drugs use in treatment of bronchial asthma classification pharmacokinetics adverse effect theraputic uses detail 2nd yr mbbs refer kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, 2nd year MBBS-level answer. Let me compile the complete response:
Drugs Used in Treatment of Bronchial Asthma
Based on Katzung's Basic & Clinical Pharmacology (KDT), 16th Ed. + Lippincott Pharmacology
Mechanism Overview
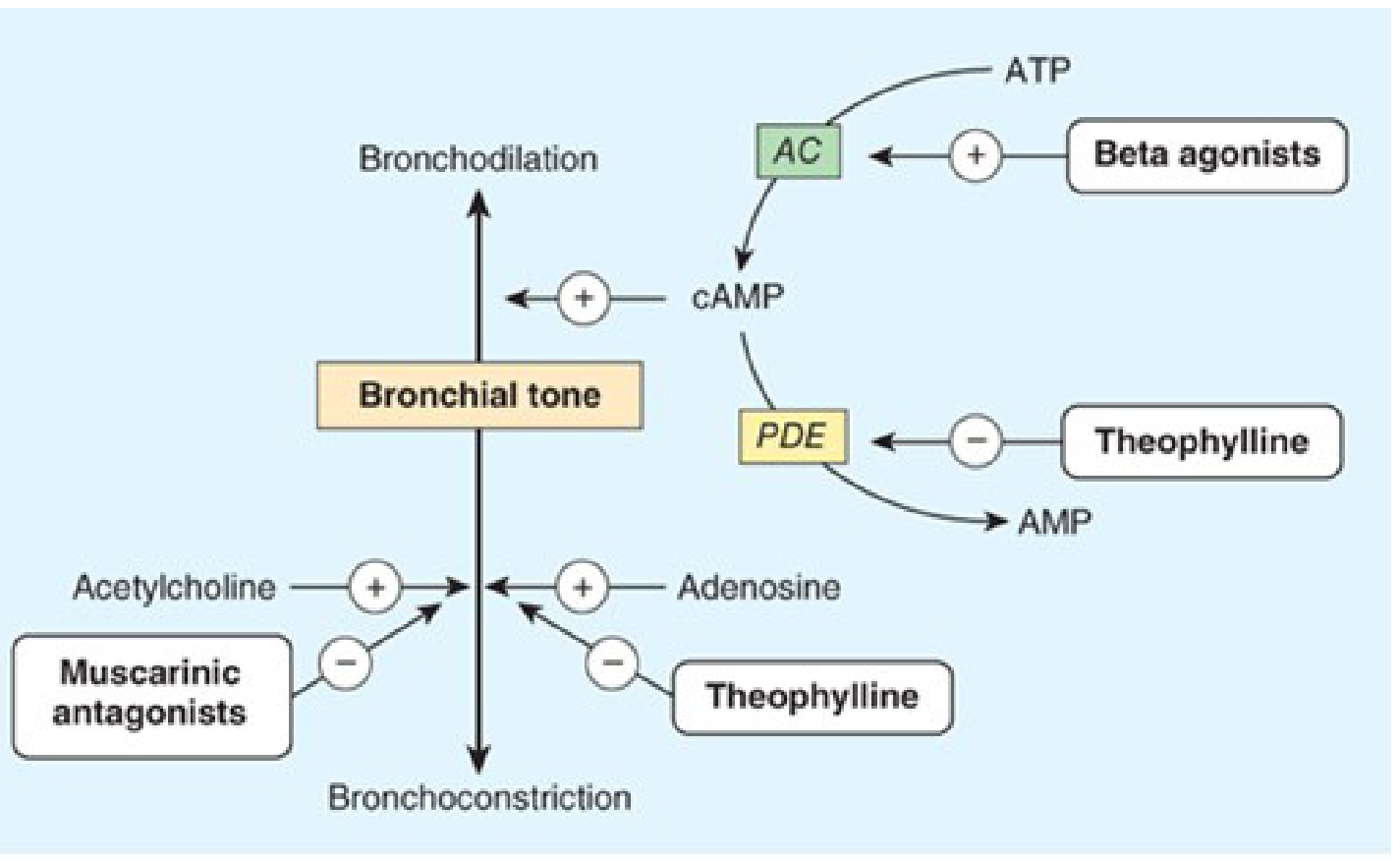
Bronchodilation is promoted by cAMP. Beta agonists increase cAMP synthesis via adenylyl cyclase (AC); theophylline prevents cAMP breakdown by inhibiting phosphodiesterase (PDE); muscarinic antagonists block acetylcholine-mediated bronchoconstriction.
