Wernickes aphasia
Reading File
Finding Sources
Searching PubMed
"Wernicke aphasia"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive, high-quality content from four major neurology textbooks plus an MRI image. Here is the full answer:
Wernicke's Aphasia
Definition and Historical Background
Wernicke's aphasia is a fluent aphasia resulting from damage to the posterior perisylvian region of the dominant (left) hemisphere. It was first described by Carl Wernicke in 1874, who showed that a lesion in the posterior superior temporal lobe produced a syndrome distinct from Broca's aphasia - speech was preserved in terms of flow and melody, but comprehension was lost. It is also called receptive aphasia, sensory aphasia, or posterior aphasia, though each of these terms has limitations (e.g., expression is also impaired, not just reception).
- Bradley and Daroff's Neurology in Clinical Practice, p. 209
- Adams and Victor's Principles of Neurology, 12th Ed., p. 509
Neuroanatomical Basis
Wernicke's area is classically located in the posterior part of the left superior temporal gyrus (area 22, planum temporale), adjacent to the primary auditory cortex. The full lesion in Wernicke's aphasia typically involves a larger zone - the posterior perisylvian region - encompassing:
- Posterior superior temporal gyrus
- Supramarginal gyrus
- Angular gyrus
- Posterior insular gyrus
The most common cause is embolic occlusion of the inferior (lower) division of the left middle cerebral artery (MCA). Other causes include hemorrhage, tumor, abscess (e.g., herpes encephalitis), or extension of putaminal/thalamic hemorrhage.
The lesion also disconnects Wernicke's area from Broca's area via the arcuate fasciculus, explaining the impaired repetition.
Adams and Victor, p. 510; Neuroanatomy Through Clinical Cases, 3rd Ed.
MRI Example
Below: Axial and coronal MRI (A, B) of an elderly woman with Wernicke's aphasia showing a large left superior temporal lobe lesion. A PET scan was used to confirm reduced metabolism consistent with stroke rather than tumor.
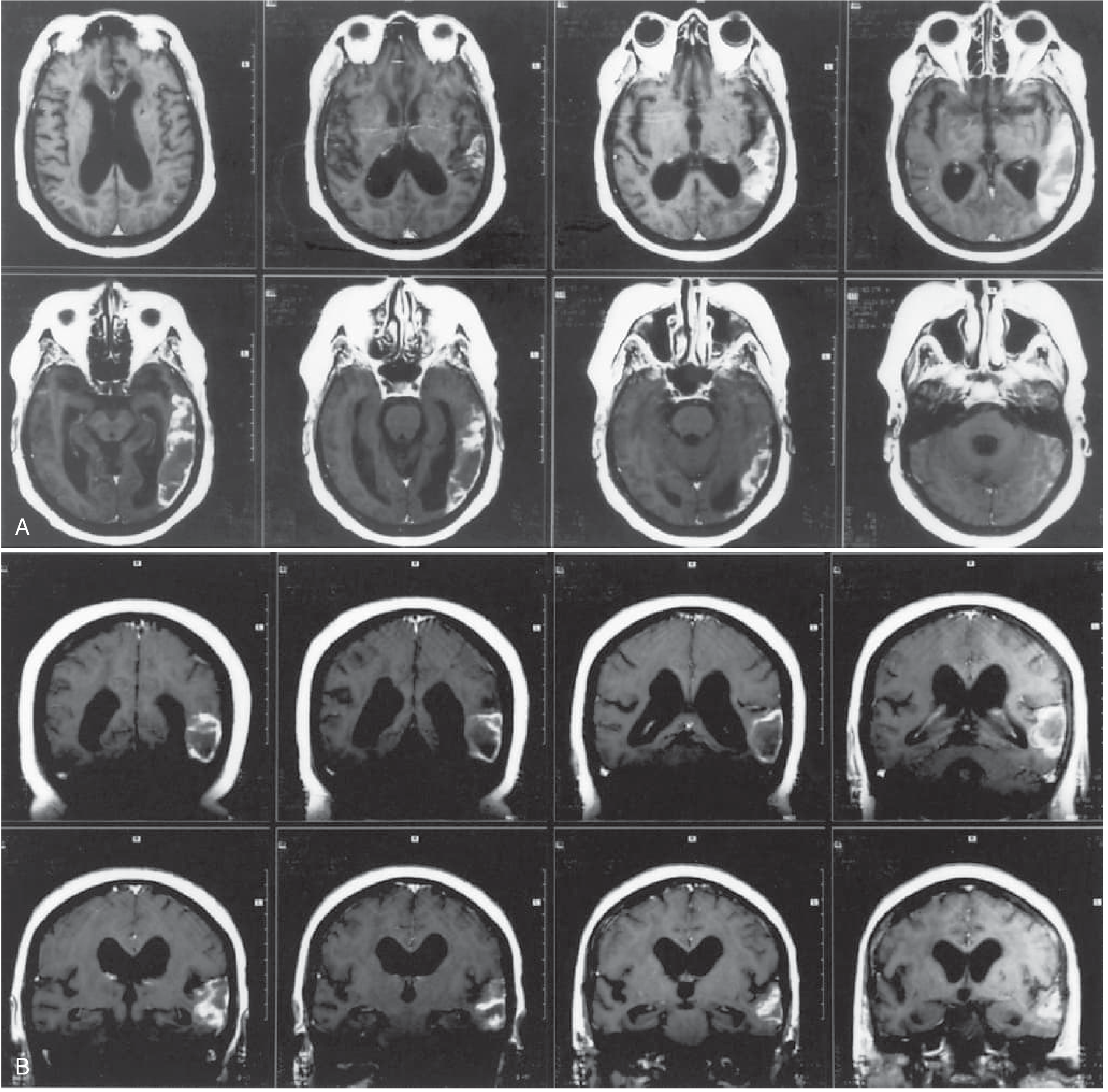
Bradley and Daroff's Neurology, Fig. 13.4
Core Clinical Features
1. Spontaneous Speech - Fluent but Empty
- Speech flows effortlessly at normal or even excessive rate (logorrhea)
- Normal prosody (melody/intonation) and grammatical structure
- However, speech is devoid of meaning - full of paraphasic errors
Types of paraphasias:
| Type | Description | Example |
|---|---|---|
| Verbal / Semantic paraphasia | One word substituted for another of similar meaning | "ink" instead of "pen"; "The grass is blue" |
| Literal / Phonemic paraphasia | Wrong phoneme or syllable substituted | "The grass is greel"; "pish" instead of "fish" |
| Neologism | Non-words invented by the patient | "The grass is grumps"; "tarripoi" |
| Jargon aphasia | Extreme form - speech becomes entirely incomprehensible gibberish |
2. Comprehension - Severely Impaired
- Cannot follow spoken commands (except possibly axial commands: "close your eyes," "stick out your tongue")
- Cannot read with comprehension (alexia)
- A few simple commands may still be executed in mild cases
3. Repetition - Impaired
This is a key distinguishing feature from transcortical sensory aphasia, where repetition is intact.
