Differences between papillary, follicular, medullary thyroid carcinoma
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, authoritative information to provide a thorough comparison. Let me compose the full answer.
Differences Between Papillary, Follicular, and Medullary Thyroid Carcinoma
Here is a comprehensive comparison across all major dimensions.
1. Cell of Origin
| Feature | Papillary (PTC) | Follicular (FTC) | Medullary (MTC) |
|---|---|---|---|
| Cell of origin | Follicular epithelial cells | Follicular epithelial cells | Parafollicular C cells (neuroendocrine) |
| Hormone produced | None (nonfunctional) | Rarely hyperfunctional | Calcitonin (+ somatostatin, serotonin, VIP) |
MTC is fundamentally different from PTC and FTC - it arises from C cells, not follicular epithelium, and is therefore a neuroendocrine tumor.
2. Epidemiology
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Frequency | Most common (~80% of thyroid cancers) | ~10-15% | ~5% |
| Peak age | Any age; commonest in 30s-40s | 40-60 years | Sporadic: 5th-6th decade; familial: younger, including children |
| Sex ratio | F > M | F > M (3:1) | Similar, slightly F > M |
| Familial | Rare | Rare | 30% familial (MEN 2A, MEN 2B, familial MTC) |
3. Risk Factors
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Ionizing radiation | Strong risk factor (esp. childhood) | Less association | No |
| Iodine deficiency | No significant link | More common in iodine-deficient areas | No |
| Genetic predisposition | RET/PTC rearrangements in radiation-associated | PAX8-PPARG rearrangement | Germline RET mutation (MEN 2A/2B) |
4. Molecular Genetics
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Key mutation | BRAF V600E (40-65%); RET/PTC rearrangements (10-20%); RAS (10-30%) | RAS mutations; PAX8-PPARG fusion t(2;3); PIK3CA gain-of-function; PTEN loss | RET point mutations (germline in familial; somatic in ~50% sporadic) |
