Teach me yolksac tumour
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
"yolk sac tumor" AND (diagnosis OR treatment)
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full teaching answer.
Yolk Sac Tumor (Endodermal Sinus Tumor)
Overview
Yolk sac tumor (YST) - also called endodermal sinus tumor - is a malignant germ cell tumor (GCT) derived from primitive germ cells that differentiate along the extraembryonic yolk sac lineage. It occurs in the testis, ovary, and extragonadal sites (mediastinum, retroperitoneum, pineal gland).
Classification by Age and Site
| Setting | Key Facts |
|---|---|
| Prepubertal testis | Most common testicular tumor in children up to 3 years; usually pure; excellent prognosis |
| Postpubertal testis | Rarely pure; usually mixed with embryonal carcinoma or other GCT elements; associated with germ cell neoplasia in situ (GCNIS) |
| Ovary | Second most common malignant ovarian GCT (after dysgerminoma); affects children and young women |
| Extragonadal | Mediastinum, retroperitoneum, pineal gland; may occur in adults |
Pathogenesis
- Derived from malignant germ cells differentiating along the extraembryonic yolk sac lineage
- Postpubertal tumors arise from germ cell neoplasia in situ (GCNIS) - the precursor lesion for most adult GCTs; prepubertal tumors do NOT have this association
- RUNX3 gene hypermethylation and GATA-4 overexpression are implicated in the pathogenesis of ovarian YST
- Postpubertal tumors frequently have isochromosome 12p [i(12p)], shared with other adult GCTs
Histological Features (The Core of Diagnosis)
Growth Patterns (multiple, variable):
- Reticular (lace-like) pattern - most common; loose network of medium-sized cuboidal, flattened, or spindled cells with less cytologic atypia than embryonal carcinoma
- Papillary pattern
- Solid cords
- Microcystic / glandular pattern
- Embryoid bodies (resemble 1-2 week embryos, surrounded by syncytio- and cytotrophoblasts)
Pathognomonic Structures:
Schiller-Duval Bodies - present in ~50% of cases
- A glomerulus-like structure: central blood vessel (capillary) enveloped by tumor cells within a space that is also lined by tumor cells
- Resembles a primitive glomerulus or endodermal sinus
- Composed of a mesodermal core with a visceral and parietal layer of cells
Eosinophilic Hyaline Globules
- Intracellular and extracellular, eosinophilic, hyaline-like globules
- Present in up to 84% of cases
- Contain AFP and alpha-1-antitrypsin; stain positive by immunoperoxidase
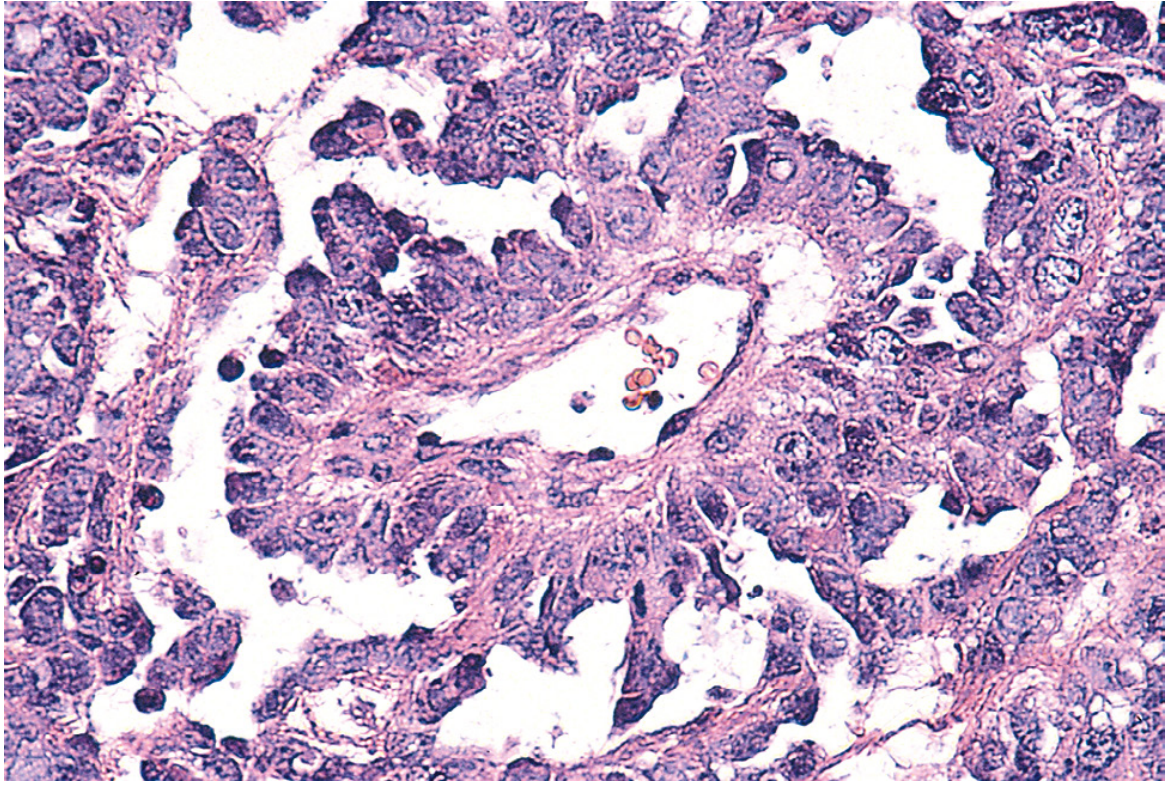
Here is the classic histology showing Schiller-Duval bodies:
Immunohistochemistry / Markers
| Marker | Result | Notes |
|---|---|---|
| AFP (alpha-fetoprotein) | Positive | Near universal; serum AFP is the key tumor marker |
| Glypican-3 | Positive | Characteristic |
| Keratin (cytokeratin) | Positive | |
| SALL4 | Positive | Pan-germ cell marker |
| HCG | Negative | Key distinction from choriocarcinoma |
| OCT3/4 | Negative | Distinguishes from embryonal carcinoma and seminoma |
| Alpha-1-antitrypsin | Positive (in globules) |