Classification of Antiasthmatic Drugs
A. Bronchodilators (Relievers)
- Beta-2 adrenergic agonists
- Short-acting (SABA): Salbutamol (albuterol), terbutaline, fenoterol
- Long-acting (LABA): Salmeterol, formoterol
- Methylxanthines: Theophylline, aminophylline, doxofylline
- Anticholinergics (Antimuscarinics): Ipratropium bromide (SAMA), tiotropium (LAMA)
B. Anti-inflammatory / Controllers
- Corticosteroids
- Inhaled (ICS): Beclomethasone, budesonide, fluticasone, mometasone
- Systemic: Prednisolone, methylprednisolone (for acute exacerbations)
- Leukotriene Modifiers
- 5-LOX inhibitor: Zileuton
- Cysteinyl LT-receptor antagonists (LTRAs): Montelukast, zafirlukast
- Mast cell stabilizers: Cromolyn sodium (sodium cromoglycate), nedocromil
- Biologics / Monoclonal antibodies: Omalizumab (anti-IgE), mepolizumab, benralizumab (anti-IL-5)
1. Beta-2 Adrenergic Agonists
Mechanism
Bind to beta-2 receptors on airway smooth muscle → activate adenylyl cyclase → increase cAMP → protein kinase A activation → smooth muscle relaxation (bronchodilation). Also inhibit mast cell mediator release and reduce microvascular leakage.
Pharmacokinetics
| Drug | Route | Onset | Duration |
|---|---|---|---|
| Salbutamol (albuterol) | Inhaled/oral/IV | 5-15 min (inhaled) | 4-6 hrs |
| Terbutaline | Inhaled/SC/oral | 5-30 min | 4-6 hrs |
| Salmeterol | Inhaled | 15-20 min | 12 hrs |
| Formoterol | Inhaled | 1-3 min | 12 hrs |
- Inhaled route preferred - greatest local effect with least systemic toxicity
- Optimal aerosol particle size: 2-5 µm
- 80-90% of inhaled dose is deposited in oropharynx
- Salbutamol: partially metabolized to inactive sulfate conjugate; excreted in urine
- Salmeterol: highly lipophilic, binds exosite on beta-2 receptor - explains long duration
Adverse Effects
- Tachycardia and palpitations (beta-1 stimulation, especially non-selective agents)
- Skeletal muscle tremor (fine tremor of hands - most common)
- Hypokalemia (K+ enters cells via Na/K-ATPase stimulation) - can cause arrhythmias
- Nervousness, headache, dizziness
- With LABAs alone (without ICS): increased risk of asthma-related death (black box warning - never use LABA as monotherapy in asthma)
Therapeutic Uses
- SABAs: First-line reliever for acute bronchoconstriction, exercise-induced bronchospasm
- LABAs: Added to ICS for moderate-to-severe persistent asthma (never alone)
- Terbutaline SC: acute severe asthma when inhaled route not possible
- Formoterol: also used as reliever due to fast onset (unlike salmeterol)
2. Methylxanthines (Theophylline)
Mechanism
- PDE inhibition → prevents cAMP breakdown → bronchodilation (main mechanism at therapeutic levels)
- Adenosine receptor antagonism → blocks bronchoconstriction
- Anti-inflammatory effects (at low concentrations)
- Increases diaphragm contractility - useful in COPD
- Mild CNS stimulation
Pharmacokinetics
