Write a 30 marks answer for Postgraduate Anaesthesia exam on the topic of coagulation cascade and thromboelastography
Reading File
Finding Sources
Finding Sources
Searching PubMed
thromboelastography coagulation monitoring anaesthesia
Finding Sources
Reading File
Reading File
Reading Article
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
I now have comprehensive content from multiple authoritative sources. Let me write the full postgraduate-level exam answer.
Coagulation Cascade and Thromboelastography
Postgraduate Anaesthesia Examination Answer (30 Marks)
1. Introduction (2 marks)
Haemostasis is a tightly regulated physiological process that arrests bleeding while maintaining vascular patency. It integrates three overlapping phases: primary haemostasis (platelet plug formation), secondary haemostasis (the coagulation cascade generating fibrin), and fibrinolysis (clot dissolution). Understanding the cascade and its point-of-care assessment with thromboelastography (TEG) and rotational thromboelastometry (ROTEM) is fundamental to perioperative and critical care anaesthetic practice.
2. The Coagulation Cascade (12 marks)
2.1 Classical (Waterfall) Model
The classical model, developed in the 1960s, divides coagulation into the extrinsic pathway, the intrinsic pathway, and a common pathway that converge at Factor Xa activation.
The coagulation cascade is a series of amplifying enzymatic reactions leading to deposition of an insoluble fibrin clot. Each reaction step involves an enzyme (activated coagulation factor), a substrate (inactive proenzyme), and a cofactor (reaction accelerator), assembled on negatively charged phospholipid surfaces provided by activated platelets. Calcium is required, binding to gamma-carboxylated glutamic acid residues on factors II, VII, IX, and X - these residues are synthesised using Vitamin K as cofactor and are antagonised by coumarin anticoagulants. (Robbins, Cotran & Kumar: Pathologic Basis of Disease)
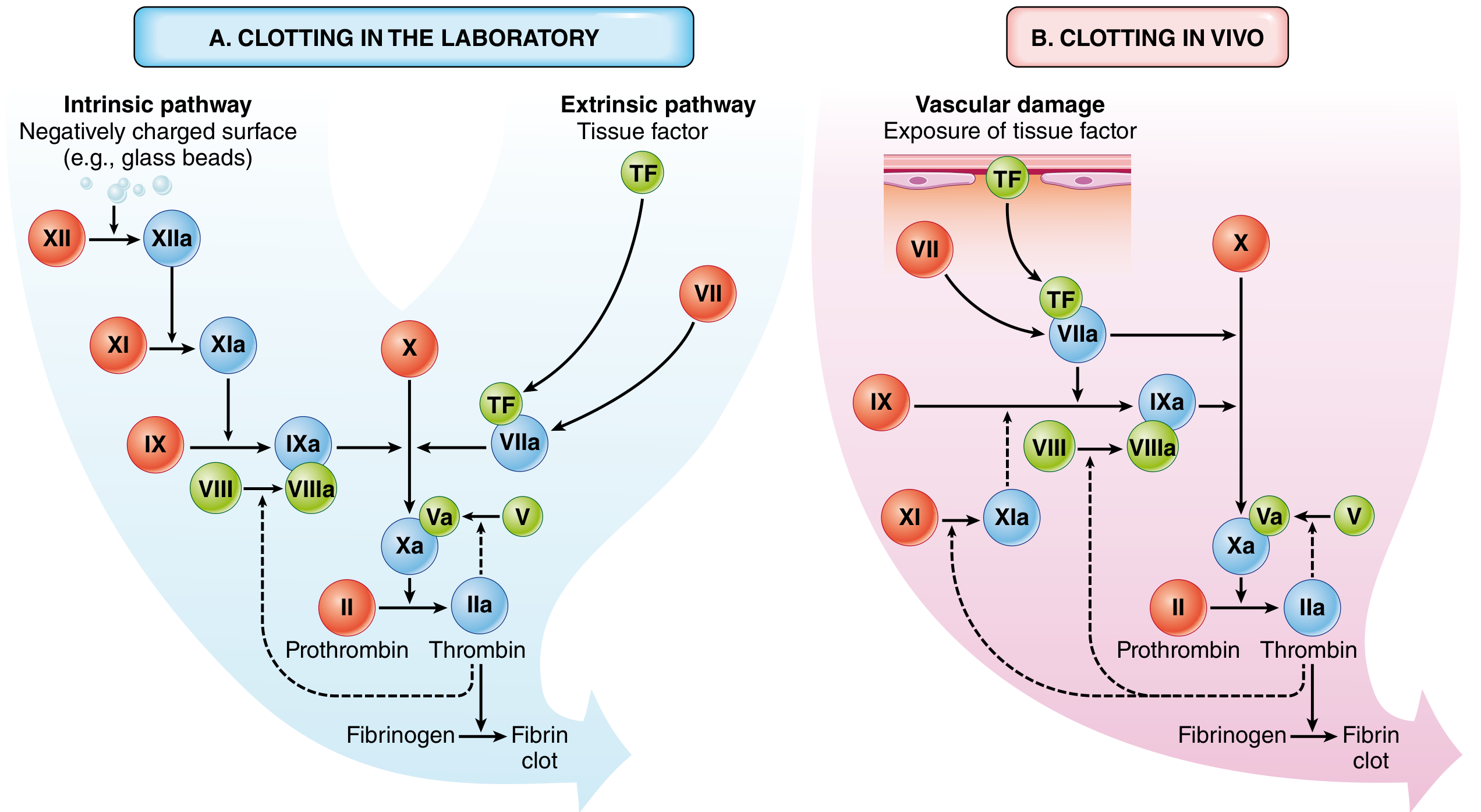
Extrinsic pathway (assessed by PT/INR):
- Tissue factor (TF), a subendothelial transmembrane glycoprotein constitutively expressed on fibroblasts and vascular smooth muscle cells, is exposed by vascular injury
- TF binds plasma FVII, activating it to FVIIa (the TF:FVIIa extrinsic tenase complex)
- TF:FVIIa activates FX → FXa and also FIX → FIXa
- The PT assay assesses factors VII, X, V, II (prothrombin), and fibrinogen
Intrinsic pathway (assessed by aPTT):
- Initiated in vitro by negatively charged surfaces activating FXII → FXIIa (Hageman factor)
- FXIIa activates FXI → FXIa, which activates FIX → FIXa
- FIXa + FVIIIa (intrinsic tenase complex on platelet surface) → activates FX
- The aPTT assesses factors XII, XI, IX, VIII, X, V, II, and fibrinogen
Common pathway:
- FXa + FVa (prothrombinase complex, assembled on negatively charged platelet membrane in the presence of calcium) converts prothrombin (FII) → thrombin (FIIa)
- Thrombin cleaves fibrinogen → fibrin monomers → polymerised insoluble fibrin
- Thrombin activates FXIII → FXIIIa, a transglutaminase that covalently cross-links fibrin strands, stabilising the clot
- Thrombin also activates FV, FVIII, FXI (positive feedback amplification loops), and platelet activation via protease-activated receptor-1 (PAR-1)
Limitation of the classical model: Clinical observations challenge its relevance in vivo. Deficiency of FXII does not cause bleeding despite prolonging the aPTT. FVII and FVIII/FIX (haemophilias A and B) deficiencies cause severe bleeding even though each affects only one pathway. This paradox is resolved by the cell-based model. (Sabiston Textbook of Surgery; Harrison's Principles of Internal Medicine 22E)
2.2 Cell-Based Model of Coagulation (Current Paradigm)
The cell-based model, now the accepted physiological framework, emphasises overlapping interactions between coagulation proteins and specific cell membranes. It proceeds in three phases:
Phase 1 - Initiation (on TF-bearing cells - fibroblasts/VSMC):
Vascular injury exposes subendothelial TF to plasma FVII, creating the TF:FVIIa complex. This activates small amounts of FX → FXa and FIX → FIXa. FXa + FVa on TF-bearing cells form the prothrombinase complex, generating trace thrombin - the trigger for amplification. Tissue factor pathway inhibitor (TFPI) rapidly inhibits the TF:FVIIa:FXa complex, limiting this phase. (Sabiston Textbook of Surgery)
Phase 2 - Amplification (on platelet surface):
Trace thrombin generated in initiation travels to the injury site and activates platelets (via PAR-1/PAR-4), FV → FVa, and FVIII → FVIIIa, and releases vWF. Platelets adhere via GPIb to vWF and via GPIa/IIa or GPVI to subendothelial collagen. Platelet structural change produces net negatively charged outer membranes - the platform for coagulation assembly. This phase dramatically amplifies the pro-coagulant signal.