| Pathway | MAPK pathway | PI3K/AKT pathway | RET tyrosine kinase constitutive activation |
All three mutations in PTC (BRAF, RET, RAS) are mutually exclusive since they have redundant effects on the MAPK pathway. - Robbins & Kumar Basic Pathology, p. 736
5. Gross and Microscopic Morphology
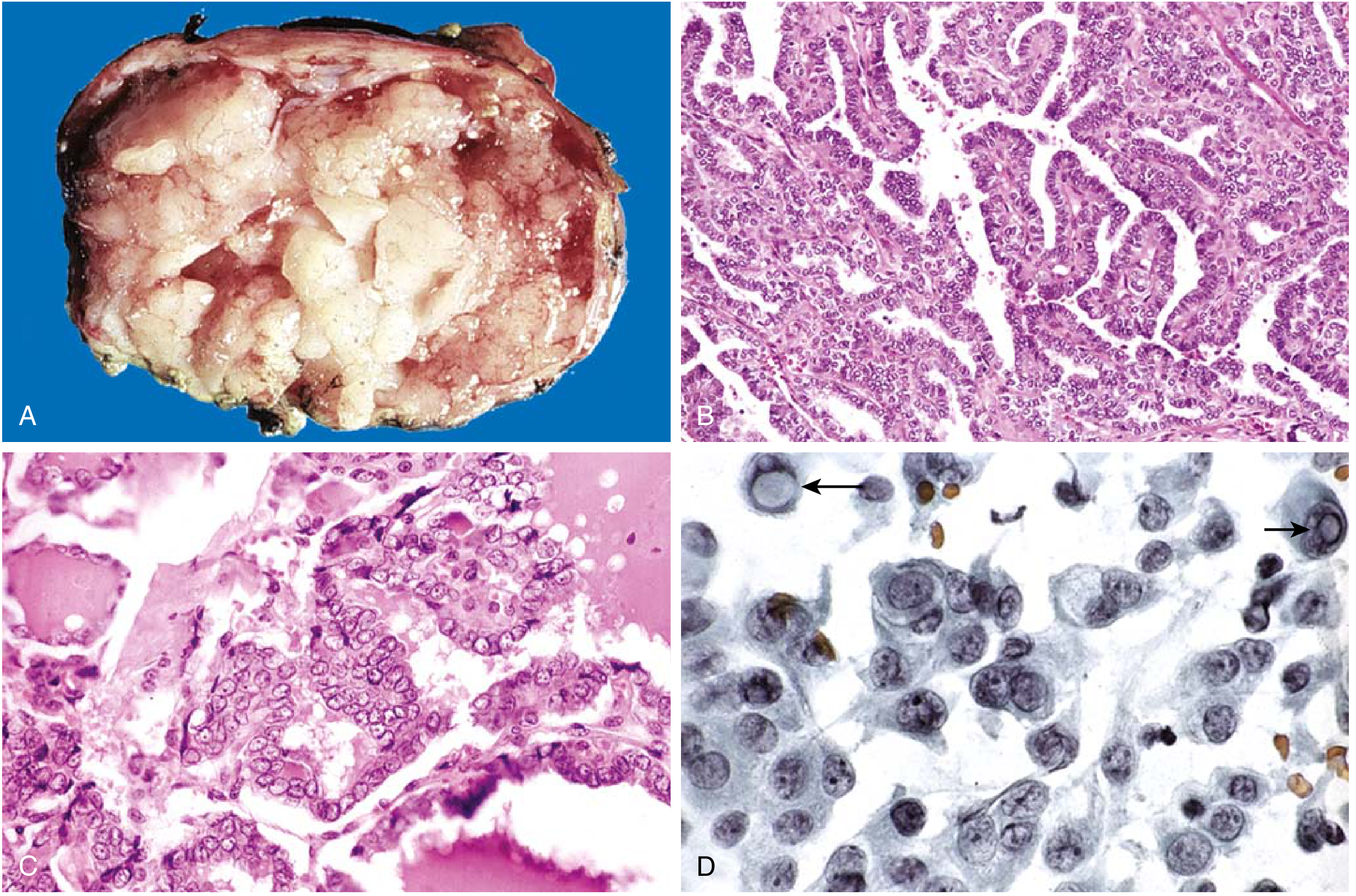
Papillary Thyroid Carcinoma
- Solitary or multifocal; may be encapsulated or infiltrative
- Branching papillae with fibrovascular stalks
- Hallmark nuclei: "ground-glass" / "Orphan Annie eye" nuclei (optically clear, empty chromatin), nuclear grooves, and pseudo-inclusions
- Psammoma bodies (concentrically calcified structures) - essentially pathognomonic; almost never seen in FTC or MTC
- Lymphatic invasion common; lymph node metastases in up to 50%
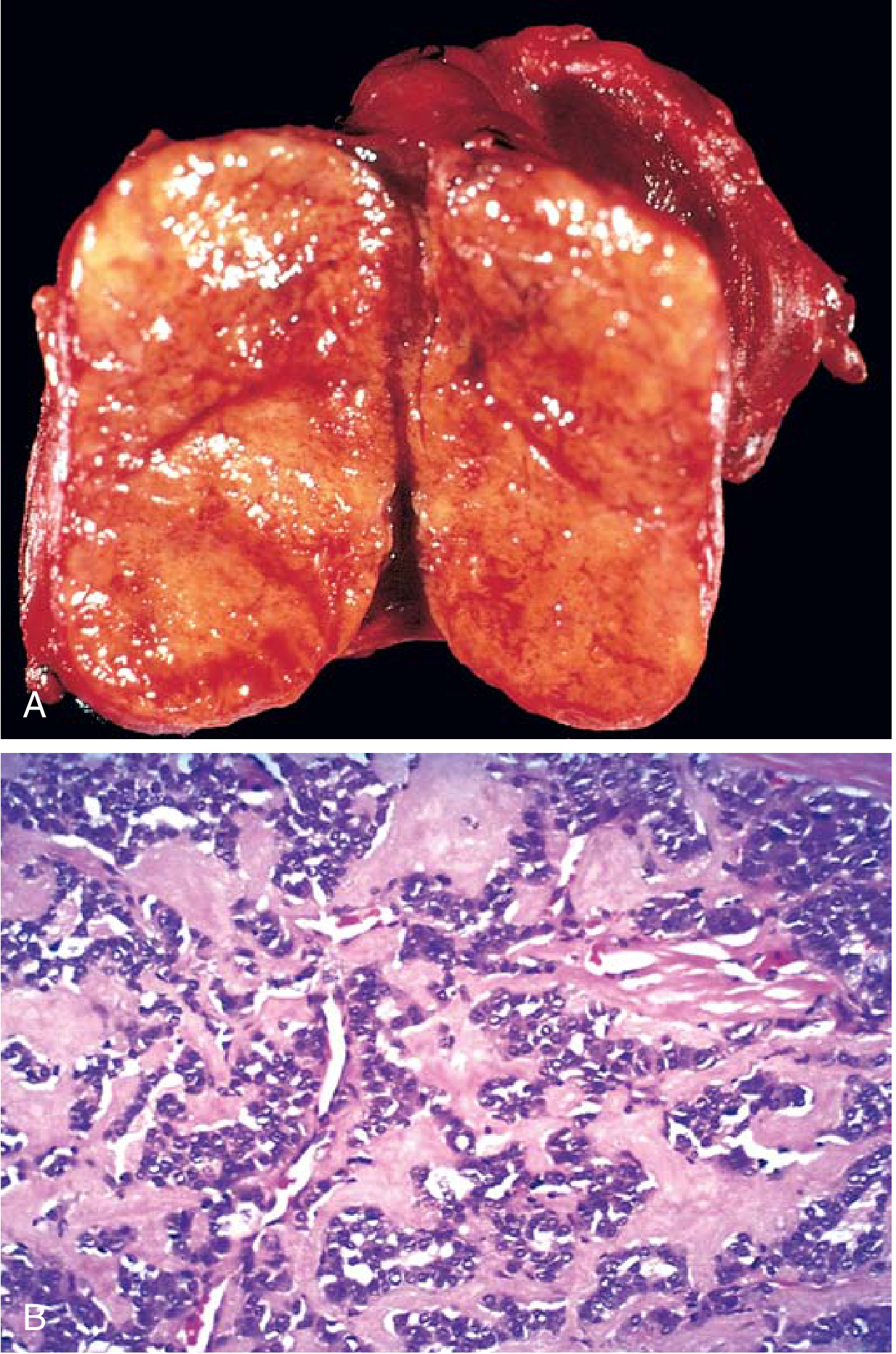
Follicular Thyroid Carcinoma
- Single nodule; may look grossly identical to a follicular adenoma
- Uniform cells forming small follicles resembling normal thyroid
- No psammoma bodies, no papillary nuclear features
- Diagnosis requires demonstration of capsular invasion and/or vascular invasion - extensive histologic sampling required
- Hematogenous spread to lungs, bone, liver (NOT lymph nodes typically)
Medullary Thyroid Carcinoma
- Solitary (sporadic) or bilateral/multicentric (familial)
- Polygonal to spindle-shaped cells in nests, trabeculae, or gland-like structures
- Amyloid deposits in the stroma (derived from altered calcitonin) - distinctive feature
- Multicentric C-cell hyperplasia in surrounding parenchyma is characteristic of familial cases (precursor lesion)
- Calcitonin demonstrable by immunohistochemistry in tumor cells and amyloid
6. Spread Pattern