- Given orally (slow-release tablets preferred) or IV as aminophylline
- Aminophylline = theophylline + ethylenediamine (80% theophylline, more water-soluble)
- Therapeutic serum level: 10-20 mg/L (narrow therapeutic index)
- Toxic level: >20 mg/L
- Hepatic metabolism via CYP1A2 - extensive drug interactions
- Half-life: 8-9 hrs in adults (varies widely)
- Half-life is shortened (t½ decreases) by: smoking, rifampicin, phenytoin, carbamazepine
- Half-life is prolonged (t½ increases) by: erythromycin, ciprofloxacin, cimetidine, heart failure, liver disease, old age
Adverse Effects (dose-dependent, narrow TI)
- Mild (10-20 mg/L): Nausea, vomiting, anorexia, headache, insomnia, restlessness
- Moderate (>20 mg/L): Tachycardia, arrhythmias, hypokalemia, tremor
- Severe toxicity (>40 mg/L): Seizures, ventricular arrhythmias, death
- GI: stimulates gastric acid secretion (avoid in peptic ulcer disease)
Therapeutic Uses
- Oral slow-release: chronic asthma (now largely replaced by ICS)
- IV aminophylline: severe acute asthma / status asthmaticus (as add-on)
- COPD with frequent exacerbations
- Apnea of prematurity (neonates - caffeine preferred)
3. Anticholinergics (Antimuscarinics)
Mechanism
Competitive antagonism at muscarinic (M3) receptors on bronchial smooth muscle and mucous glands → reduce ACh-mediated bronchoconstriction and secretions. Less effective than beta-2 agonists in asthma because cholinergic tone is NOT the predominant mechanism in asthma (unlike COPD, where they are preferred).
Pharmacokinetics
- Ipratropium bromide: Inhaled (MDI/nebulizer), onset 15-30 min, duration 4-6 hrs; quaternary ammonium compound - poorly absorbed systemically, minimal CNS effects
- Tiotropium: Inhaled (DPI), long-acting (once daily, 24 hrs), primarily used in COPD
Adverse Effects
- Dry mouth (most common)
- Urinary retention (caution in BPH)
- Constipation
- Blurred vision (if accidentally sprayed in eyes)
- Tachycardia (less than atropine because poorly absorbed)
- Does NOT cause the systemic anticholinergic effects of atropine (crosses blood-brain barrier poorly)
Therapeutic Uses
- COPD: Drug of choice (tiotropium preferred)
- Asthma: Alternative bronchodilator; particularly useful in:
- Patients with beta-blocker-induced bronchospasm
- Psychogenic asthma
- Nocturnal asthma
- Acute severe asthma (combined with salbutamol in nebulization)
- Not first-line for asthma (beta-2 agonists preferred)
4. Corticosteroids
Mechanism
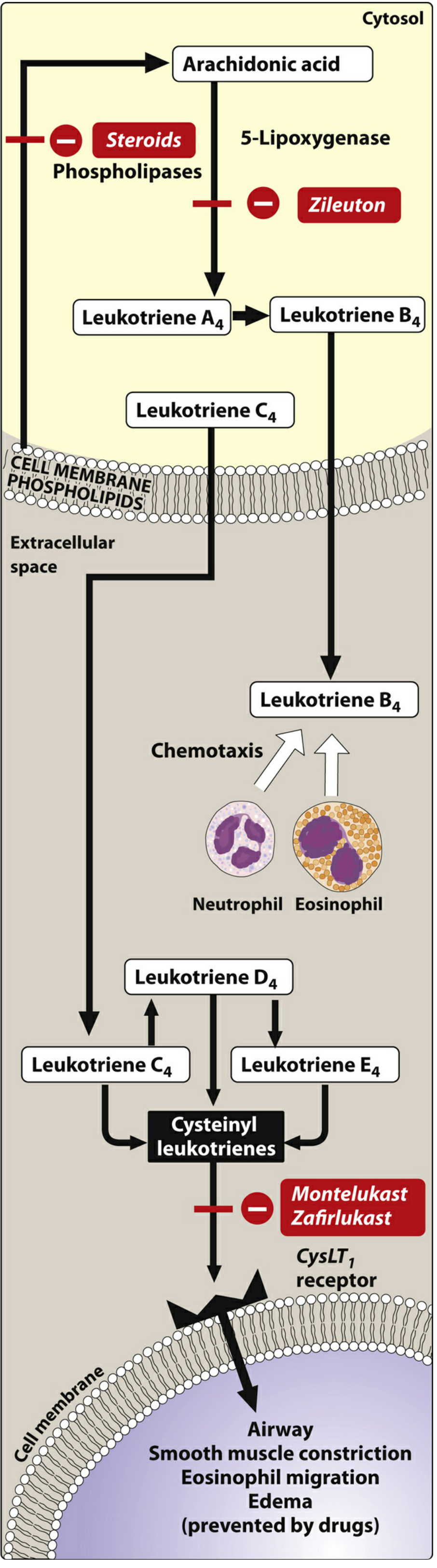
- Inhibit phospholipase A2 → reduce arachidonic acid release → decrease prostaglandins AND leukotrienes
- Reduce inflammatory cell infiltration (eosinophils, macrophages, T lymphocytes)
- Reverse mucosal edema, decrease capillary permeability
- Inhibit leukotriene release
- After months of regular use: reduce airway hyperresponsiveness
Pharmacokinetics (ICS)
| Drug | Bioavailability (inhaled) | t½ | Notes |
|---|---|---|---|