Phase 3 - Propagation (on activated platelet surface):
The assembled intrinsic tenase complex (FIXa + FVIIIa) and prothrombinase complex (FXa + FVa) on the platelet surface generate a thrombin burst - large quantities of thrombin that:
- Cleave fibrinogen → fibrin monomers
- Activate FXIII → cross-linked fibrin
- Activate TAFI (thrombin activatable fibrinolysis inhibitor)
- Sustain further platelet and factor activation (Schwartz's Principles of Surgery 11e; Rockwood & Green's Fractures in Adults 10e)
2.3 Anticoagulant Mechanisms (4 marks)
Four major endogenous anticoagulant systems prevent unbounded clot propagation:
| Inhibitor | Mechanism |
|---|---|
| Antithrombin III (ATIII) | Serine protease inhibitor inactivating thrombin, FXa, FIXa, FXIa, FXIIa. Heparin binds ATIII, inducing a conformational change that accelerates its activity ~1000-fold. Physiologically potentiated by heparan sulphate on endothelial surfaces |
| Tissue Factor Pathway Inhibitor (TFPI) | Directly inhibits the TF:FVIIa:FXa complex, limiting initiation phase. Produced by endothelium |
| Protein C / Protein S system | Thrombin bound to thrombomodulin (expressed on intact endothelium) activates Protein C. Activated Protein C (APC) + Protein S (cofactor) inactivate FVa and FVIIIa, shutting down the propagation phase |
| Prostacyclin (PGI2) and Nitric Oxide | Released by intact endothelium; inhibit platelet aggregation and cause vasodilatation |
(Harrison's Principles of Internal Medicine 22E; Goldman-Cecil Medicine)
2.4 Fibrinolysis
Once haemostasis is achieved, fibrinolysis restores vascular patency. Tissue-type plasminogen activator (t-PA), synthesised by endothelium and most active when bound to fibrin, converts plasminogen → plasmin. Plasmin degrades fibrin into fibrin degradation products (FDPs), notably D-dimers - a clinically useful marker of thrombus formation and lysis (DVT/PE screening, DIC). Alpha-2-antiplasmin rapidly inactivates free circulating plasmin. Plasminogen activator inhibitor-1 (PAI-1) inhibits t-PA and uPA. In DIC, PAI-1 is elevated, suppressing normal fibrinolysis and worsening microvascular thrombosis. (Robbins Pathologic Basis of Disease; Sabiston Textbook of Surgery)
3. Thromboelastography (TEG) and Rotational Thromboelastometry (ROTEM) (12 marks)
3.1 Principle and Technology
TEG (Haemonetics) and ROTEM (Werfen) are point-of-care viscoelastic haemostatic assays (VHAs) that measure the mechanical properties of whole blood as it clots. Unlike standard laboratory tests (PT, aPTT, platelet count), which assess individual components of coagulation in plasma under static conditions, VHAs assess the entire haemostatic process - including coagulation factor activity, platelet function, fibrinogen contribution, clot strength, and fibrinolysis - simultaneously and in real time.
Mechanism: In TEG, a small sample of whole blood is placed in a heated cuvette (37°C). A pin is suspended in the blood on a torsion wire. The cuvette oscillates; as a clot forms and strengthens, the increasing mechanical resistance is transmitted to the pin, which is detected as an electrical signal and plotted graphically as the characteristic thromboelastogram. In ROTEM, the cuvette is stationary and the pin rotates - functionally equivalent results, though numerical values differ and are not interchangeable. (Morgan & Mikhail's Clinical Anesthesiology 7e; Scott-Brown's Otorhinolaryngology, Head & Neck Surgery)
3.2 TEG Trace Parameters and Clinical Interpretation
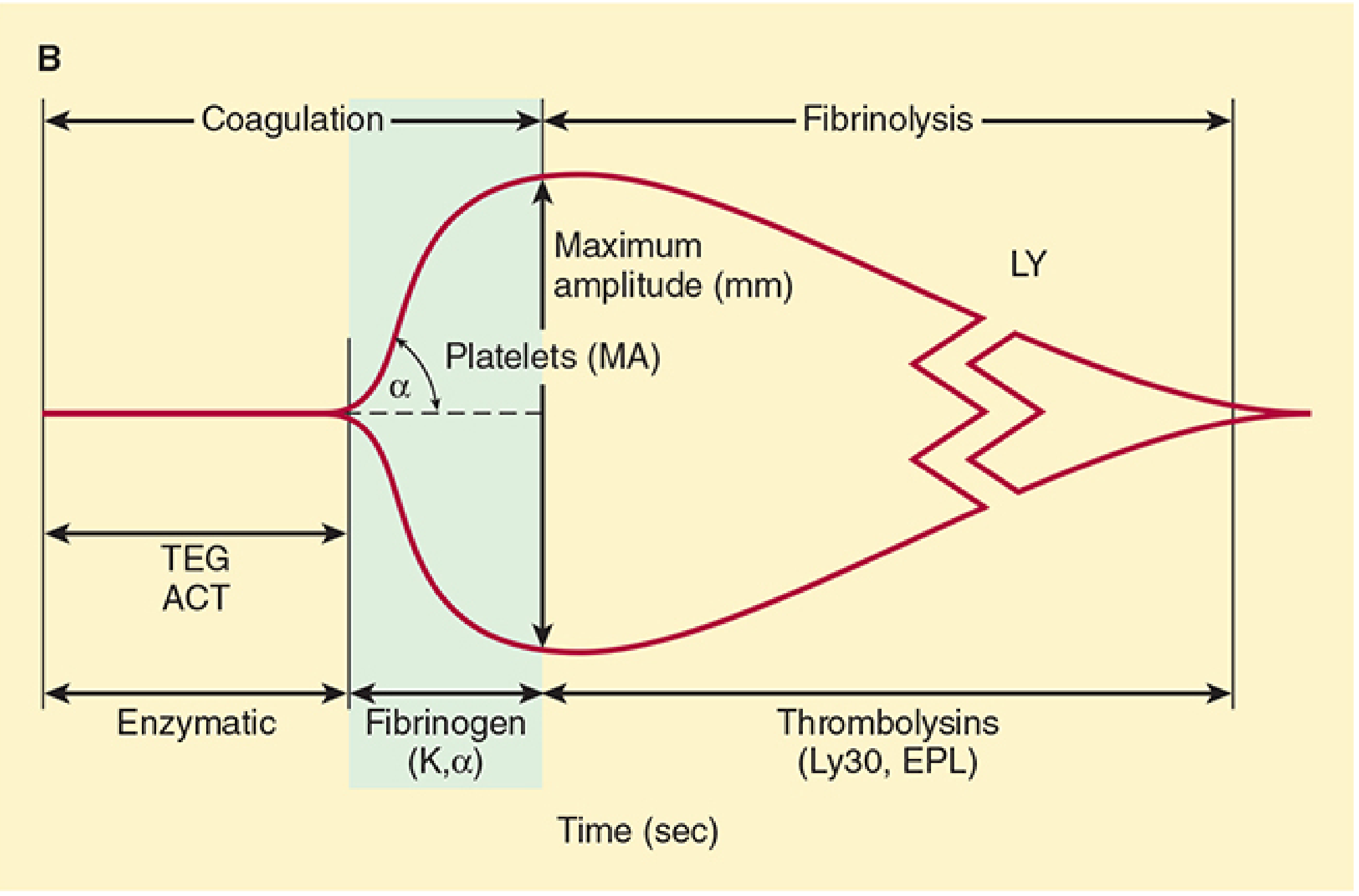
| Parameter | Definition | Normal Range | Clinical Significance |
