cannot tolerate sympathectomy (hypovolemia, aortic stenosis, Eisenmenger syndrome, pulmonary hypertension)
- No motor block or sympathectomy
- Disadvantages: incomplete analgesia, no perineal relaxation, pruritus, nausea, risk of respiratory depression
- Side effects managed with low-dose naloxone (0.1-0.2 mg/h IV)
2. Epidural Analgesia
- Most commonly used regional technique for labour
- Provides excellent analgesia while keeping the mother awake and cooperative
- Combined epidural spinal analgesia (CSE) provides faster onset
3. Combined Spinal-Epidural (CSE)
- Spinal component for rapid initial analgesia
- Epidural catheter for ongoing maintenance and top-ups
Typical Drug Combinations
- Local anaesthetic (bupivacaine/ropivacaine) + opioid (fentanyl/sufentanil) intrathecally or epidurally
- The synergy allows lower doses of each agent
(Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1609-1611)
Summary: Pain Coverage by Technique
| Technique | Stage Covered | Dermatomes Blocked |
|---|---|---|
| Epidural/Spinal (early labour) | First stage | T10-L1 |
| Pudendal nerve block | Second stage | S2-S4 (perineum) |
| Full epidural/CSE | Both stages | T10-S4 |
| Parenteral opioids | First stage primarily | Systemic |
Key Clinical Points:
- Disruption of the superior hypogastric plexus (e.g., during radical hysterectomy or deep infiltrating endometriosis surgery) can cause de novo bladder, bowel, or sexual dysfunction
- The uterovaginal (Frankenhäuser) ganglion is the critical relay center - historically targeted in presacral neurectomy for dysmenorrhoea
- Paracervical block is contraindicated in labour due to fetal bradycardia risk
- Remifentanil PCA requires mandatory 1:1 nursing monitoring due to maternal respiratory depression risk
This is a shared conversation. Sign in to Orris to start your own chat.