| Beclomethasone | Low systemic (converted to active metabolite) | - | Oldest ICS |
| Budesonide | ~11% systemic | 2 hrs | Safe in pregnancy |
| Fluticasone | ~1% systemic | 14 hrs | Most potent ICS |
| Mometasone | ~<1% systemic | 5 hrs | Once daily |
- Inhaled route: 80-90% deposited in oropharynx (swallowed) → first-pass hepatic inactivation reduces systemic absorption
- Spacer device reduces oropharyngeal deposition
- Systemic steroids (prednisolone): well-absorbed orally, hepatically metabolized
Adverse Effects
ICS (local):
- Oropharyngeal candidiasis (thrush) - prevented by rinsing mouth after use
- Dysphonia (hoarseness) - due to vocal cord myopathy
- Cough, irritation
ICS (systemic - at high doses):
- Adrenal suppression
- Growth retardation in children (small effect)
- Osteoporosis
- Cataracts, glaucoma
Systemic corticosteroids (long-term):
- Cushing syndrome, osteoporosis, hypertension, hyperglycemia
- Peptic ulcer, immunosuppression, myopathy
- HPA axis suppression
Therapeutic Uses
- ICS: Foundation of controller therapy in all grades of persistent asthma
- Oral prednisolone: acute severe asthma (short course / "burst")
- IV methylprednisolone: status asthmaticus
- Key principle: ICS + LABA combination (e.g., fluticasone-salmeterol, budesonide-formoterol) for moderate-severe persistent asthma
5. Leukotriene Modifiers
Mechanism
- Zileuton: Inhibits 5-lipoxygenase → prevents formation of ALL leukotrienes (LTB4 + cysteinyl LTs: LTC4, LTD4, LTE4)
- Montelukast, zafirlukast: Selective CysLT1 receptor antagonists → block effects of cysteinyl leukotrienes (bronchoconstriction, edema, mucus secretion)
Pharmacokinetics
- All are orally active, highly protein-bound
- Extensive hepatic metabolism
- Zileuton + metabolites: excreted in urine
- Montelukast, zafirlukast + metabolites: biliary excretion
- Food impairs absorption of zafirlukast (take on empty stomach)
Adverse Effects
- Montelukast: Headache, GI upset; black box warning - serious neuropsychiatric effects (agitation, depression, suicidal ideation, sleep disturbances)
- Zafirlukast, zileuton: Elevated liver enzymes (monitor LFTs), headache, dyspepsia
- Zafirlukast inhibits CYP2C9, 3A4 (drug interactions - warfarin levels increase)
- Zileuton inhibits CYP1A2
- Rare: Eosinophilic granulomatosis with polyangiitis (EGPA) / Churg-Strauss syndrome (especially when oral steroids tapered)
Therapeutic Uses
- Mild persistent asthma (alternative to ICS or add-on)
- Aspirin-exacerbated respiratory disease (AERD) - particularly effective
- Exercise-induced bronchospasm - prevention
- Allergic rhinitis (montelukast)
- Not for acute attacks (no bronchodilator effect)
6. Mast Cell Stabilizers
Mechanism
Inhibit mast cell degranulation → prevent release of histamine, leukotrienes, and other mediators. Exact mechanism unclear (may block chloride channels). Also inhibit sensory nerve activation.