|---|---|---|---|
| R time (Reaction time) | Time from sample placement to first clot detection (2mm amplitude) | 5-10 min | Prolonged: coagulation factor deficiency, anticoagulants (heparin, warfarin, DOACs). Shortened: hypercoagulable state |
| K time (Kinetics) | Time from R-time to 20mm amplitude; clot formation rate | 1-3 min | Prolonged: fibrinogen deficiency, thrombocytopaenia. Reflects fibrinogen and early platelet activity |
| Alpha angle (α) | Angle of tangent to the curve at 2mm; rate of fibrin accumulation | 53-72° | Reduced: fibrinogen deficiency, hypofibrinogenaemia. Increased: hypercoagulability. Guides cryoprecipitate use |
| Maximum Amplitude (MA) | Greatest vertical width; reflects clot strength | 50-70 mm | Reduced: platelet dysfunction or thrombocytopaenia (platelets contribute ~80% of clot strength, fibrinogen ~20%). Guides platelet transfusion |
| LY30 (Lysis at 30 min) | % reduction in amplitude 30 minutes after MA | <7.5% | Elevated (>7.5-8%): hyperfibrinolysis. Guides tranexamic acid / aminocaproic acid use |
| EPL (Estimated Percent Lysis) | Predicted lysis before 30 min | <15% | Similar clinical use to LY30 |
| CI (Coagulation Index) | Composite algorithmic score | -3 to +3 | <-3: hypocoagulable; >+3: hypercoagulable |
(Morgan & Mikhail's Clinical Anesthesiology 7e; Rockwood & Green's Fractures in Adults 10e; Scott-Brown's Otorhinolaryngology Vol.1)
ROTEM Equivalents:
| ROTEM Parameter | TEG Equivalent |
|---|---|
| CT (Clotting Time) | R time |
| CFT (Clot Formation Time) | K time |
| Alpha angle (α) | Alpha angle |
| MCF (Maximum Clot Firmness) | MA |
| LI30 / ML | LY30 |
ROTEM uses specific activator reagents: EXTEM (extrinsic pathway via tissue factor), INTEM (intrinsic pathway via ellagic acid), FIBTEM (extrinsic + platelet inhibitor cytochalasin D, isolating fibrinogen contribution), APTEM (extrinsic + aprotinin, detecting fibrinolysis).
3.3 TEG/ROTEM-Guided Transfusion Algorithms
The greatest clinical utility of VHAs is in goal-directed transfusion therapy, particularly in:
- Major trauma and haemorrhage - identifying trauma-induced coagulopathy (TIC), which is characterised by early hyperfibrinolysis, dilution, hypothermia, and acidosis (the "lethal triad")
- Cardiac surgery - distinguishing surgical from coagulopathic bleeding
- Liver transplantation - monitoring complex coagulopathy including hyperfibrinolysis
- Obstetric haemorrhage - real-time guidance for clotting factor replacement
- Neurosurgery - detecting hypercoagulability and guiding anticoagulation
Algorithmic use: prolonged R time → FFP or coagulation factor concentrates; reduced alpha/K time → cryoprecipitate or fibrinogen concentrate; reduced MA → platelet transfusion; elevated LY30 → tranexamic acid (TXA) or epsilon-aminocaproic acid. (Rockwood & Green's Fractures 10e; Morgan & Mikhail's Clinical Anesthesiology 7e)
3.4 Advantages over Standard Coagulation Tests
| Feature | PT / aPTT / CBC | TEG / ROTEM |
|---|---|---|
| Sample | Plasma only | Whole blood (includes platelets and RBCs) |
| Condition | Static | Dynamic |
| Time | 45-90 min | 20-30 min (functional result) |
| Fibrinolysis detected | No (directly) | Yes |
| Platelet function | No | Yes (via MA / MCF) |
| Hypercoagulability | No | Yes |
| POC availability | Limited | Yes |
Standard tests (PT, aPTT) do not detect hyperfibrinolysis, platelet dysfunction, qualitative fibrinogen defects, or hypercoagulability, and are performed on platelet-poor plasma under non-physiological conditions. TEG/ROTEM provide a global, dynamic, real-time haemostatic profile.
