Cardiac arrest silently
Reading File
Checking Date & Time
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching PubMed
"sudden cardiac death" AND "silent" OR "no warning" AND prevention
Searching PubMed
"sudden cardiac death"[MeSH Terms] AND prevention
Reading File
Now I have comprehensive information to provide a thorough answer. Let me synthesize everything.
Cardiac Arrest — The Silent Killer
What Makes It "Silent"
Cardiac arrest can strike without warning. A key clinical fact is that Sudden Cardiac Death (SCD) may be the first manifestation of otherwise phenotypically silent cardiac disease — meaning a person may have underlying structural or electrical heart disease, yet appear entirely healthy until the arrest occurs.
Key statistics underscoring its silent nature:
- 80% of sudden cardiac deaths occur in the home environment
- Up to 40% are unwitnessed
- 80–90% of patients successfully resuscitated from SCD show no enzymatic or ECG evidence of myocardial necrosis — even when the underlying cause is ischemic heart disease
- SCD can be the first clinical manifestation of IHD in many patients
— Fuster and Hurst's The Heart, 15th Edition, p. 1191; Robbins & Kumar Basic Pathology, p. 362
Definition
- Sudden Cardiac Death (SCD): Unexpected death from a cardiac cause within 1 hour of symptom onset (or within 24 hours of being last seen well)
- Sudden Cardiac Arrest (SCA): Same event, but the person is successfully resuscitated
- Estimated 325,000–450,000 deaths annually in the United States; 4–5 million worldwide
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Robbins & Kumar Basic Pathology
Mechanism
The mechanism is almost always a lethal arrhythmia:
| Mechanism | Notes |
|---|---|
| Ventricular Fibrillation (VF) | Most common in out-of-hospital SCD |
| Ventricular Tachycardia (VT) | Deteriorates into VF |
| Asystole | ~50% of out-of-hospital cardiac arrests at EMS arrival |
| Pulseless Electrical Activity (PEA) | ~20–25% |
Most cases of fatal arrhythmia are triggered by electrical irritability of the myocardium distant from the major conduction system — not direct conduction system damage. The heart's tissue becomes irritable from chronic ischemia or prior scarring, generating re-entry circuits that cascade into VF.
— Robbins, Cotran & Kumar Pathologic Basis of Disease
Underlying Causes (Why It's Occult Until It Strikes)
In Adults (>35 years)
| Cause | Notes |
|---|---|
| Coronary Artery Disease (CAD) | Responsible for 65–70% of SCD; acute plaque rupture found in only 10–20% — most have chronic, silent atherosclerosis |
| Hypertensive heart disease | Hypertrophy + fibrosis → arrhythmogenic substrate |
| Dilated/Hypertrophic Cardiomyopathy | HCM: SCD incidence 0.5–0.8%/year; often the first manifestation |
| Healed prior MI | Present in ~40% of SCD victims — old, silent scar provides re-entry substrate |
In Young Patients (<35 years) — Most Likely to Be Completely Silent
| Cause | Notes |
|---|---|
| Channelopathies (Long QT, Brugada, CPVT) | Structurally normal heart; ion channel mutations — no symptoms until arrhythmia |
| Hypertrophic Cardiomyopathy (HCM) | Most common cause of SCD in young athletes |
| Congenital coronary artery anomalies | Asymptomatic until exertion-triggered ischemia |
| Myocarditis | Inflammatory, often follows a viral illness |
| Arrhythmogenic Right Ventricular Dysplasia (ARVD) | Fibro-fatty replacement of RV myocardium |
| Mitral valve prolapse | Rarely, malignant arrhythmic phenotype |
| Early repolarization syndrome | J-point elevation ≥0.1 mV in inferior leads → 43% increased risk of arrhythmic death; up to 3-fold increase with ≥0.2 mV elevation |
— Fuster and Hurst's The Heart, 15th Edition, p. 1193–1194; Robbins & Kumar Basic Pathology
Why Silent? — The Pathophysiology
- No myocardial necrosis needed: In most SCD from CAD, arrhythmia is triggered by sublethal ischemia or pre-existing scar — not an acute MI. The person has no chest pain, no troponin rise.
- Channelopathies: The heart looks structurally normal on echo, ECG may be subtle or intermittently abnormal. The trigger is often electrolyte shifts, adrenergic surges (exercise, emotion), or drug interactions.
- Silent ischemia: CAD can cause chronic myocardial irritability without causing angina (especially in diabetics, elderly, and women).
- Increased cardiac mass alone (hypertension, obesity, cocaine use) creates an arrhythmogenic substrate with no overt symptoms.
