Diseases of iris
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have comprehensive data from Kanski's Clinical Ophthalmology and Wills Eye Manual. Let me compile the full answer.
Diseases of the Iris
A systematic overview based on Kanski's Clinical Ophthalmology (10th ed.) and The Wills Eye Manual.
1. Congenital Anomalies
Aniridia
Aniridia is a rare bilateral condition arising from mutations in the PAX6 gene (chromosome 11). PAX6 is adjacent to the WT1 gene (Wilms tumour gene).
- AD form (~2/3 of cases): no systemic implications; complete penetrance, variable expressivity
- Sporadic/WAGR syndrome (~1/3): previously "Miller syndrome" - Wilms tumour, Aniridia, Genito-urinary abnormalities, mental Retardation. ~30% chance of Wilms tumour
- Gillespie syndrome (~1%): AR (not PAX6), cerebellar ataxia + learning disabilities
- Presentation: nystagmus, photophobia at birth; apparent "large pupils" (absent iris)
- Ocular features: limbal stem cell deficiency, corneal vascularization, cataract, lens subluxation, foveal/optic nerve hypoplasia
- Glaucoma (75%): late childhood/adolescence, due to synechial angle closure from rudimentary iris contraction
- Monitoring: abdominal ultrasound every 3 months until age 5 (then 6-monthly to age 10, annually to 16) for Wilms tumour unless WT1 mutation excluded
Fig. - Aniridia: the iris is almost entirely absent with a frill of rudimentary tissue visible on gonioscopy

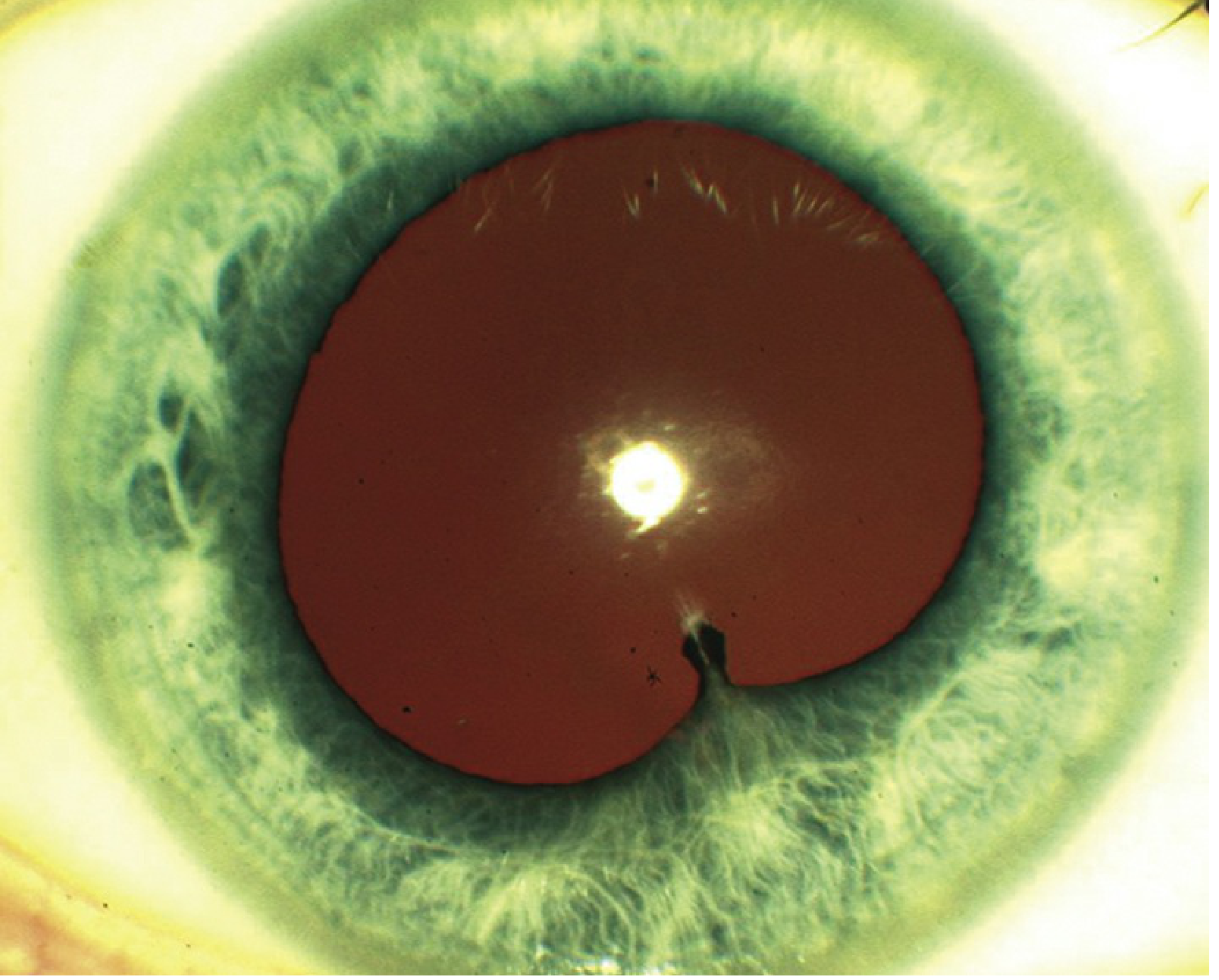
Iris Coloboma
- Results from failed closure of the embryonic fissure (inferior)
- Appears as a keyhole-shaped inferior pupil defect
- May be associated with choroidal/retinal coloboma
- Can occur in isolation or as part of CHARGE syndrome
Congenital Ectropion Uveae