3.5 Limitations of TEG/ROTEM
- Temperature sensitivity: samples must be maintained at 37°C
- Inter-operator variability; time-sensitive sample processing required
- Do not assess endothelial function or vascular component of haemostasis
- Weak sensitivity for antiplatelet drugs (aspirin, ADP receptor inhibitors) - specific platelet mapping reagents needed
- ROTEM and TEG values are not interchangeable and have different reference ranges
- Evidence base predominantly from cardiac surgery; evidence in trauma and obstetrics is growing but certainty remains variable
- Cost and availability in lower-resource settings
4. Current Evidence (4 marks)
A 2026 Cochrane systematic review (Kvisselgaard et al., 35 RCTs, n=3096, mostly cardiac surgery) found TEG/ROTEM-guided transfusion may reduce all-cause mortality (RR 0.76, 95% CI 0.63-0.92), reduce bleeding volume, reduce FFP and platelet transfusion use, and reduce surgical re-exploration, but noted the evidence is of very low certainty. No benefit in packed red blood cell use was demonstrated. This is consistent with earlier systematic reviews cited in Morgan & Mikhail and Goldman-Cecil Medicine (Anaesthesia 2017;72:519-531). The evidence is strongest for cardiac surgery, with emerging data in trauma, liver transplantation, and obstetrics.
5. Anaesthetic Relevance - Practical Summary (marks incorporated above)
The anaesthetist must:
- Understand the cell-based model rather than the classical cascade alone, to interpret the clinical significance of factor deficiencies and guide replacement
- Recognise the limitations of PT/aPTT: normal values do not exclude coagulopathy, and they do not detect fibrinolysis or platelet dysfunction
- Use TEG/ROTEM as decision support tools within a goal-directed algorithm, not as isolated tests
- Apply tranexamic acid early in high-risk haemorrhage (CRASH-2 / WOMAN trial evidence), as TEG-confirmed hyperfibrinolysis (LY30 >7.5%) indicates further benefit
- Account for the confounders of anaesthesia on haemostasis: hypothermia impairs enzymatic reactions and platelet function; acidosis disrupts the coagulation factor environment; haemodilution reduces factor and platelet concentrations - all components of the lethal triad in major haemorrhage
Summary Table
| Aspect | Key Points |
|---|---|
| Classical cascade | Extrinsic (TF-FVII) + Intrinsic (contact, FXII) → common pathway (FXa, prothrombin → thrombin → fibrin) |
| Cell-based model | Initiation (TF cells) → Amplification (platelets) → Propagation (platelet surface) |
| Thrombin | Central mediator: fibrinogen cleavage, FXIII activation, platelet activation (PAR-1), feedback activation of FV/FVIII/FXI |
| Anticoagulants | ATIII, TFPI, Protein C/S, PGI2/NO |
| Fibrinolysis | t-PA → plasmin → fibrin degradation; D-dimers as markers |
| TEG/ROTEM | Global viscoelastic assay: R/CT (factors) → K/CFT + alpha (fibrinogen) → MA/MCF (platelets) → LY30/LI30 (fibrinolysis) |
| Clinical use | Goal-directed transfusion in cardiac surgery, trauma, liver Tx, obstetrics |
| Evidence | Cochrane 2026 (35 RCTs): possible mortality reduction, reduced blood product use; very low certainty evidence |
Word count: ~1,800 | Sources: Robbins Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22E; Sabiston Textbook of Surgery; Morgan & Mikhail's Clinical Anesthesiology 7e; Schwartz's Principles of Surgery 11e; Rockwood & Green's Fractures in Adults 10e; Scott-Brown's Otorhinolaryngology Vol.1; Goldman-Cecil Medicine; Kvisselgaard et al. Cochrane Database Syst Rev 2026 [PMID: 42145275]
Convert the above answer in a pdf
Reading File
Running Command
Running Command
Writing File
Running Command
Running Command
Your PDF is ready (827 KB). Download it here:
Coagulation Cascade and TEG Exam Answer
PDF Document · PDF
What's included in the PDF:
- Navy header and footer on every page with page numbers
- Colour-coded section banners for each of the 5 sections
- Both textbook diagrams embedded (coagulation cascade figure + annotated TEG trace)
- All formatted tables: TEG/ROTEM parameters, ROTEM equivalents, anticoagulant mechanisms, goal-directed algorithm, advantages vs. standard tests, and summary table
- Cell-based model displayed as a highlighted three-phase table
- Full reference list with Cochrane 2026 citation (PMID: 42145275)
- Optimised for A4 printing
Create a quick reference laminated TEG/ROTEM interpretation card for theatre use
Running Command
Writing File
Running Command
Editing File
Running Command
Writing File
Running Command
Running Command
Running Command
Your theatre card is ready (233 KB). Download here:
TEG ROTEM Theatre Card
PDF Document · PDF
How to use it:
- Print on A4 paper, landscape orientation, at 100% scale
- Cut along the centre line (marked with a thin grey rule)
- Laminate each half - you get two A5-landscape cards
What's on each side:
Side A - Parameters
- Annotated TEG trace diagram (R · K · α · MA · LY30 labelled)
- Full TEG parameters table with normal ranges and immediate actions
- TEG ↔ ROTEM equivalents table
- Colour-coded ROTEM reagent key (EXTEM · INTEM · FIBTEM · APTEM)
Side B - Algorithm
- Goal-directed intervention table: VHA finding → likely defect → TEG parameter → ROTEM parameter → what to give (colour-coded rows: green=FFP, amber=cryo, red=TXA, purple=mixed deficit)
- Drug and condition effects on VHA (heparin, warfarin, DOACs, aspirin, P2Y12 inhibitors, TXA, hypothermia, DIC)
- Lethal triad summary with clinical context priority list
- Evidence footnote from Cochrane 2026 (PMID: 42145275)
Generate a 30 marks answer for Postgraduate Anaesthesia exam on the topic of Ultrasound in Anaesthesia with diagrams
Reading File
Finding Sources
Finding Sources
Searching PubMed
ultrasound guided regional anesthesia outcomes
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have extensive content and real textbook images from Miller's Anesthesia. Let me now write the comprehensive exam answer.
Ultrasound in Anaesthesia
Postgraduate Anaesthesia Examination Answer (30 Marks)
1. Introduction (2 marks)
Ultrasound has transformed anaesthetic practice over the past three decades, shifting it from landmark-based, empirical technique to real-time, image-guided precision. Its applications span the entire perioperative period: preoperative assessment, vascular access, regional anaesthesia, airway management, haemodynamic monitoring, and critical care. The result is improved procedural success rates, reduced complications, and better patient outcomes. Proficiency in point-of-care ultrasound (POCUS) is now considered a core competency for anaesthetists.
2. Physics of Ultrasound (4 marks)
2.1 Basic Principles
Ultrasound uses sound waves with frequencies above 20 kHz - clinical imaging uses 2-15 MHz. The fundamental relationship governing resolution and penetration is:
Wave speed (c) = Frequency (f) × Wavelength (λ)
In soft tissue, sound travels at approximately 1540 m/s. The transducer acts both as emitter and receiver (pulse-echo principle).