4. Naming - Impaired
Frequent paraphasic errors or entirely irrelevant responses when asked to name objects.
5. Reading and Writing - Both Impaired
- Reading: fluent aloud but without comprehension; paragraphic
- Writing: well-formed letters but with paragraphic and spelling errors; more abnormal than oral speech in some patients
Bedside Features Summary (Table)
| Feature | Finding |
|---|---|
| Spontaneous speech | Fluent, paraphasic, often logorrhoeic |
| Naming | Impaired (bizarre paraphasic misnaming) |
| Comprehension | Impaired |
| Repetition | Impaired |
| Reading | Impaired for comprehension |
| Writing | Well-formed but paragraphic, spelling errors |
| Motor/sensory deficits | Usually absent |
| Associated signs | ± Right homonymous hemianopia (upper quadrant > full) |
Bradley and Daroff's, Table 13.2
Associated Neurological Signs
- Right homonymous hemianopia (upper quadrantanopia especially) - due to involvement of the lower (temporal) portion of the optic radiation
- No hemiparesis - the motor cortex and corticospinal tract are spared, which is why these patients are often misdiagnosed as psychotic or confused
- Apraxia - may be present but difficult to test due to impaired comprehension
- Elements of Gerstmann syndrome - if the lesion extends to the supramarginal and angular gyri (agraphia, acalculia, finger agnosia, left-right disorientation)
Behavioral / Psychiatric Features
In sharp contrast to Broca's aphasia (where patients are typically depressed and frustrated), Wernicke's aphasics:
- Are often unaware of their deficit (anosognosia) - they appear to carry on a "normal" conversation
- May become angry or paranoid when others cannot understand them
- Do not typically show depression
- Can be misdiagnosed as schizophrenia or acute psychosis due to the jargon speech and lack of insight
Classic example from Neuroscience: Exploring the Brain: A patient asked "What brings you to hospital?" replied with a rapid, fluent, but incoherent stream: "Boy, I'm sweating, I'm awful nervous, you know, once in a while I get caught up, I can't mention the tarripoi, a month ago, quite a little, I've done a lot well..." - The speech sounds superficially normal in rhythm and flow but is largely meaningless.
Differential Diagnosis
| Condition | Fluency | Comprehension | Repetition | Key Differentiator |
|---|---|---|---|---|
| Wernicke's aphasia | Fluent | Impaired | Impaired | Posterior lesion; paraphasic output |
| Broca's aphasia | Non-fluent | Relatively intact | Impaired | Anterior lesion; hemiparesis |
| Transcortical sensory aphasia | Fluent | Impaired | Intact | Repetition spared |
| Conduction aphasia | Fluent | Relatively intact | Markedly impaired | Arcuate fasciculus lesion |
| Global aphasia | Non-fluent | Impaired | Impaired | Large MCA territory; hemiplegia |
| Acute psychosis | Normal | Intact | Intact | No lesion on imaging; insight varies |
Prognosis and Persistence
- Wernicke's aphasia caused by small embolic strokes may improve substantially over weeks to months
- Persistence is associated with lesions involving both the supramarginal and angular gyri
- Causes with better prognosis: cerebral trauma, compression from edema, herpes encephalitis (if treated early), metabolic derangements
- Rehabilitation is often hindered by the patient's lack of awareness of their deficits
Adams and Victor, p. 510
Sources:
- Bradley and Daroff's Neurology in Clinical Practice, p. 208-210
- Adams and Victor's Principles of Neurology, 12th Ed., pp. 509-510
- Neuroanatomy Through Clinical Cases, 3rd Ed., Ch. 19.5
- Neuroscience: Exploring the Brain, 5th Ed., pp. 1818-1819
- Kandel's Principles of Neural Science, 6th Ed., p. 1431-1432
Bell mangendies law mbbs 1st year ohysio short note
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
I have excellent textbook content and diagrams. Here is the complete short note:
Bell-Magendie Law - Short Note (MBBS 1st Year Physiology)
Definition
Bell-Magendie Law states that:
The ventral (anterior) roots of the spinal cord are motor (efferent), and the dorsal (posterior) roots are sensory (afferent).
Historical Background
- Around 1810, Scottish physician Charles Bell and French physiologist François Magendie independently investigated the functional difference between the two roots of spinal nerves.
- Bell showed that cutting only the ventral roots caused muscle paralysis (loss of movement) without loss of sensation.
- Magendie showed that cutting only the dorsal roots caused loss of sensation without loss of movement.
- Together they concluded that within each peripheral nerve, motor and sensory fibers are bundled together, but they are anatomically segregated at the point where they attach to the spinal cord.
