Maintenance of ph of body physiology short notes
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have all the content needed. Let me compile the comprehensive short notes.
Maintenance of pH of Body - Physiology Short Notes
Normal Blood pH
- Arterial blood pH is maintained between 7.35 and 7.45 (normal = 7.40)
- Intracellular pH ranges from 7.0 to 7.3
- pH = -log[H+]; a 10-fold change in [H+] = a shift of 1 pH unit
- Even small pH changes alter enzyme activity, protein conformation, ion channel function, and receptor binding
Sources of Acid Load
| Source | Type | Amount |
|---|---|---|
| Lipid & carbohydrate metabolism | CO2 (volatile acid) | ~15,000 mmol/day |
| Protein metabolism (methionine, cysteine) | H2SO4, H3PO4 (non-volatile) | ~1 mmol/kg/day |
| Organic acids (lactic, pyruvic, acetic) | Non-volatile | Small daily amount |
| Stool alkali excretion | Net acid equivalent | Minimal |
Animal foods (high protein, organophosphates) = net acid load. Plant foods (high organic anions) = net alkaline load.
Three Lines of Defense
The body uses three sequential mechanisms to maintain pH:
Buffers (immediate) → Lungs (minutes) → Kidneys (hours to days)
1. Buffer Systems (Chemical Defense)
Buffers minimize pH change - they do not remove acid from the body.
A. Bicarbonate-CO2 System (most important ECF buffer)
The Henderson-Hasselbalch equation:
pH = pKa + log [HCO3-] / [CO2]
Or practically:
pH = 6.1 + log [HCO3-] / (0.03 × PaCO2)
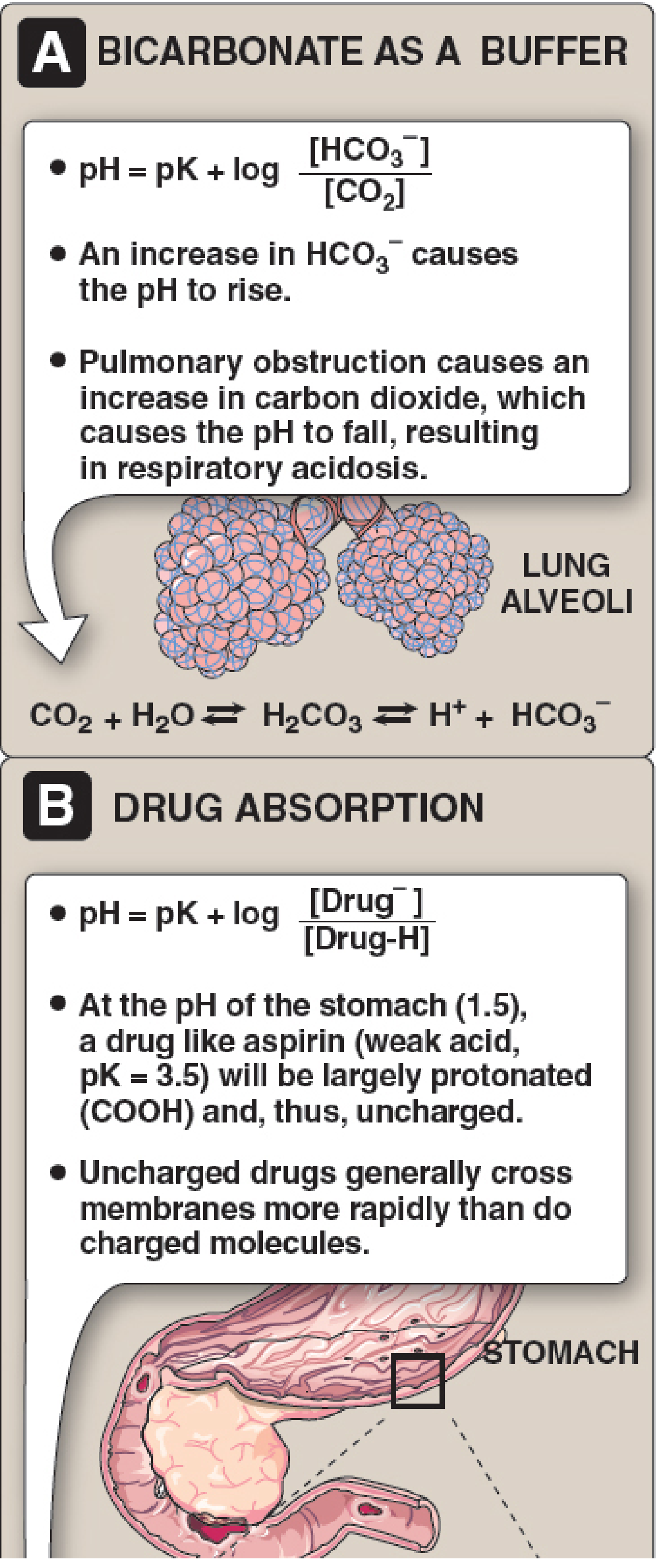
- When acid (HA) is added: HA + NaHCO3 → NaA + H2O + CO2
- HCO3- is consumed but CO2 is blown off by lungs, so pH change is minimal
- pH is determined by the ratio of HCO3- to CO2 - not their absolute values
B. Other ECF Buffers
- Plasma proteins (e.g., albumin)
- Phosphate (HPO4²- / H2PO4-), pKa 6.8 - more important in urine than plasma
C. Intracellular Buffers
- Hemoglobin (major intracellular buffer in blood)
- Cellular proteins
- Organophosphate complexes
- Intracellular HCO3- and H+-HCO3- transport mechanisms
D. Bone as Buffer
- In chronic metabolic acidosis, bone acts as a major buffer reserve
- Acid-induced dissolution of bone apatite releases Ca2+ salts and HCO3- into ECF
- Chronic use leads to osteomalacia, osteoporosis, hypercalciuria, and renal stones
2. Respiratory Regulation (Fast, Minutes)
The lungs regulate CO2 (the volatile acid component) by controlling alveolar ventilation.