Key trade-off:
- High frequency (10-15 MHz): Superior spatial resolution, poor tissue penetration (shallow structures - nerve blocks, vascular access)
- Low frequency (2-5 MHz): Poor resolution, deep penetration (cardiac, abdominal, deep vessels)
2.2 Piezoelectric Effect
The piezoelectric crystal within the transducer converts electrical energy into sound waves (transmit) and back into electrical signals (receive). This crystal deforms when voltage is applied, generating pressure waves, and generates voltage when deformed by returning echoes.
2.3 Image Generation
Returning echoes are processed according to their:
- Amplitude (brightness - creating the B-mode greyscale image)
- Time of arrival (used to calculate depth: depth = c × time/2)
Echogenicity terminology:
| Term | Appearance | Example |
|---|---|---|
| Hyperechoic | Bright white | Bone cortex, needle, fascia |
| Hypoechoic | Dark grey | Muscle, nerve, solid organ |
| Anechoic | Black | Fluid (blood, urine, effusion) |
| Isoechoic | Same as surrounding tissue | Thrombus (fresh) |
2.4 Imaging Modes
| Mode | Description | Clinical Use in Anaesthesia |
|---|---|---|
| B-mode (2D) | Brightness-based greyscale cross-section | Standard imaging for all procedures |
| M-mode | Single-line motion over time | Lung sliding ("seashore sign"), IVC diameter |
| Colour Doppler | Direction and velocity of flow (colour-coded) | Distinguish vein from artery |
| Pulsed wave Doppler | Flow velocity at a specific depth | Cardiac output, stenosis grading |
| Power Doppler | Sensitive low-flow detection | Confirm vessel patency |
2.5 Artefacts
Understanding artefacts is essential to avoid misinterpretation:
| Artefact | Cause | Significance |
|---|---|---|
| Acoustic shadowing | Bone/air blocks beam | Confirms calcification or gas |
| Posterior acoustic enhancement | Fluid transmits beam | Confirms fluid-filled structure |
| Reverberation / A-lines | Repeated reflections between two surfaces | Normal lung; horizontal bright parallel lines |
| B-lines (comet tail) | Fluid in interlobular septa | Pulmonary oedema, ARDS |
| Mirror artefact | Strong reflector duplicates image | Diaphragm-liver interface |
| Anisotropy | Angle-dependent reflectance of tendons/nerves | Nerve appears less echogenic off-axis |
3. Needle Guidance Techniques (2 marks)
Two principal approaches exist for needle insertion under ultrasound guidance:
In-plane (longitudinal approach):
- Needle inserted parallel to the transducer's long axis
- Entire needle shaft and tip visualised as a hyperechoic line
- Preferred for nerve blocks (full needle course visible, safer)
Out-of-plane (transverse approach):
- Needle inserted perpendicular to the probe
- Only needle tip (or shaft cross-section) seen as a bright dot
- Risk of mistaking shaft for tip - "tip tracking" techniques required
- Preferred for central venous cannulation (short access distance)
Needle echogenicity is enhanced by: echogenic coatings, stylets, increased needle gauge, and oblique cutting of the bevel.
4. Vascular Access (5 marks)
4.1 Central Venous Cannulation
Ultrasound-guided central venous catheterisation (CVC) is now the standard of care, with level 1B evidence from the European Society of Anaesthesiology. The Agency for Healthcare Research and Quality (AHRQ) lists ultrasound as one of 11 practices clinicians should adopt for central venous access. (Miller's Anesthesia 10e)
Internal jugular vein (IJV):
- Probe placed transversely at the level of the thyroid cartilage
- IJV: compressible, oval, lateral to the common carotid artery
- Carotid artery: non-compressible, round, pulsatile, with colour Doppler confirming arterial flow
- The out-of-plane approach is most commonly used; the in-plane approach visualises the entire needle course
Key advantages:
- Reduces arterial puncture risk from ~6.3% (landmark) to <1%
- Reduces haematoma, pneumothorax, and overall complication rate
- Particularly beneficial in: obesity, coagulopathy, abnormal anatomy, previously attempted sites
- Subclavian approach - linear probe in infraclavicular fossa; ultrasound guidance reduces pneumothorax risk but is technically more demanding
- Femoral approach - useful in coagulopathic patients; ultrasound identifies femoral vein medial to femoral artery
4.2 Arterial Cannulation
Systematic review of 11 RCTs comparing radial artery cannulation with and without ultrasound: significantly improved first-attempt success and reduced total attempts in the ultrasound-guided group. (Miller's Anesthesia 10e)
Additional benefit: absence of Doppler flow in the superficial palmar branch on radial occlusion indicates inadequate ulnar collateral circulation - a contraindication to radial cannulation.
4.3 Peripheral Venous Access
Ultrasound-guided peripheral IV access is invaluable in patients with difficult peripheral access (obesity, scar tissue, prior cannulation, intravenous drug use). Long-axis in-plane technique preferred; 18G-20G cannulae inserted into the basilic or cephalic vein of the upper arm.
5. Ultrasound-Guided Regional Anaesthesia (6 marks)
5.1 Historical Context and Evidence
La Grange et al. reported the first use of ultrasound for neural blockade in 1978. Since then, ultrasound-guided nerve blocks have become standard practice, shown to be quicker, more precise, with lower complication rates and higher patient satisfaction. They have transformed enhanced recovery after surgery (ERAS) pathways, reduced length of hospital stay, and improved outcomes. (Miller's Anesthesia 10e)
A 2009 systematic review and meta-analysis comparing ultrasound guidance with electrical neurostimulation for peripheral nerve blocks demonstrated reduced block performance time, improved block quality, and reduced complications with ultrasound (Br J Anaesth. 2009;102:408-417, cited in Miller's Anesthesia 10e).
5.2 Advantages over Nerve Stimulator Technique
| Feature | Nerve Stimulator | Ultrasound Guided |
|---|---|---|
| Real-time visualisation | No | Yes |
| Needle-nerve relationship | Indirect (electrical) | Direct visual |
| Local anaesthetic spread | Not seen | Visualised in real time |
| Intravascular injection detection | No | Yes (Doppler) |
| Intraneural injection warning | No | Yes (nerve swelling) |
| Deep block accuracy | Variable | Improved |
| Effectiveness in patients with neuropathy | Reduced | Maintained |
5.3 Nerve Sonoanatomy
Nerve appearance on ultrasound: Nerves appear as honeycomb structures in cross-section - multiple round hypoechoic fascicles surrounded by hyperechoic perineurium and epineurium. In longitudinal section they appear as parallel echogenic lines ("tram tracks"). Anisotropy must be considered - nerves appear less echogenic when the beam is not perpendicular to them.
5.4 Common Blocks in Anaesthetic Practice
Upper limb:
- Interscalene brachial plexus block - roots C5/C6/C7 visualised between anterior and middle scalene muscles at C6 level. Used for shoulder surgery. Risk: phrenic nerve paralysis (ipsilateral hemidiaphragm palsy in 100% - avoid bilateral or in severe respiratory compromise).
- Supraclavicular block - trunks/divisions of brachial plexus at the first rib, around the subclavian artery. "Cluster of grapes" appearance. Dense forearm and hand block.