Neuroscience: Exploring the Brain, 5th Ed., p. 117-118
Anatomical Basis
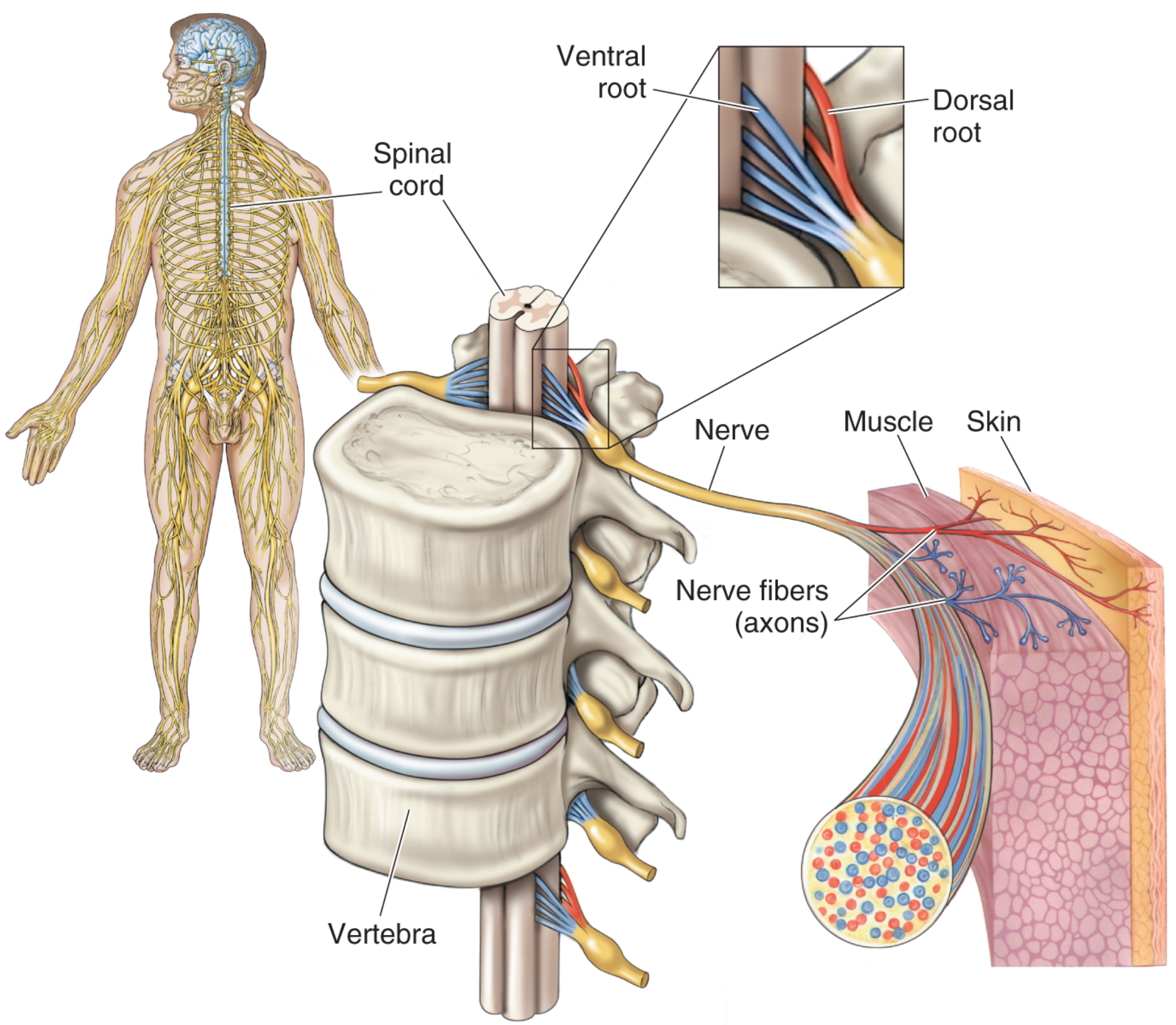
Fig 1.9 - Spinal nerves and roots. Blue fibers = motor (ventral root); Red fibers = sensory (dorsal root). Both are bundled together in the peripheral nerve but segregate at the spinal cord.
| Feature | Dorsal (Posterior) Root | Ventral (Anterior) Root |
|---|---|---|
| Function | Sensory (Afferent) | Motor (Efferent) |
| Direction | Carries impulses into spinal cord | Carries impulses out of spinal cord |
| Cell bodies | In Dorsal Root Ganglion (DRG) - outside spinal cord | In Anterior horn of spinal cord gray matter |
| Fiber type | Afferent (sensory) axons | Efferent (motor) axons |
| Effect of cutting | Loss of sensation | Loss of movement (paralysis) |
| Relative thickness | Thicker (2x the motor root) | Thinner |
Key Points to Remember
- Dorsal = Sensory (D for Dorsal, also for "Data coming in")
- Ventral = Motor (V for Ventral, also for "Voluntary movement out")
- The dorsal root ganglion (DRG) contains the cell bodies of sensory neurons - it is a swelling visible on the dorsal root before it enters the spinal cord.
- Motor neuron cell bodies lie in the anterior (ventral) horn of the spinal cord gray matter.
- The two roots unite just distal to the DRG to form a mixed spinal nerve - which is why cutting a peripheral nerve causes both motor and sensory loss in that region.
- There are 31 pairs of spinal nerves (8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal), each with a dorsal and ventral root.