- Uncommon; displacement of posterior pigmented epithelium onto the anterior iris surface
- May be associated with glaucoma
2. Inflammatory Diseases
Anterior Uveitis (Iritis / Iridocyclitis)
The most common form of uveitis. Inflammation of the iris ± ciliary body.
Symptoms:
- Acute: pain, redness, photophobia, consensual photophobia, tearing, decreased vision
- Chronic: reduced vision (cataract, CME, ERM), floaters; minimal pain (e.g., JIA-associated)
Signs (slit lamp):
- Cells and flare in the anterior chamber (graded 0-4+)
- Ciliary flush (perilimbal injection)
- Keratic precipitates (KP):
| KP Type | Associated Conditions |
|---|---|
| Fine KP | HSV, VZV, CMV, Fuchs heterochromic iridocyclitis |
| Small non-granulomatous KP | HLA-B27, JIA, trauma, Posner-Schlossman |
| Mutton-fat (granulomatous) KP | Sarcoidosis, TB, syphilis, VKH, sympathetic ophthalmia |
| Coin-shaped KP | CMV uveitis (characteristic) |
- Posterior synechiae (iris-to-lens adhesions), iris nodules, hypopyon (HLA-B27, Behçet)
- IOP: usually low (ciliary hyposecretion); raised in herpetic, Fuchs, Posner-Schlossman
Anterior uveitis with posterior synechiae:
Treatment:
- Topical corticosteroids (prednisolone acetate 1%)
- Cycloplegic agents (atropine, cyclopentolate) to prevent synechiae and relieve spasm
- Periocular/systemic steroids for severe or refractory cases
- Treat underlying cause
Fuchs Uveitis Syndrome (Fuchs Heterochromic Iridocyclitis - FHC/FUS)
- Chronic, low-grade, non-granulomatous uveitis; mean age 40 years
- Typically unilateral, more common in middle-aged women
- Characterized by: diffuse fine KP (stellate), loss of iris pigment epithelium causing heterochromia (affected eye is lighter), fine bridging vessels in the angle (bleed on paracentesis - Amsler sign)