- Infraclavicular block - cords around the axillary artery in the infraclavicular fossa. Lateral, posterior, medial cords identified at 9, 6, and 3 o'clock positions respectively.
- Axillary block - terminal branches (radial, ulnar, median, musculocutaneous) identified around the axillary artery. Multiple injections required.
Lower limb:
- Femoral nerve block - nerve lies lateral to femoral artery, deep to fascia iliaca. Used for hip fracture analgesia, anterior knee surgery.
- Adductor canal block (ACB) - saphenous nerve in the adductor canal, mid-thigh. Motor-sparing alternative to femoral nerve block for knee arthroplasty analgesia - preserves quadriceps strength.
- Popliteal sciatic nerve block - sciatic nerve bifurcation above the popliteal crease. Used for foot/ankle surgery.
Truncal blocks:
- Transversus abdominis plane (TAP) block - local anaesthetic deposited between internal oblique and transversus abdominis muscles. Provides somatic (not visceral) analgesia for abdominal wall; T7-L1 coverage depending on approach.
- Erector spinae plane (ESP) block - injection into the plane deep to erector spinae, over transverse process. Covers both somatic and visceral pain via paravertebral spread. Used for thoracic, abdominal, and rib fracture analgesia.
- Serratus anterior plane (SAP) block - between serratus anterior and either the latissimus dorsi (superficial) or the ribs (deep). T2-T9 coverage - used for thoracic surgery, rib fractures, mastectomy.
- Rectus sheath block - between rectus abdominis and posterior rectus sheath. Bilateral blocks provide midline abdominal wall analgesia.
5.5 Local Anaesthetic Systemic Toxicity (LAST) Prevention
Real-time visualisation of local anaesthetic spread, combined with aspiration before injection, allows detection of intravascular needle placement. Colour Doppler confirms vascular proximity. Reduced volumes of local anaesthetic are required with ultrasound guidance (precise placement reduces the need for high volumes), thereby lowering LAST risk.
6. Point-of-Care Cardiac Ultrasound (POCUS) (5 marks)
6.1 Focused Cardiac Ultrasound (FoCUS)
FoCUS is a targeted, binary (yes/no) cardiac assessment performed by the anaesthetist at the bedside - distinct from formal echocardiography performed by cardiologists. It answers specific clinical questions and guides immediate management.
Core FoCUS views:
| View | Probe Position | Structures Assessed |
|---|---|---|
| Parasternal long axis (PLAX) | Left parasternal, 3rd/4th ICS | LV size, wall motion, MV, AV, pericardial effusion |
| Parasternal short axis (PSAX) | Left parasternal, rotated 90° | LV end-diastolic area, RV:LV ratio, wall motion |
| Apical 4-chamber | Cardiac apex | Biventricular size and function, valves, effusion |
| Subcostal 4-chamber | Subxiphoid | RV/LV, pericardial effusion (tamponade), IVC |
| IVC long axis | Subcostal | Volume status: IVC collapsibility >50% = hypovolaemia |
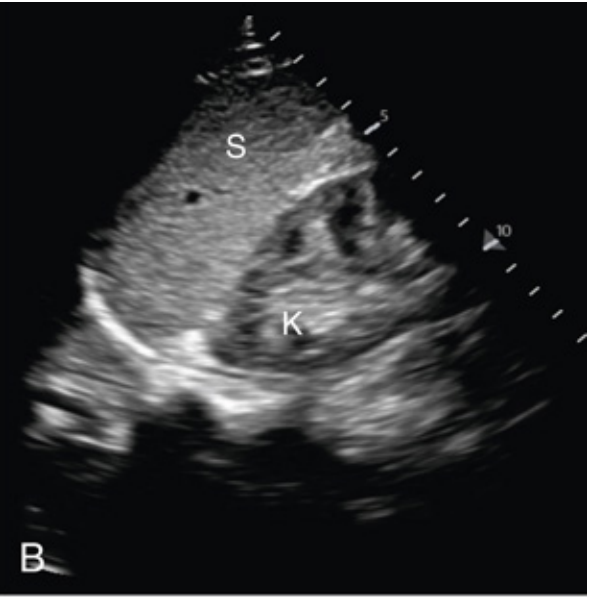
Fig. 1 - Subcostal echocardiographic view: S = stomach/right ventricle side, K = left ventricle. Used to assess biventricular function and pericardial effusion. (Miller's Anesthesia 10e)
6.2 Clinical Applications of FoCUS in Anaesthesia
Preoperative:
- Rapid assessment of ventricular function before emergency/urgent surgery
- Detection of pericardial effusion or tamponade
- Preoperative cardiac risk stratification (hip fracture patients - delay for echocardiography associated with increased mortality)
- ROSE protocol (Rapid Obstetric Screening Echocardiography) for haemodynamically unstable obstetric patients
Intraoperative:
- Feasible in >90% of surgical cases (Miller's Anesthesia 10e)
- Impacts management in 22-66% of intraoperative uses
- Differentiation of shock subtypes (hypovolaemic, cardiogenic, distributive, obstructive)
- Detection of acute right heart strain (pulmonary embolism - D-shaped interventricular septum)
- Monitoring response to fluid resuscitation
Perioperative haemodynamic assessment:
- IVC diameter and collapsibility: IVC <1.5 cm with >50% inspiratory collapse = hypovolaemia; IVC >2.5 cm with <25% collapse = volume overload / raised CVP
- LV end-diastolic area (LVEDA): Reduced (<10 cm²) = hypovolaemia ("kissing ventricles" in severe hypovolaemia); elevated = volume overload or poor function
- Visually estimated LVEF: Reduced (<30%) = severe cardiogenic dysfunction
6.3 Transoesophageal Echocardiography (TOE)
TOE provides superior image quality compared to transthoracic echo due to proximity of the transducer to the heart. Performed under GA or deep sedation. It is the gold standard for:
- Intraoperative cardiac surgical monitoring
- Assessment of aortic disease, valve pathology
- Detection of intracardiac thrombus/air
- Monitoring after cardiopulmonary bypass (assessment of de-airing)
7. Lung Ultrasound (3 marks)
7.1 Principles
Normal aerated lung reflects ultrasound at the pleural interface, generating characteristic artefacts.