Clinical Relevance
| Condition | Root Affected | Consequence |
|---|---|---|
| Posterior column disease (e.g., tabes dorsalis) | Dorsal roots | Loss of proprioception, vibration, touch - no weakness |
| Poliomyelitis | Anterior horn cells (ventral root origin) | Flaccid paralysis - no sensory loss |
| Dorsal rhizotomy (surgical procedure) | Dorsal roots cut | Used to relieve chronic pain or spasticity |
| Ventral rhizotomy | Ventral roots cut | Used to treat severe spasticity |
| Disc herniation | Compresses dorsal root/DRG | Radicular pain + sensory loss in a dermatomal distribution |
Mnemonic
"SAME DAVE"
- Sensory = Afferent = Dorsal
- Motor = Efferent = Ventral (and Exiting)
Or simply: "Don't Mess with Sensory Dorsally, Motor Ventrally"
Sources: Neuroscience: Exploring the Brain, 5th Ed., pp. 117-118, 577; Neuroanatomy Through Clinical Cases, 3rd Ed.; Langman's Medical Embryology
Cerebellar ataxia physiology mbbs 1st year / reference: AK JAIN
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Guyton & Hall (the standard physiology reference used alongside AK Jain for MBBS 1st year) covering all aspects needed. Let me now compile the complete short note.
Cerebellar Ataxia - Short Note (MBBS 1st Year Physiology)
Reference: AK Jain / Guyton & Hall Medical Physiology
Definition
Ataxia (from Greek: "without order") is a disturbance in the smooth performance of voluntary motor acts, resulting in muscular incoordination - movements that are abnormal in rate, range, timing, direction, and force.
Cerebellar ataxia specifically refers to incoordination caused by cerebellar dysfunction. It is the "cerebellar sign par excellence."
The cerebellum is called a "silent area" - its excitation causes no sensation, but its removal causes highly abnormal movements.
- Guyton & Hall Textbook of Medical Physiology
Role of the Cerebellum (Normal Function)
The cerebellum acts as a comparator and error-correcting device:
- Receives intended movement signals from the cerebral motor cortex
- Receives actual movement feedback via proprioceptive/sensory pathways from the periphery
- Compares the two - if they don't match, sends corrective signals back to the motor system
- Helps sequence and monitor motor activities in real time
- Plans the next movement a fraction of a second before the current one finishes
- Learns by mistakes - adjusts excitability of cerebellar neurons for future movements
Anatomical Basis - Three Functional Zones
| Zone | Region | Function | Lesion Effect |
|---|---|---|---|
| Vestibulocerebellum | Flocculonodular lobe + adjacent vermis | Equilibrium and postural control | Truncal ataxia, gait unsteadiness, nystagmus |
| Spinocerebellum | Vermis + intermediate zone | Coordination of distal limb movements (hands, fingers) | Limb ataxia (ipsilateral) |
| Cerebrocerebellum | Lateral hemispheres | Planning of sequential voluntary movements with cerebral cortex | Decomposition of movement, dysmetria |
Key rule: Cerebellar lesions cause IPSILATERAL signs (unlike upper motor neuron lesions which are contralateral).
Features / Signs of Cerebellar Ataxia
1. Hypotonia
- Decreased muscle tone on the side of the lesion
- Due to loss of tonic facilitatory signals from deep cerebellar nuclei (dentate, interposed) to motor cortex and brainstem motor nuclei
- Pendular knee jerk on testing
2. Dysmetria
- Inability to judge distance and stop a movement at the right point
- Movement overshoots (hypermetria) or undershoots (hypometria) the target
- The cerebellum cannot predict how far a movement will go
- Finger-nose test and heel-shin test demonstrate this
3. Past-Pointing (Hypermetria)
- Hand/limb moves beyond the intended mark when reaching for an object
- A manifestation of dysmetria - cerebellum is not initiating the "stop signal" in time
4. Dysdiadochokinesia
- Inability to perform rapid alternating movements
- e.g., rapidly pronating and supinating the hand
- The motor control system "loses track" of the limb position during fast movements
- Results in jumbled, disorganized movements instead of smooth alternation
5. Dysarthria (Scanning/Staccato Speech)
- Failure of progression in talking
- Speech muscles (larynx, mouth, respiratory system) are uncoordinated
- Results in slurred, jerky, explosive speech - some syllables loud, some weak, irregular rhythm
- Also called cerebellar dysarthria
6. Intention Tremor
- Tremor that appears on voluntary movement (unlike resting tremor of Parkinsonism)
- Oscillating, rhythmic tremor that worsens as the target is approached
- Best seen on finger-nose test
- Due to failure of damping oscillations in the feedback control loop
7. Nystagmus
- Rhythmic oscillation of the eyeballs, especially on lateral gaze
- Occurs due to failure of cerebellar damping of eye movement control
- Most prominent with flocculonodular lobe lesions
- Gaze-evoked nystagmus is most common type
8. Ataxic Gait (Cerebellar / Drunken Gait)
- Wide-based, staggering, unsteady gait
- Patient walks as if intoxicated / drunk
- Falls to the side of the lesion (ipsilateral)
- Midline (vermis) lesions: truncal ataxia - falls in any direction
- Lateral hemisphere lesions: falls toward the affected side
9. Rebound Phenomenon (Loss of Check Reflex)
- When a resisted movement is suddenly released, the limb flies past the intended position
- Normally the cerebellum activates antagonist muscles to "check" the movement
- In cerebellar lesions, this checking mechanism is absent
10. Decomposition of Movement
- Complex movements are broken down into their component parts
- Performed in a jerky, sequential (robotic) fashion instead of as smooth coordinated acts
Summary Table of Signs
| Sign | Test | Mechanism |
|---|---|---|
| Hypotonia | Passive movement, pendular knee jerk | Loss of deep nuclei facilitation |
| Dysmetria | Finger-nose, heel-shin test | Cannot predict movement termination |
| Past-pointing | Point to examiner's finger | Hypermetria - no stop signal |
| Dysdiadochokinesia | Rapid alternating hand movements | Loses position sense during fast movement |
| Intention tremor | Finger-nose test | Oscillating feedback loop |
| Dysarthria | Ask patient to speak | Uncoordinated speech muscles |
| Nystagmus | Lateral gaze | Failure of eye movement damping |
| Ataxic gait | Walk in a straight line | Wide-based, unsteady, ipsilateral falls |
| Rebound | Holmes rebound test | Absent antagonist check |
Mnemonic for Cerebellar Signs: "DANISH"
- D - Dysdiadochokinesia
- A - Ataxia (gait)
- N - Nystagmus
- I - Intention tremor
- S - Slurred (scanning) speech
- H - Hypotonia
Important Points for Exams
- Cerebellar signs are always ipsilateral to the lesion
- No paralysis, no sensory loss - purely motor coordination deficit
- Cerebellar ataxia is worse with eyes open (unlike sensory/posterior column ataxia which is worse with eyes closed - positive Romberg's sign)
- Romberg's sign is NEGATIVE in cerebellar ataxia (patient unsteady with both eyes open and closed, not specifically worse when eyes closed)
- Deep cerebellar nuclei (especially the dentate nucleus) must be involved for significant persistent symptoms
- The cerebellum also has nonmotor functions - cognitive, emotional (cerebellar cognitive affective syndrome / Schmahmann syndrome)
Sources: Guyton & Hall Textbook of Medical Physiology (closest standard to AK Jain's physiology coverage); Bradley & Daroff's Neurology in Clinical Practice; Neuroanatomy Through Clinical Cases, 3rd Ed.; Localization in Clinical Neurology, 8th Ed.