Risk Factors for Silent SCD
- Male sex, age 45–64 (7:1 male:female ratio; narrows to 2:1 after age 65)
- Women are more likely than men (64% vs 50%) to suffer SCD without prior evidence of coronary heart disease
- Family history of premature SCD
- Known LV dysfunction (every 10% drop in LVEF → 39% increase in mortality hazard)
- Diabetes (silent hypoglycemia can trigger arrhythmias)
- Cocaine/methamphetamine use
- Sleep apnea, hypertension, obesity
Prevention Strategies
| Intervention | Indication |
|---|---|
| Implantable Cardioverter-Defibrillator (ICD) | Gold standard; 50% reduction in arrhythmic death; 25% reduction in all-cause mortality (secondary prevention). Primary prevention in EF <35% |
| Beta-blockers | Reduce sympathetic-triggered arrhythmias in IHD, HCM, channelopathies |
| Amiodarone | Equivalent to ICD in patients with EF >35%; useful for VT suppression |
| Catheter ablation | VT substrate modification, especially in scar-related VT |
| Genetic screening | Channelopathies and HCM — family cascade screening |
| ECG screening | Athletes; identifies Brugada, long QT, WPW, HCM |
| AED access / CPR training | Community-level response; critical when 80% of arrests occur at home |
— Fuster and Hurst's The Heart, 15th Edition, p. 1194; Braunwald's Heart Disease
Key Takeaway
The "silence" of cardiac arrest is rooted in its underlying pathophysiology: chronic, clinically undetected structural changes (atherosclerosis, hypertrophy, fibrosis) or electrical mutations (channelopathies) create a substrate that remains dormant until a triggering event — a sympathetic surge, an electrolyte shift, transient ischemia — ignites a lethal arrhythmia. By the time arrest occurs, there is often no prior warning, no prodrome, no diagnosis. This makes population-level screening, risk factor modification, genetic testing in high-risk families, and community CPR/AED availability the pillars of prevention.
Rigor mortis
Checking Date & Time
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have everything needed for a comprehensive answer.
Rigor Mortis
Definition
Rigor mortis (Latin: stiffness of death) is the postmortem stiffening of all skeletal muscles of the body into a state of contracture. It occurs without action potentials, affecting all voluntary and involuntary striated muscle groups uniformly.
Molecular Mechanism — The ATP Cross-Bridge Lock
The explanation lies entirely in the cross-bridge cycle of muscle contraction:
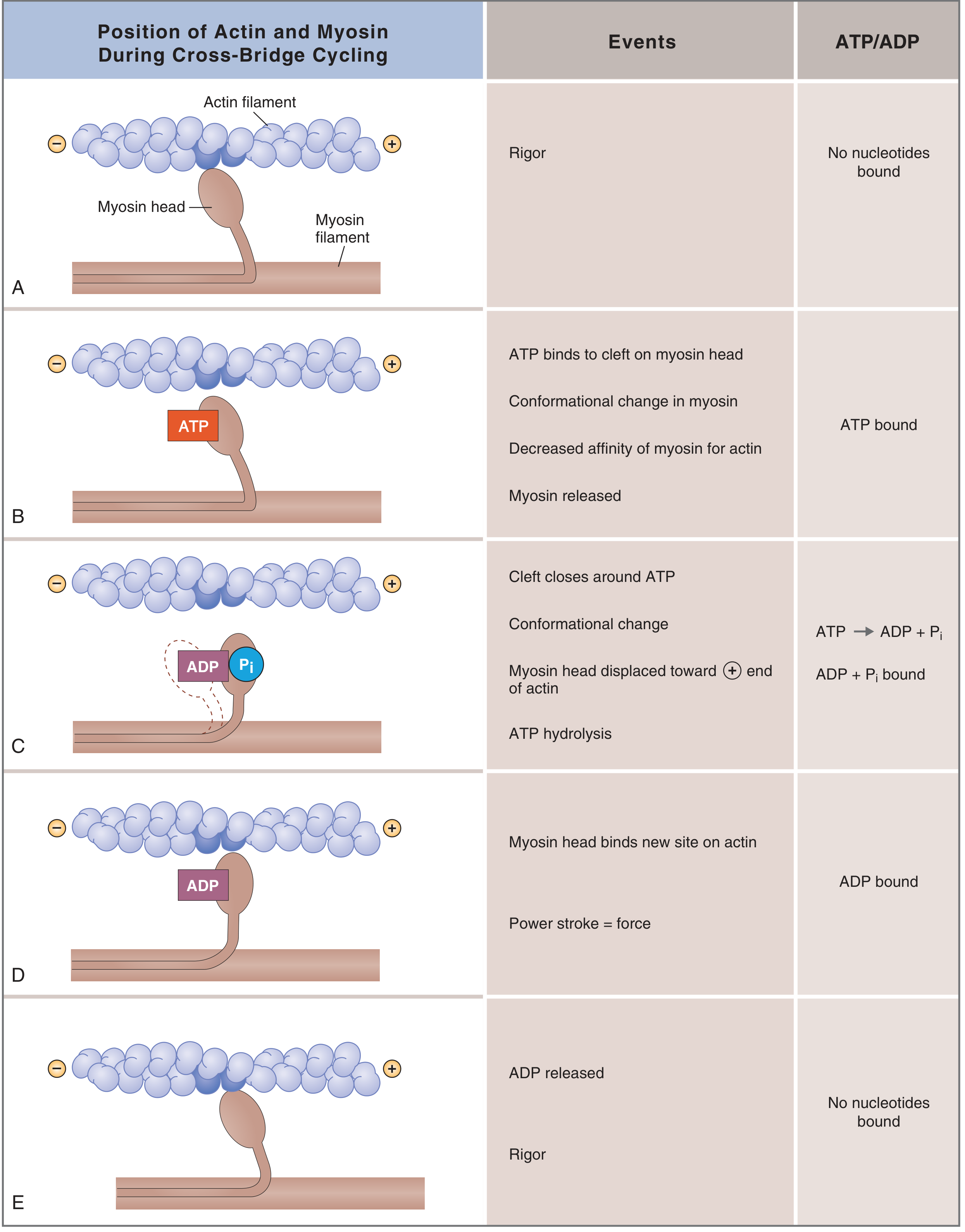
Cross-bridge cycle in skeletal muscle. State A/E (no nucleotide bound) = the "rigor" position. — Costanzo Physiology, 7th Ed.