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Lymphatic spread | Common (up to 50% cervical nodes) | Uncommon | Common - central and lateral neck nodes |
| Hematogenous spread | Uncommon | Common - lungs, bone, liver | Can occur (hepatic, skeletal) |
| Bilateral | Can be multifocal | Usually unilateral | Bilateral in familial cases |
7. Tumor Marker
| PTC | FTC | MTC |
|---|---|---|
| Thyroglobulin (post-op surveillance) | Thyroglobulin (post-op surveillance) | Calcitonin (diagnosis + post-op follow-up); CEA also elevated |
Calcitonin measurement is central to MTC diagnosis and follow-up. Elevated serum calcitonin provides a marker of residual or recurrent disease. - Harrison's Principles of Internal Medicine 22E
8. Radioiodine (RAI) Uptake
| PTC | FTC | MTC |
|---|---|---|
| Yes (if well-differentiated) | Yes (well-differentiated metastases may take up RAI - useful for ablation) | No - MTC does not arise from follicular cells, so no RAI uptake |
9. Clinical Presentation
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Presentation | Painless neck mass; incidental on imaging | Solitary cold nodule | Neck mass ± compressive symptoms (dysphagia, hoarseness) |
| Paraneoplastic | None | Rarely hyperfunctional | Diarrhea (VIP secretion); Cushing's syndrome (ACTH) |
| Association | Prior radiation | Iodine deficiency, goiter | MEN 2A (pheo + hyperparathyroidism), MEN 2B (pheo + mucosal neuromas + marfanoid habitus) |
10. Prognosis
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| 10-year survival | >95% (excellent) | Minimally invasive: >90%; Widely invasive: ~50% | Sporadic: ~80% if localized; metastatic: ~20% at 10 years |
| Lymph node mets effect | Isolated nodal mets do NOT significantly worsen prognosis | Rare; less impact | Significant prognostic impact |
| Overall | Most indolent | Intermediate | More aggressive than PTC/FTC |