- Complications: cataract (very common), secondary glaucoma
- Associated with CMV or rubella virus in many cases
- No synechiae (distinguishing feature)
3. Iris Tumours
Iris Naevus
- Circumscribed solitary flat or variably elevated pigmented lesion in the superficial stroma
- Disrupts normal iris architecture
- Diffuse naevus: occurs in congenital ocular melanocytosis and Cogan-Reese (ICE) syndrome
- Malignant transformation rate: up to 8% over 15 years
- Risk factors for malignancy: age <40, inferior location, bleeding, diffuse involvement, feathery margins, ectropion uveae
- Management: lifelong observation with slit lamp photography
Iris Freckle (Ephelis)
- Superficial, flat; no elevation or distortion of iris architecture
- Increased melanocyte pigmentation but normal cell number
- No malignant potential
Brushfield Spots
- Small whitish peripheral iris speckles in a concentric ring
- Classically associated with Down syndrome (trisomy 21), also normal in blue eyes
- Consist of focal hyperplasia surrounded by a ring of hypoplasia
- No malignant potential
Lisch Nodules
- Small well-defined bilateral iris nodules
- Pathognomonic of neurofibromatosis type 1 (NF1); present in >95% by second-third decade
- Hamartomas; no malignant potential
Lisch nodules - multiple small pigmented nodules on the iris surface:
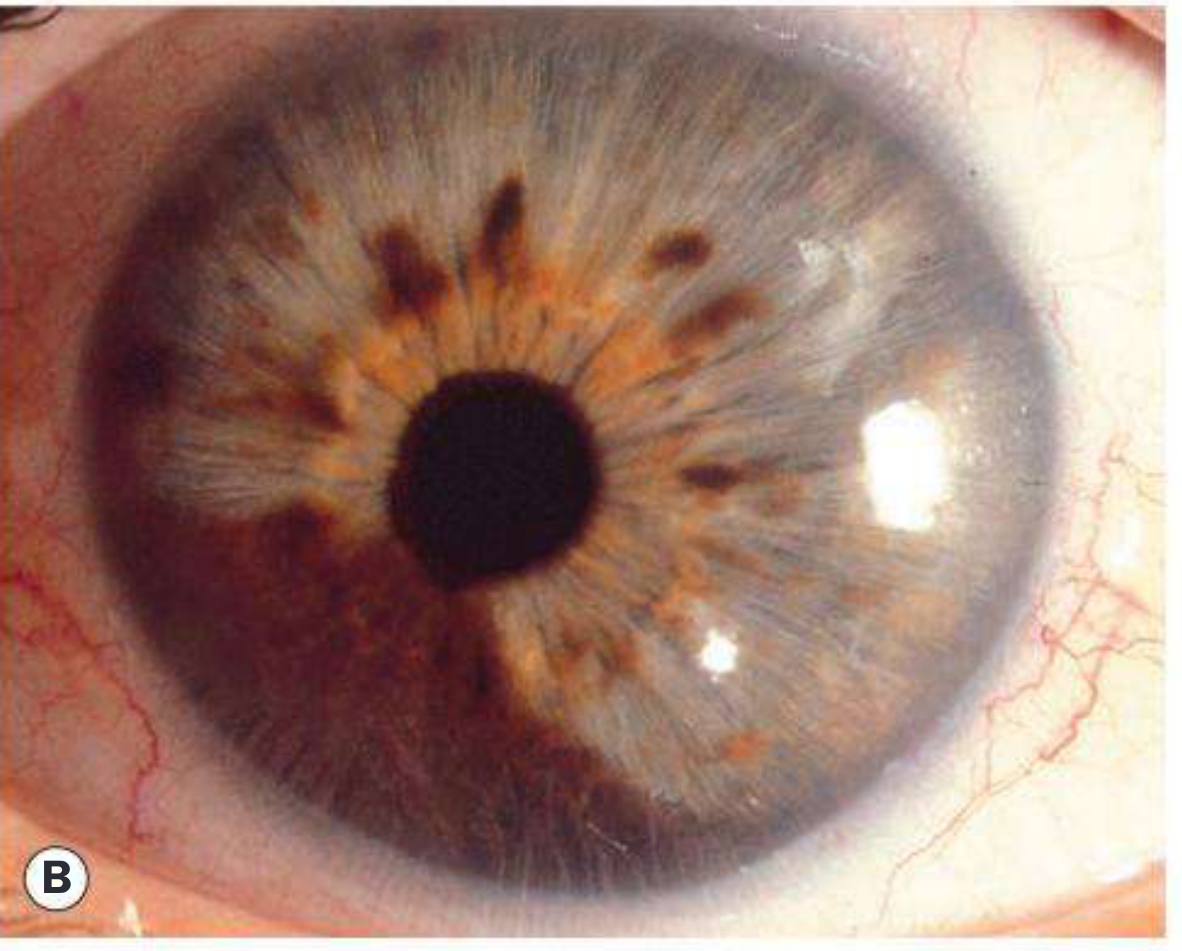
Iris Melanoma
- ~8% of all uveal melanomas; better prognosis than choroidal melanoma (~5% metastasis at 10 years)
- Risk factors: fair skin, light iris colour, atypical naevi, ocular melanocytosis, chronic UV/arc welding exposure
- Presentation: middle age (a decade earlier than choroidal melanoma); enlargement of pre-existing naevus
- Histology: diffusely infiltrating spindle cells (low-grade); epithelioid component = more aggressive