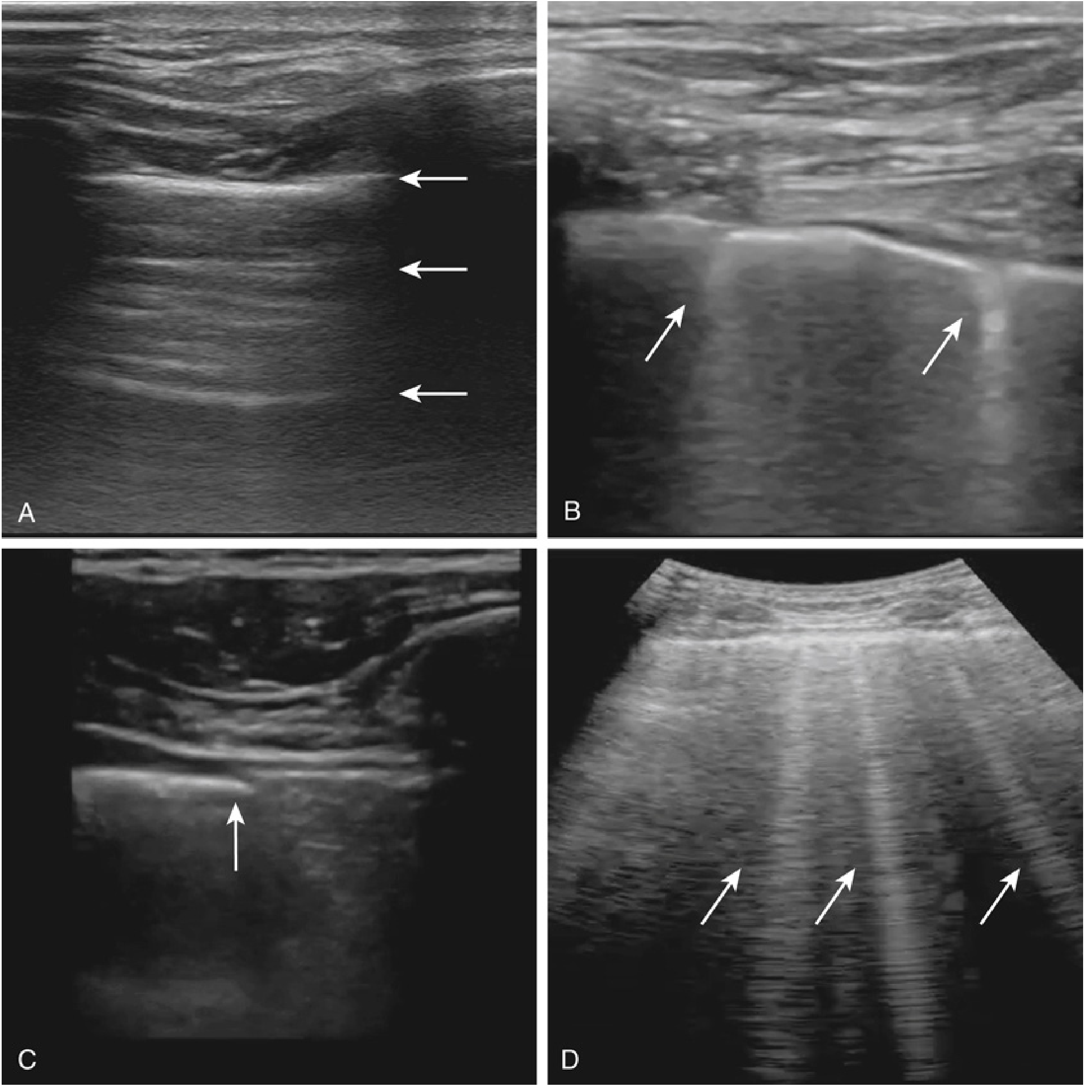
Fig. 2 - Lung ultrasound findings. (A) A-lines: horizontal repetitive artefacts - normal aeration. (B) Z-lines: short B-lines, often normal. (C) Lung point: highly specific for pneumothorax - transition between sliding and non-sliding. (D) Pathological B-lines: comet-tail artefacts indicating interstitial fluid (pulmonary oedema). (Miller's Anesthesia 10e)
Key findings:
| Finding | Appearance | Significance |
|---|---|---|
| A-lines | Horizontal regularly spaced bright lines | Normal lung - aeration present |
| Lung sliding | Shimmering motion at pleural line | Pleural surfaces in apposition (normal) |
| B-lines ("rockets") | Vertical comet-tail artefacts reaching screen edge | Interstitial fluid: pulmonary oedema, ARDS |
| Lung point | Transition between sliding and non-sliding | Highly specific for pneumothorax |
| Absent lung sliding | No pleural movement | Pneumothorax, apnoea, mainstem intubation |
| "Seashore sign" (M-mode) | Granular pattern below pleural line | Normal lung sliding present |
| "Barcode sign" (M-mode) | Parallel lines throughout | Pneumothorax (absent lung sliding) |
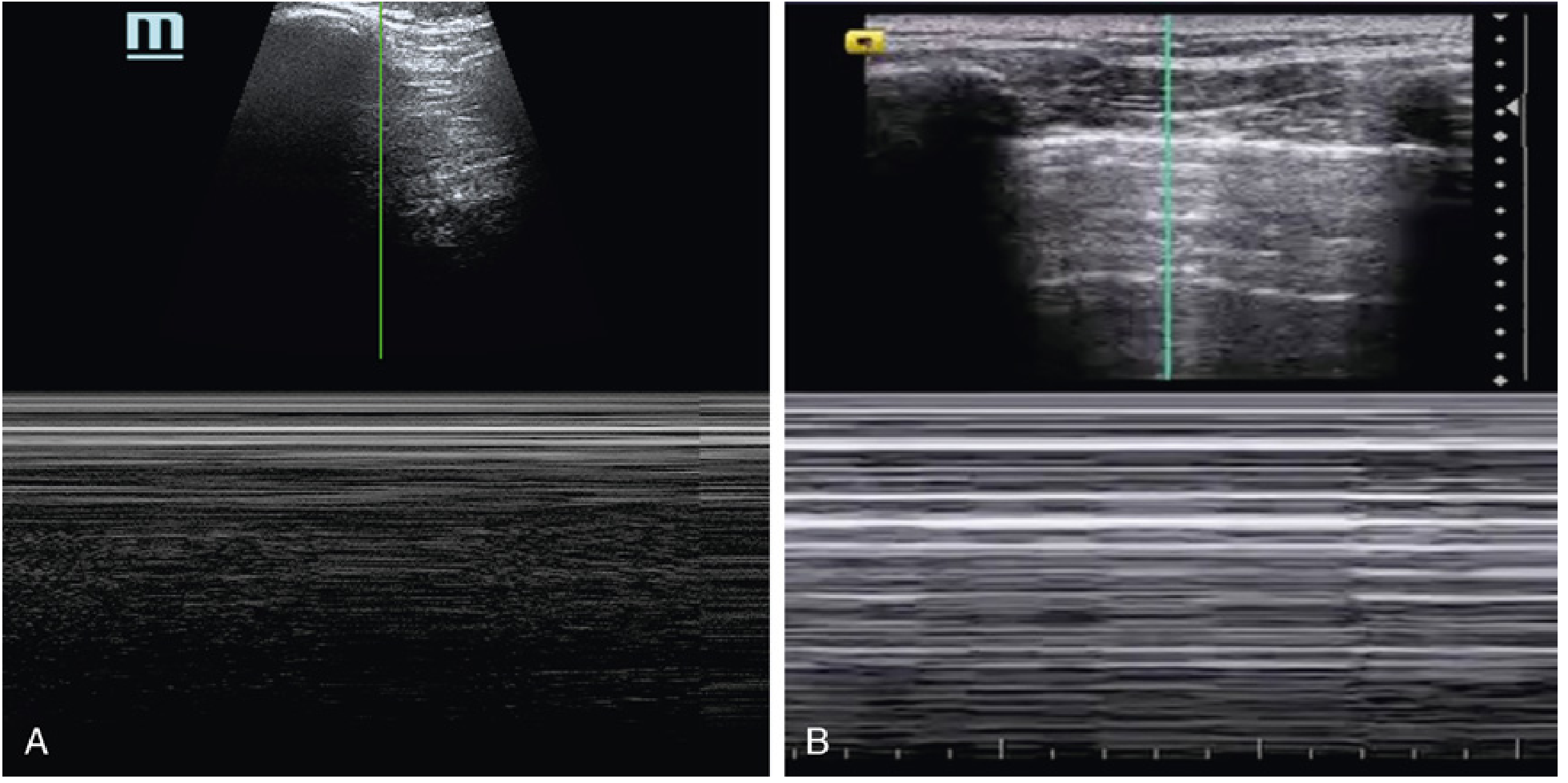
Fig. 3 - M-mode lung ultrasound. (A) Normal "seashore sign" - granular pattern below pleural line indicates lung sliding. (B) Absence of seashore pattern in pneumothorax. (Miller's Anesthesia 10e)
7.2 Pneumothorax Detection
Lung ultrasound predicts absence of pneumothorax with 93.8% sensitivity and 99.9% negative predictive value, superior to chest X-ray. (Miller's Anesthesia 10e). The lung point is pathognomonic for pneumothorax - the precise transition point between free air and lung contact.