11. Treatment
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Surgery | Total thyroidectomy ± lymph node dissection | Total thyroidectomy | Total thyroidectomy + central neck dissection (bilateral central if evident MTC) |
| Radioiodine | Yes (post-op ablation) | Yes (well-differentiated metastases) | Not used |
| TSH suppression | Yes (levothyroxine) | Yes | Not applicable |
| Targeted therapy | BRAF inhibitors (for BRAF-mutated advanced disease) | None established | Vandetanib, cabozantinib, selpercatinib (most selective RET inhibitor) for advanced/metastatic disease |
| Prophylactic thyroidectomy | Not applicable | Not applicable | Offered to RET mutation carriers (age <1-5 years depending on mutation risk) |
| Screening family members | Not routine | Not routine | Mandatory - RET genetic testing + calcitonin screening |
Quick Summary Table
| Feature | PTC | FTC | MTC |
|---|---|---|---|
| Origin | Follicular epithelium | Follicular epithelium | C cells (neuroendocrine) |
| Frequency | 80% | 10-15% | 5% |
| Key mutation | BRAF V600E | RAS, PAX8-PPARG | RET |
| Nuclear hallmark | Ground-glass nuclei, grooves, pseudo-inclusions | None (follicular pattern) | N/A |
| Psammoma bodies | Yes | No | No |
| Amyloid stroma | No | No | Yes |
| Tumor marker | Thyroglobulin | Thyroglobulin | Calcitonin |
| RAI uptake | Yes | Yes | No |
| Metastasis route | Lymphatic (cervical nodes) | Hematogenous (lung, bone) | Both |
| Familial | Rare | Rare | 30% (MEN 2A/2B) |
| Prognosis | Excellent (>95% 10-yr) | Intermediate | Worse (20% at 10yr if metastatic) |
Sources: Robbins & Kumar Basic Pathology, pp. 735-740; Harrison's Principles of Internal Medicine 22E, pp. 767-771, 3129; Quick Compendium of Clinical Pathology 5th ed., p. 415
This is a shared conversation. Sign in to Orris to start your own chat.