- Signs:
- Pigmented nodule ≥3 mm diameter, ≥1 mm thick, typically inferior half of iris
- Prominent surface blood vessels
- Pupillary distortion, ectropion uveae, localized cataract
- Rarely amelanotic
- Angle infiltration possible; extrascleral extension rare
- Complications: hyphaema, cataract, glaucoma
- Investigations: UBM (to rule out ciliary body involvement), fine-needle aspiration biopsy, systemic staging
- Treatment:
- Sector iridectomy (small tumours)
- Iridocyclectomy (angle involvement)
- Brachytherapy or proton beam radiotherapy
- Enucleation for diffuse tumours
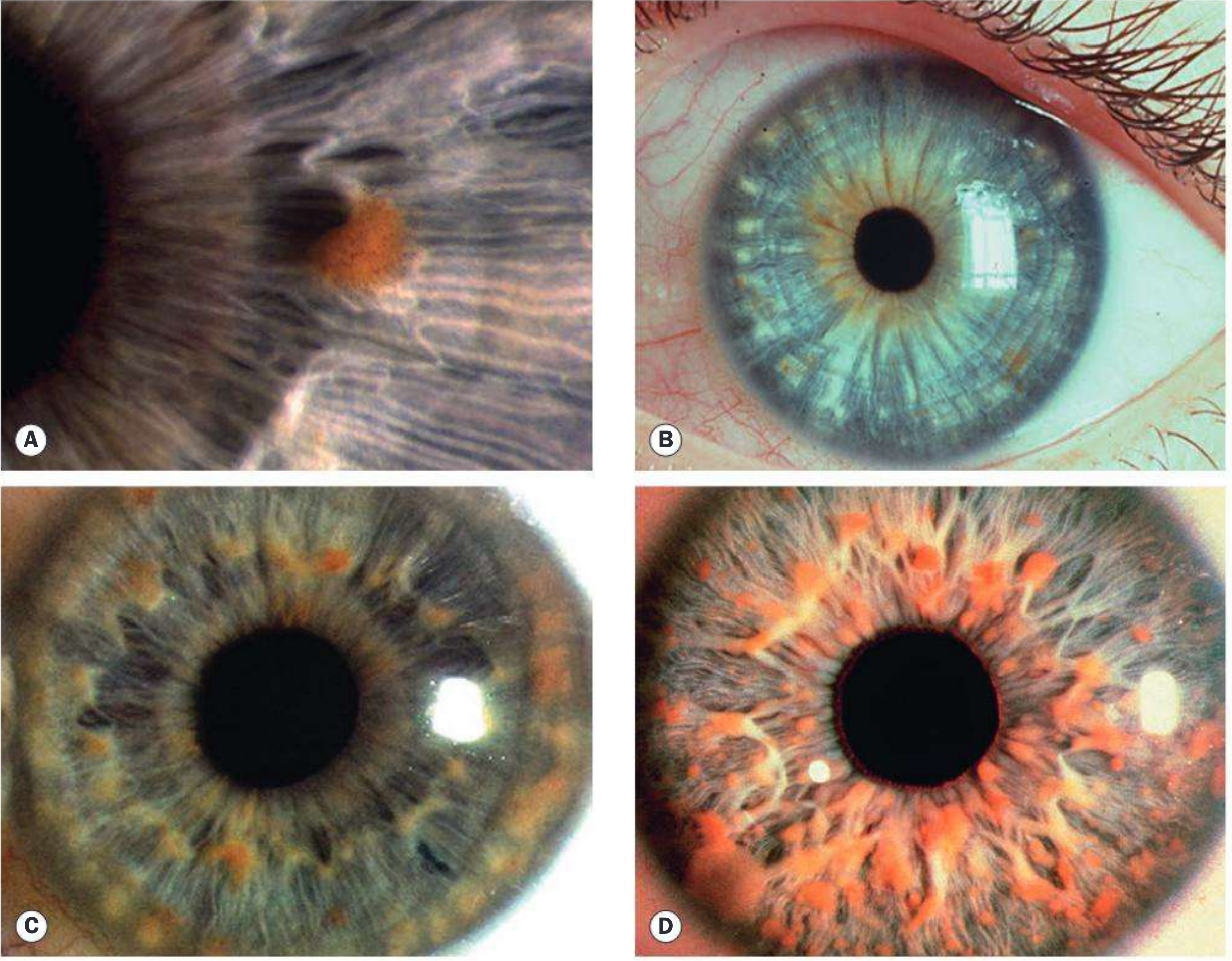
Iris melanoma - slit lamp views showing (A) histology with spindle cells, (B-C) pigmented nodules, (D) ectropion uveae:
Metastatic Tumours to the Iris
- Rare; fast-growing white/pink/yellow masses
- Associated with anterior uveitis and occasionally hyphaema
- Primary sites: breast, lung, cutaneous melanoma (most common)
Juvenile Xanthogranuloma (JXG)
- Rare idiopathic granulomatous disease of early childhood
- Iris involvement can cause spontaneous hyphaema - key clinical clue
- Yellow-orange lesions on iris
- Treated with topical/systemic steroids
4. Iris Cysts
Primary Epithelial Cysts
- Arise from iris/iridociliary pigment epithelium
- 75% peripheral iris - smooth dome-shaped bulging visible on gonioscopy
- May rarely dislodge to float freely in AC or vitreous
- Most are asymptomatic; large cysts causing vision obstruction treated with focal photocoagulation
Primary Stromal Cysts
- Solitary, unilateral, smooth translucent anterior wall on or within iris
- Congenital type (more aggressive): requires aspiration, surgical excision, or ethanol sclerosis
- May remain stable for years, then enlarge or spontaneously rupture