Sensori-neural hearing loss physiology mbbs 1st year / reference: AK JAIN
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed from Guyton & Hall, Ganong, and specialized ear surgery texts. Here is the complete MBBS 1st year physiology short note:
Sensorineural Hearing Loss (SNHL)
Short Note - MBBS 1st Year Physiology
Reference: AK Jain / Guyton & Hall / Ganong's Medical Physiology
Definition
Sensorineural hearing loss (SNHL) - also called nerve deafness - is hearing loss caused by damage to:
- The cochlea (hair cells / organ of Corti) - "sensory" component
- The auditory (cochlear) division of CN VIII - "neural" component
- Central auditory pathways (brainstem / auditory cortex)
SNHL accounts for approximately 90% of all hearing loss.
- Histology: A Text and Atlas, Wolters Kluwer
Classification
| Type | Site of Lesion | Example |
|---|---|---|
| Sensory (cochlear) | Hair cells of organ of Corti | Noise-induced, presbycusis |
| Neural (retrocochlear) | CN VIII / auditory nerve | Acoustic neuroma, meningitis |
| Central | Brainstem / auditory cortex | Stroke, multiple sclerosis |
Causes / Etiology
Congenital
- Genetic mutations (connexin 26 - most common; myosin VIa, Ib, VI mutations)
- Prenatal infections (rubella, CMV)
- Prematurity
Acquired
| Category | Examples |
|---|---|
| Noise-induced | Prolonged exposure to loud sounds (rock concerts, jet engines) - damages basal turn hair cells → high-frequency loss |
| Age-related | Presbycusis - progressive bilateral SNHL starting at high frequencies; begins at basal turn |
| Infections | Meningitis, chronic otitis media, labyrinthitis, herpes zoster |
| Ototoxic drugs | Aminoglycoside antibiotics (gentamicin, streptomycin), loop diuretics (furosemide), cisplatin, high-dose aspirin |
| Trauma | Temporal bone fracture, barotrauma |
| Vascular | Internal auditory artery occlusion → sudden SNHL |
| Autoimmune | Autoimmune inner ear disease |
| Metabolic | Hypothyroidism, diabetes |
| Tumors | Acoustic neuroma (vestibular schwannoma) |
| Meniere's disease | Endolymphatic hydrops |
Pathophysiology
The cochlea in normal hearing:
- Sound waves → tympanic membrane vibration → ossicles → oval window → perilymph waves in scala vestibuli → displacement of basilar membrane → bending of stereocilia of hair cells → K⁺ influx → depolarization → neurotransmitter release → CN VIII impulses → auditory cortex
In SNHL - what goes wrong:
- Hair cell damage/loss: Stereocilia of inner or outer hair cells are damaged (by noise, drugs, aging). Once destroyed, hair cells do not regenerate in humans.
- The basal turn of the cochlea (responding to high frequencies) is most vulnerable - hence SNHL typically shows high-frequency loss first
- Loss of outer hair cells → loss of cochlear amplification (outer hair cells normally amplify basilar membrane vibration)
- Loss of inner hair cells → direct loss of signal transduction to CN VIII
Special features of cochlear SNHL:
- Recruitment (abnormal loudness growth): Loudness grows faster than normal just above threshold. This is a hallmark of cochlear (not neural) SNHL. Patient cannot hear soft sounds but is intolerant of loud sounds - the dynamic range is compressed.
- Poor speech discrimination: Even when amplified, speech is unclear - not just "turned down" like conductive loss
Audiogram in SNHL
Both air conduction (AC) AND bone conduction (BC) are equally reduced - there is no air-bone gap.