Key rule: YST always produces AFP but NOT HCG. This is diagnostically critical.
Clinical Presentation
Testicular YST:
- Prepubertal: painless testicular mass in infant/toddler (< 3 years); serum AFP elevated (but note AFP is physiologically high in neonates, interpret with age-adjusted norms)
- Postpubertal/Adult: testicular mass, often part of mixed GCT; markedly elevated serum AFP
Ovarian YST:
- Children and young women
- Abdominal pain and rapidly growing pelvic mass involving a single ovary
- Elevated serum AFP
Extragonadal YST:
- Mediastinum (most common extragonadal site in adults), retroperitoneum, pineal gland
- Elevated AFP
Staging and Prognosis
Ovarian YST (combination chemotherapy era):
- Stage I-II: >95% 5-year survival
- Stage III: ~70% 5-year survival
- Stage IV: ~50% 5-year survival
Prepubertal testicular YST: Very good prognosis after orchiectomy; many stage I patients cured without chemotherapy.
Postpubertal testicular YST: Prognosis depends on IGCCCG risk category (AFP levels used in staging - AFP >10,000 ng/mL = poor risk).
Comparison: Prepubertal vs. Postpubertal YST
| Feature | Prepubertal | Postpubertal |
|---|---|---|
| Age | Infants/children (<3 yr) | Teens/adults |
| Purity | Usually pure | Usually mixed |
| GCNIS precursor | NO | YES |
| i(12p) | No | Yes |
| Prognosis | Excellent | Intermediate |
| AFP | Elevated (interpret with age norms) | Elevated |
Differential Diagnosis
| Tumor | Key Distinction |
|---|---|
| Embryonal carcinoma | OCT3/4+, more cytologic atypia, AFP low/absent |
| Seminoma / Dysgerminoma | OCT3/4+, KIT+, AFP negative |
| Choriocarcinoma | HCG markedly elevated, AFP negative |
| Clear cell carcinoma (ovary) | Older women, no AFP elevation |
Treatment
- Radical orchiectomy / salpingo-oophorectomy - primary surgery
- Chemotherapy: BEP (Bleomycin, Etoposide, Cisplatin) - backbone of treatment for advanced disease
- Surveillance vs. adjuvant chemotherapy based on stage for prepubertal testicular YST
- AFP monitoring - used for treatment response and relapse detection
High-Yield Summary for Exams
- Also called: Endodermal sinus tumor
- Most common testicular tumor in children < 3 years
- Second most common malignant ovarian GCT
- Key histology: Schiller-Duval bodies + eosinophilic hyaline globules
- Key marker: AFP positive, HCG negative
- IHC: AFP, glypican-3, keratin, SALL4 positive; OCT3/4 negative
- Prepubertal = no GCNIS, no i(12p), excellent prognosis
- Postpubertal = associated with GCNIS, usually mixed, AFP used in IGCCCG staging
- Treatment: BEP chemotherapy for advanced stages
Sources:
- Robbins & Cotran Pathologic Basis of Disease - Chapters on Testicular and Ovarian GCTs
- Campbell-Walsh-Wein Urology, Germ Cell Tumors of the Testis
- Smith and Tanagho's General Urology, 19th Edition
- Recent evidence: Hepatic YST systematic review (2025) and mediastinal YST meta-analysis (2024) confirm no major changes to existing clinical framework; BEP-based chemotherapy remains standard.
This is a shared conversation. Sign in to Orris to start your own chat.