- Acidosis stimulates the respiratory center → increased ventilation → CO2 blown off → pH rises
- Alkalosis depresses ventilation → CO2 retained → pH falls
Quantitative Respiratory Compensation:
| Disorder | Compensation |
|---|---|
| Metabolic acidosis | PaCO2 decreases 1.2 mmHg per 1 mmol/L decrease in HCO3- (Winter's formula: PaCO2 = 1.5×[HCO3-] + 8 ± 2) |
| Metabolic alkalosis | PaCO2 increases 0.7 mmHg per 1 mmol/L increase in HCO3- |
Respiratory compensation is rapid but rarely normalizes pH completely.
3. Renal Regulation (Slow, Hours to Days)
The kidneys regulate HCO3- (the base component) and are the only organs that can truly excrete or generate new bicarbonate.
Net Acid Excretion (NAE):
NAE = V × (U_NH4+ + U_TA - U_HCO3-)
- ~40% of NAE = Titratable acids
- ~60% of NAE = Ammonium (NH4+)
- Urinary HCO3- is essentially zero under normal conditions
Renal Mechanisms by Segment:
Proximal Tubule (reabsorbs ~80% of filtered HCO3-)
- H+ is secreted into lumen via Na+-H+ antiporter (NHE3) (2/3 of H+ secretion) and H+-ATPase (1/3)
- Secreted H+ combines with filtered HCO3- → H2CO3 → CO2 + H2O (catalyzed by carbonic anhydrase IV on brush border)
- CO2 re-enters cell → reconverted to H+ + HCO3- by carbonic anhydrase II → HCO3- exits basolateral side via NBCe1 (Na+-3HCO3- cotransporter)
- Also synthesizes NH3 (ammonia) and titrates phosphate to H2PO4-
Thick Ascending Limb (TAL)
- Reabsorbs remaining HCO3- via NHE3 (apical) and AE2/KCC4 (basolateral)
Distal Nephron / Collecting Duct
- Alpha-intercalated (α-IC) cells: secrete H+ via H+-ATPase and H+-K+-ATPase; generate new HCO3-
- Beta-intercalated (β-IC) cells: secrete HCO3- (active in alkalosis)
- The ratio of α to β cells adjusts based on chronic acid-base status
Titratable Acids
- Weak acids filtered at glomerulus that act as urinary buffers
- Most important = Phosphate (HPO4²- → H2PO4-, pKa 6.80)
- Limited capacity; under increased acid load, NH4+ excretion compensates
Ammonium (NH4+) - Major Adaptive Mechanism
- NH3 is synthesized in the proximal tubule from glutamine (glutaminase reaction)
- NH3 diffuses into tubular lumen and combines with secreted H+ → NH4+ (trapped in lumen by "ion trapping")
- NH4+ excretion can increase 10-fold in chronic acidosis - this is the primary adaptive mechanism
- NH4+ is also reabsorbed in TAL and re-secreted in collecting duct (the NH4+ recycling pathway)
Summary Table
| System | Mechanism | Speed | Normalizes pH? |
|---|---|---|---|
| Chemical buffers | Titrate H+ without excretion | Immediate (seconds) | No |
| Respiratory | Adjust PaCO2 via ventilation | Minutes | Rarely |
| Renal | Regulate HCO3-, excrete NH4+/TA | Hours to days | Yes |
Key Equations to Remember
| Equation | Use |
|---|---|
| pH = 6.1 + log[HCO3-]/(0.03 × PaCO2) | Henderson-Hasselbalch for blood |
| Normal: pH 7.40, PaCO2 40 mmHg, HCO3- 24 mEq/L | Normal values |
| NAE = V(U_NH4+ + U_TA - U_HCO3-) | Net acid excretion |
Sources: Comprehensive Clinical Nephrology, 7th Ed. (Ch. 12) | Medical Physiology (Boron & Boulpaep, Ch. 28) | Lippincott's Biochemistry, 8th Ed. (Ch. 1)
This is a shared conversation. Sign in to Orris to start your own chat.