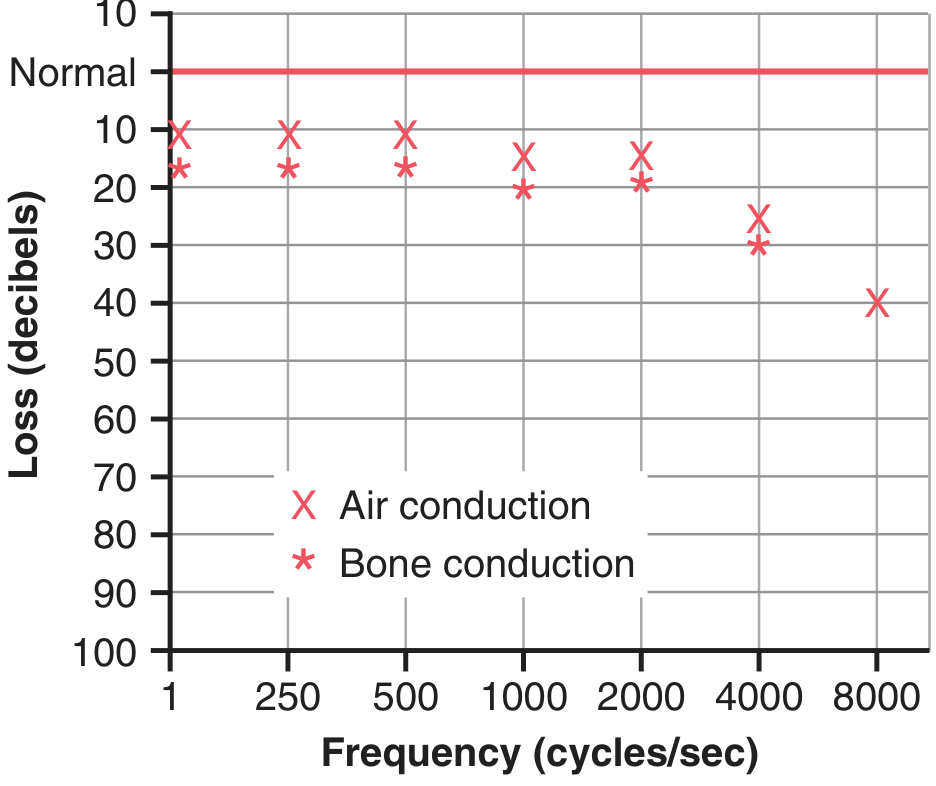
Fig 53.11 from Guyton & Hall - Audiogram of nerve (sensorineural) deafness showing predominantly high-frequency loss. Both air and bone conduction are equally affected - no air-bone gap.
- No air-bone gap (AC = BC, both impaired)
- High-frequency loss pattern common (presbycusis, noise-induced)
- Contrast with conductive deafness: AC impaired, BC normal → air-bone gap present
Tuning Fork Tests
Rinne Test (512 Hz fork)
| Result | Interpretation |
|---|---|
| AC > BC (Positive Rinne) | Normal OR SNHL - in both, air conduction is better than bone |
| BC > AC (Negative Rinne) | Conductive hearing loss |
In SNHL: Both AC and BC are reduced, but AC is still better than BC → Rinne POSITIVE (same as normal, but both are diminished)
Weber Test (512 Hz fork on forehead/vertex)
| Result | Interpretation |
|---|---|
| Sound heard equally | Normal, or bilateral equal SNHL |
| Lateralizes to better (normal) ear | SNHL in the worse ear |
| Lateralizes to worse (affected) ear | Conductive hearing loss in that ear |
In SNHL: Weber lateralizes to the normal/better ear.
Schwabach Test
- Patient's bone conduction compared to a normal-hearing examiner
- In SNHL: Bone conduction diminished (shorter than normal) = Schwabach decreased
- In conductive loss: Bone conduction prolonged (better than normal) = Schwabach increased
Comparison: SNHL vs Conductive Hearing Loss
| Feature | SNHL (Nerve Deafness) | Conductive HL |
|---|---|---|
| Site | Cochlea / CN VIII / CNS | Outer/middle ear |
| Air conduction | Reduced | Reduced |
| Bone conduction | Reduced equally | Normal |
| Air-bone gap | Absent | Present |
| Rinne test | Positive (AC > BC, both ↓) | Negative (BC > AC) |
| Weber test | Lateralizes to normal ear | Lateralizes to affected ear |
| Schwabach | Decreased | Increased |
| Recruitment | Present (cochlear lesion) | Absent |
| Speech discrimination | Poor | Relatively preserved |
| Treatment | Hearing aid / cochlear implant | Often surgical |
Treatment
| Option | Details |
|---|---|
| Hearing aids | Amplify sound; for partial/mild-moderate SNHL; digital aids selectively amplify frequencies patient is most deficient in |
| Cochlear implants | For severe-profound SNHL; electrodes bypass damaged hair cells and directly stimulate CN VIII; FDA-approved from 12 months of age |
| Stem cell research | Experimental; aim to regenerate hair cells |
Key Points for Exams
- SNHL = Both AC and BC impaired equally → no air-bone gap