Secondary Cysts
- Traumatic: conjunctival/corneal epithelial implantation after penetrating injury or surgery; frequently enlarge, causing corneal oedema, uveitis, and glaucoma
- Miotic-induced: long-acting miotic drugs (e.g., echothiophate) cause bilateral, multiple small pupillary border cysts; prevented by concurrent phenylephrine 2.5%
- Parasitic: extremely rare
Anterior segment OCT and ultrasound biomicroscopy (UBM) are key tools to differentiate iris cysts from solid ciliary body tumours.
5. Iris Heterochromia
| Lighter Affected Iris | Darker Affected Iris |
|---|---|
| Congenital Horner syndrome | Ocular/oculodermal melanocytosis |
| Fuchs heterochromic iridocyclitis | Hemosiderosis / siderosis |
| Chronic uveitis | Retained intraocular foreign body |
| Juvenile xanthogranuloma | Uveal melanoma |
| Waardenburg syndrome | ICE syndrome |
| Metastatic carcinoma | Diffuse iris naevus |
6. Iris Lesion Classification (Wills Eye)
| Pigmentation | Differential Diagnosis |
|---|---|
| Melanotic (brown) | Naevus, melanoma, adenoma/adenocarcinoma of iris pigment epithelium |
| Amelanotic (white/yellow/orange) | Amelanotic melanoma, sarcoid/TB granuloma, neurofibroma, JXG, foreign body, cyst, leiomyoma, medulloepithelioma |
7. Iris Neovascularization (Rubeosis Iridis)
New vessels on the iris surface - a marker of ocular ischemia. Causes:
- Diabetic retinopathy (most common)
- Ocular ischemic syndrome
- Central or branch retinal vein/artery occlusion
- Chronic uveitis, chronic retinal detachment
- Intraocular tumours (retinoblastoma, melanoma)
Sources: Kanski's Clinical Ophthalmology - A Systematic Approach, 10th ed.; The Wills Eye Manual, 8th ed.
This is a shared conversation. Sign in to Orris to start your own chat.