In a living, relaxed muscle, the cycle proceeds as follows:
| Step | What Happens |
|---|---|
| A — Rigor position | No ATP bound; myosin head locked tightly onto actin |
| B — ATP binds | ATP binding reduces myosin's affinity for actin → myosin releases |
| C — ATP hydrolysis | ATP → ADP + Pᵢ; myosin head cocks into power-stroke position |
| D — Power stroke | Myosin binds new actin site; Pᵢ released → force generated |
| E — ADP released | Returns to rigor position; cycle restarts with next ATP |
After death, cellular respiration ceases → ATP production stops → residual ATP is consumed → myosin heads cannot be released from actin.
"In the complete absence of ATP, the actin-myosin crossbridges become stable, which accounts for the rigidity of skeletal muscles (rigor mortis) that occurs as mitochondrial activity stops after death." — Junqueira's Basic Histology, 17th Ed.
"In a corpse soon after death, the lack of ATP prevents the cycle from proceeding further; this leads to an extreme example of muscle rigidity — called rigor mortis — that is limited only by protein decomposition." — Medical Physiology (Boron & Boulpaep)
Essentially: every myosin head locks permanently in the "strong binding" state — the muscle is frozen mid-cycle. This is the same rigor linkage that occurs transiently during ischemia when intracellular ATP drops too far.
— Braunwald's Heart Disease, 2nd Vol.
Calcium's Role
After death, the sarcoplasmic reticulum loses integrity and can no longer sequester calcium. Calcium floods the cytoplasm, causing an initial wave of contraction throughout the muscle. Combined with the absence of ATP (which is also needed to drive the Ca²⁺-ATPase/SERCA pump back), the muscle cannot relax — locking in a contracted, rigid state.
Timeline
| Phase | Timing | Description |
|---|---|---|
| Onset | ~1–4 hours after death | Muscles begin stiffening; starts in smaller muscles (face, jaw) |
| Full rigidity | ~6–12 hours | All muscle groups maximally stiff (head-to-toe) |
| Peak | ~12 hours | Maximum stiffness |
| Resolution | ~15–25 hours | Proteins begin to decompose via autolysis (lysosomal enzymes); muscles become flaccid again |
"The muscles remain in rigor until the muscle proteins deteriorate about 15 to 25 hours later, which presumably results from autolysis caused by enzymes released from lysosomes." — Guyton and Hall Textbook of Medical Physiology
Temperature dependency: All these events occur faster at higher temperatures and slower at lower temperatures. This is why rigor mortis has forensic relevance — it must be interpreted against ambient temperature.
Forensic Significance
- Rigor mortis, together with livor mortis (dependent lividity), is used as a sign of irreversible death
- It develops after hours of cardiac arrest — pupils dilate within 1 minute, but rigor takes considerably longer
- In hypothermia, "pseudo-rigor mortis" (muscle rigidity from cold) can mimic true rigor mortis — hence rigor alone cannot confirm death in a cold patient
"Hypothermia can cause muscle rigidity, termed pseudo-rigor mortis; hence, rigor mortis cannot be used as a reliable marker of death in the cold patient." — Tintinalli's Emergency Medicine
- Resuscitation should be withheld when true rigor mortis is present alongside irreversible signs (decapitation, dependent lividity) — Fuster and Hurst's The Heart, 15th Ed.
Sequence of Postmortem Changes (Context)
| Change | Onset | Mechanism |
|---|---|---|
| Pallor | Immediate | Loss of circulation |
| Algor mortis (body cooling) | Immediate–hours | Body equilibrates to ambient temp |
| Livor mortis (lividity) | 1–2 hours | Blood pools dependently by gravity |
| Rigor mortis | 1–4 hours | ATP depletion → actin-myosin lock |
| Putrefaction | 24–72 hours | Bacterial autolysis begins |
Summary
Rigor mortis is the physical expression of a biochemical endpoint: without ATP, the molecular motors of muscle — myosin cross-bridges — cannot detach from actin, locking every muscle in rigid contracture. It begins within hours, peaks around 12 hours, and resolves at 15–25 hours as proteins begin to auto-digest. Temperature accelerates or retards the entire process, which is central to its use in forensic medicine for estimating time of death.
Myocardial infraction
Reading File
Checking Date & Time
Finding Sources
Finding Sources
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.