- Rinne positive in SNHL (AC > BC) - same finding as normal ear, but both thresholds elevated
- Weber lateralizes to better ear in unilateral SNHL
- Recruitment (abnormal loudness growth) = hallmark of cochlear SNHL
- Hair cells do NOT regenerate once damaged
- High-frequency loss is typical (basal cochlea most vulnerable)
- Presbycusis = age-related bilateral progressive SNHL (most common cause in elderly)
- Common ototoxic drugs: Aminoglycosides + Loop diuretics + Cisplatin + High-dose aspirin
- Connexin 26 mutation = most common genetic cause
- Cochlear implant works by directly stimulating CN VIII, bypassing damaged hair cells
Mnemonic
"SNHL = Same Normal (Rinne) - Hear Less"
- Rinne stays positive (same as normal pattern), but hearing is reduced in both modalities
For ototoxic drugs: "A FLING"
- Aminoglycosides
- Furosemide (loop diuretics)
- Loop diuretics
- Indomethacin (high doses)
- Neomycin
- Gentamicin / cisplatin (G for Gold standard chemo)
Sources: Guyton & Hall Textbook of Medical Physiology (Fig. 53.11, 53.12); Ganong's Review of Medical Physiology, 26th Ed. (Table 11-1); Shambaugh Surgery of the Ear; Histology: A Text and Atlas; Bradley & Daroff's Neurology
Classification of nerve fibers physiology mbbs 1st year / reference: AK JAIN
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
I now have everything needed - Guyton's detailed text and figure, Katzung's table, Costanzo's classification table, and Campbell Orthopaedics table. Here is the complete short note:
Classification of Nerve Fibers
Short Note - MBBS 1st Year Physiology
Reference: AK Jain / Guyton & Hall / Costanzo Physiology
Introduction
Nerve fibers differ in diameter, myelination, and conduction velocity. Larger diameter and presence of myelin sheath both increase conduction velocity. There are two main classification systems used in physiology:
- Erlanger & Gasser Classification (A, B, C) - applies to both sensory and motor fibers
- Lloyd & Hunt Classification (I, II, III, IV) - applies only to sensory (afferent) fibers
Range of nerve fiber diameter: 0.5 to 20 μm; Range of conduction velocity: 0.5 to 120 m/sec
- Guyton & Hall Textbook of Medical Physiology
Classification Figure (Guyton & Hall, Fig. 47.6)
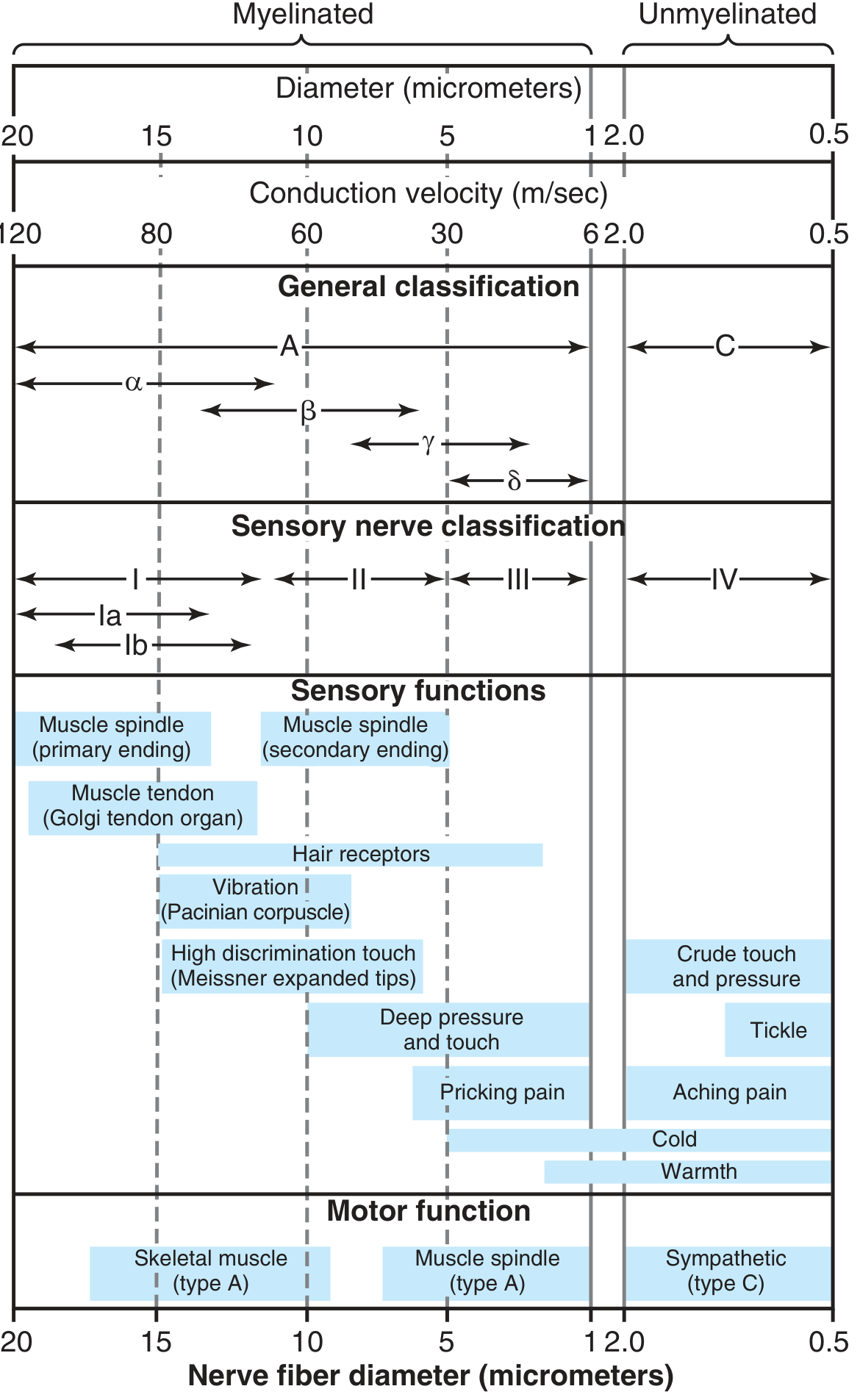
Fig. 47.6 - Guyton & Hall: Complete physiological classification of nerve fibers. Top: diameter and conduction velocity scale. Middle panels: general (A/C) and sensory (I-IV) classification. Bottom panels: sensory and motor functions of each fiber type.