Pharmacokinetics
- Cromolyn sodium: Inhaled (nebulizer), poor oral bioavailability (<1%), excreted unchanged in urine and bile
- Short duration - requires 3-4 times daily dosing
- Nedocromil: inhaled, 4 times daily
Adverse Effects
- Very safe - minimal adverse effects
- Cough, throat irritation, unpleasant taste (cromolyn)
- Not a bronchodilator - useless in acute attack
Therapeutic Uses
- Prophylaxis only - not for acute attacks
- Alternative therapy for mild persistent asthma (especially children)
- Prevention of exercise-induced and allergen-induced bronchospasm (taken 15-20 min before)
- Allergic rhinitis (nasal spray), mastocytosis (oral cromolyn)
7. Biologics (Monoclonal Antibodies)
| Drug | Target | Indication |
|---|---|---|
| Omalizumab | Anti-IgE (prevents IgE binding to mast cells/basophils) | Moderate-severe allergic asthma with elevated IgE |
| Mepolizumab | Anti-IL-5 (reduces eosinophil production) | Severe eosinophilic asthma |
| Benralizumab | Anti-IL-5Rα (depletes eosinophils) | Severe eosinophilic asthma |
| Dupilumab | Anti-IL-4Rα (blocks IL-4 and IL-13) | Moderate-severe asthma with type 2 inflammation |
- Given SC every 2-4 weeks
- Reserved for severe uncontrolled asthma despite maximum ICS + LABA therapy
- Omalizumab dose based on IgE level and body weight
Step-wise Treatment (GINA Guidelines Summary)
| Severity | Controller | Reliever |
|---|---|---|
| Infrequent symptoms (<2×/month) | Low-dose ICS-formoterol as needed | - |
| Mild persistent (>2×/month, <daily) | Low-dose ICS-formoterol as needed | - |
| Moderate persistent (most days) | Low-dose maintenance ICS-formoterol | ICS-formoterol as needed |
| Severe persistent (daily + low FEV1) | Medium-dose ICS-formoterol | ICS-formoterol as needed |
| Refractory | Add LAMA, LTRA, biologics | SABA as needed |
Acute severe asthma (Status asthmaticus): Nebulized salbutamol + ipratropium, IV methylprednisolone, supplemental O2, IV aminophylline (if no response), IV magnesium sulfate.
Quick Comparison: Drug of Choice
| Situation | Drug of Choice |
|---|---|
| Acute attack (quick relief) | Inhaled SABA (salbutamol) |
| Long-term controller | ICS (beclomethasone/budesonide) |
| ICS + add-on | ICS + LABA combination |
| COPD > asthma | Tiotropium (LAMA) |
| Aspirin-sensitive asthma | Montelukast (LTRA) |
| Allergic asthma (high IgE) | Omalizumab |
| Prophylaxis in children | Cromolyn / low-dose ICS |
| Status asthmaticus | IV methylprednisolone + nebulized salbutamol |
Sources: Katzung's Basic and Clinical Pharmacology 16th Ed., Chapter 20 (Drugs Used in Asthma & COPD); Lippincott Illustrated Reviews Pharmacology, Chapter 41
This is a shared conversation. Sign in to Orris to start your own chat.