Classification 1: Erlanger & Gasser System (A, B, C)
TYPE A FIBERS - Myelinated, large to medium
| Subtype | Diameter (μm) | Velocity (m/s) | Myelination | Function |
|---|---|---|---|---|
| A-α (alpha) | 12–20 | 70–120 | Heavy | Proprioception (muscle spindle primary endings, GTO); α-motor neurons to skeletal muscle |
| A-β (beta) | 5–12 | 30–70 | Heavy | Touch, pressure, vibration (Meissner's, Pacinian corpuscles) |
| A-γ (gamma) | 3–8 | 15–30 | Heavy | γ-motor neurons → muscle spindle intrafusal fibers (motor); muscle spindle secondary endings (sensory) |
| A-δ (delta) | 2–5 | 5–25 | Light | Fast (first) pain, sharp pricking pain; temperature (cold); crude touch |
TYPE B FIBERS - Lightly myelinated, small
| Type | Diameter (μm) | Velocity (m/s) | Myelination | Function |
|---|---|---|---|---|
| B | < 3 | 3–15 | Light | Preganglionic autonomic fibers (sympathetic and parasympathetic) |
TYPE C FIBERS - Unmyelinated, smallest
| Type | Diameter (μm) | Velocity (m/s) | Myelination | Function |
|---|---|---|---|---|
| C | 0.3–1.3 | 0.5–2.3 | None | Slow (second) pain (dull, aching, burning); crude touch; tickle; warmth; postganglionic autonomic fibers; olfaction |
C fibers constitute more than half of all sensory fibers in most peripheral nerves, plus ALL postganglionic autonomic fibers.
- Guyton & Hall
Classification 2: Lloyd & Hunt System (Sensory Only: I, II, III, IV)
| Group | Equivalent (Erlanger-Gasser) | Diameter (μm) | Receptor / Function |
|---|---|---|---|
| Ia | A-α | ~17 | Annulospiral (primary) endings of muscle spindles - muscle length and velocity |
| Ib | A-α | ~16 | Golgi tendon organs (GTO) - muscle tension |
| II | A-β and A-γ | ~8 | Flower-spray (secondary) endings of muscle spindles; discrete cutaneous tactile receptors (touch, pressure, vibration) |
| III | A-δ | ~3 | Temperature, crude touch, pricking (fast) pain |
| IV | C | 0.5–2 | Slow (aching) pain, itch, warmth, crude touch - unmyelinated |
Comprehensive Master Table
| Fiber | Group (Lloyd) | Diameter (μm) | Velocity (m/s) | Myelin | Key Functions |
|---|---|---|---|---|---|
| Aα | Ia, Ib | 12–20 | 70–120 | Yes (heavy) | Proprioception (spindle primary, GTO); skeletal motor |
| Aβ | II | 5–12 | 30–70 | Yes (heavy) | Touch, pressure, vibration |
| Aγ | II | 3–8 | 15–30 | Yes (heavy) | Muscle spindle motor (intrafusal); spindle secondary |
| Aδ | III | 2–5 | 5–25 | Yes (light) | Fast pain (sharp/pricking); cold temperature; crude touch |
| B | - | <3 | 3–15 | Yes (light) | Preganglionic autonomic |
| C | IV | 0.3–1.3 | 0.5–2.3 | No | Slow pain (dull/aching/burning); warmth; crude touch; itch; postganglionic autonomic |
Key Physiological Concepts
1. Factors Determining Conduction Velocity
- Larger diameter → faster conduction (lower internal resistance)
- Myelination → faster conduction (saltatory conduction at nodes of Ranvier)
- Largest (Aα): 120 m/sec = travels length of football field per second
- Smallest (C): 0.5 m/sec = takes ~2 seconds to travel from big toe to spinal cord
2. Fast Pain vs. Slow Pain
| Feature | Fast (First) Pain | Slow (Second) Pain |
|---|---|---|
| Fiber | A-δ (Group III) | C (Group IV) |
| Character | Sharp, pricking, well-localized | Dull, burning, aching, diffuse |
| Latency | Short (rapid) | Longer delay |
| Example | Needle prick | Toothache, inflammatory pain |
3. Autonomic Fibers
| Preganglionic | Postganglionic | |
|---|---|---|
| Fiber type | B (lightly myelinated) | C (unmyelinated) |
| Velocity | 3–15 m/s | 0.5–2.3 m/s |
4. Sensitivity to Local Anesthetics
Smaller fibers are blocked at lower concentrations:
- B > C > Aδ > Aβ > Aα (B and C blocked first, Aα hardest to block)
- Order of block: Sympathetic (B/C) → Sensory (pain/temperature) → Touch/pressure → Motor (Aα last)
Mnemonics
For Erlanger-Gasser (A, B, C):
"All Big Cats" → A (myelinated somatic), B (myelinated autonomic preganglionic), C (unmyelinated)
For A fiber subtypes in order:
"α - β - γ - δ" → "After Being Given Delta"
- α = biggest, fastest (proprioception + motor)
- β = touch/pressure
- γ = muscle spindle motor
- δ = fast pain/temperature
For fast vs. slow pain:
"A-Delta = Acute (sharp) pain; C = Chronic (dull) pain"
For Lloyd-Hunt groups and receptors:
| Group | Mnemonic |
|---|---|
| Ia | "I am the Primary spindle" |
| Ib | "I belong to GTO (tendon)" |
| II | "IIndeed - secondary spindle + touch" |
| III | "IIIrky pain (fast) + temperature" |
| IV | "IV - the last and slowest - dull pain" |
Summary in One Line Each
- Aα - largest, fastest, proprioception + skeletal muscle motor
- Aβ - touch and pressure
- Aγ - muscle spindle motor (intrafusal)
- Aδ - fast pain + cold temperature (myelinated "pain" fiber)
- B - preganglionic autonomic (lightly myelinated)
- C - slow pain + warmth + postganglionic autonomic (unmyelinated, slowest)
Sources: Guyton & Hall Textbook of Medical Physiology (Fig. 47.6, p. 587); Costanzo Physiology, 7th Ed. (Table 3.1, p. 80); Katzung's Basic & Clinical Pharmacology, 16th Ed. (Table 26-3); Campbell's Operative Orthopaedics, 15th Ed. (eTable 46.1)
This is a shared conversation. Sign in to Orris to start your own chat.