7.3 eFAST (Extended Focused Assessment with Sonography for Trauma)
eFAST extends the traditional FAST exam (abdominal free fluid) to include thoracic assessment.
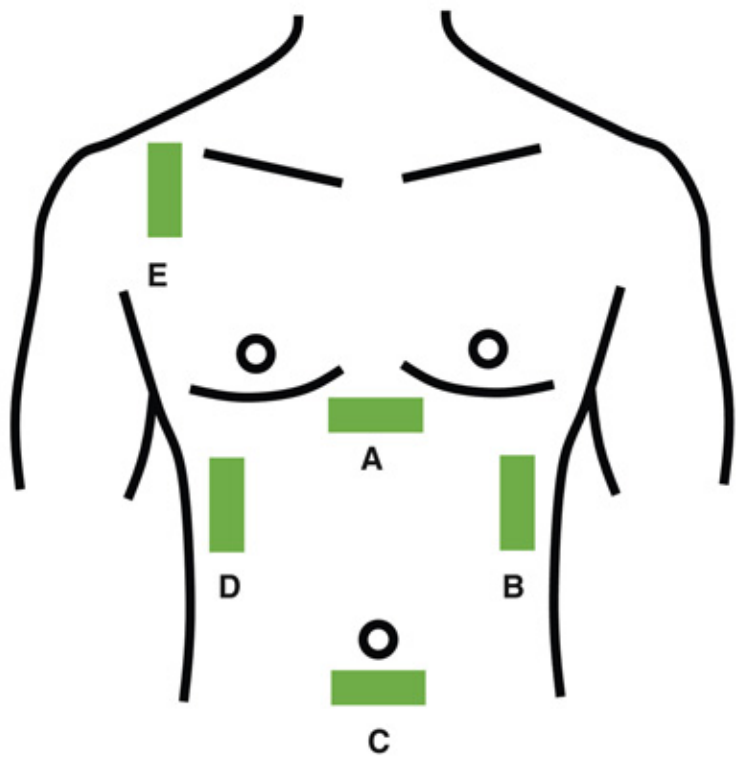
Fig. 4 - eFAST exam probe positions. A = subcostal (pericardial effusion), B = left upper quadrant, C = pelvic (free fluid), D = right upper quadrant (Morrison's pouch), E = thoracic (pneumothorax/haemothorax). (Miller's Anesthesia 10e)
eFAST components:
- Pericardial view (subcostal): pericardial effusion, tamponade
- Right upper quadrant (Morrison's pouch): hepatorenal free fluid
- Left upper quadrant (splenorenal): free fluid
- Pelvic view (bladder): pelvic free fluid
- Bilateral thoracic views: haemothorax (anechoic fluid above diaphragm), pneumothorax (absent lung sliding)
8. Airway Assessment (2 marks)
8.1 Gastric Ultrasound
A full stomach is defined as identification of solid food or presence of more than 1.5 mL/kg of clear liquid calculated by measuring the gastric antral cross-sectional area (CSA). The formula used is:
Gastric volume (mL) = 27.0 + 14.6 × right-lateral CSA − 1.28 × age
Solid content appears as heterogeneous, echogenic material with posterior acoustic shadowing ("frosted glass" appearance). Clear fluid appears anechoic. This assessment is particularly valuable in emergency surgery where aspiration risk is uncertain (trauma patients, delayed gastric emptying, uncertain fasting status).
8.2 Tracheal/Laryngeal Ultrasound
- Identifies tracheal midline for confirmation of endotracheal tube position (bilateral lung sliding confirms bilateral ventilation)
- Detects supraglottic structures for awake intubation planning
- Measures subglottic diameter to guide endotracheal tube selection (particularly in paediatric anaesthesia)
- Identifies cricothyroid membrane for emergency front-of-neck access (FONA) - the CTM is located between the thyroid and cricoid cartilages as a hypoechoic gap between two hyperechoic cartilaginous structures
9. Limitations, Training and Governance (2 marks)
9.1 Limitations
- Operator dependency: Image quality and interpretation are directly proportional to skill
- Acoustic windows: Obesity, subcutaneous emphysema, and dressings impair imaging
- Learning curve: Requires dedicated structured training; misinterpretation can cause harm (e.g., mistaking a thrombus for patent vessel, intraneural injection not prevented)
- Equipment: High-quality machines are expensive; portable devices have limitations
- POCUS does not replace formal echocardiography - a negative focused assessment does not exclude all cardiac pathology
- Anaesthetic interference: General anaesthesia, positive pressure ventilation, and the sterile surgical field complicate intraoperative use
- No standardisation: TEE values and POCUS reference ranges vary between institutions
9.2 Training and Competency
The Association of Anaesthetists of Great Britain and Ireland (AAGBI) and British Society of Echocardiography (BSE) have published guidelines for credentialing. Levels of competency range from:
- Level 1: Basic POCUS (cardiac, lung, vascular access) - expected of all anaesthetists
- Level 2: Advanced perioperative echocardiography
- Level 3: Expert / diagnostic TOE for complex cardiac surgery
Barriers to adoption include lack of training (most commonly cited), lack of equipment, and absence of formal credentialling pathways. (Miller's Anesthesia 10e)
10. Summary Table (marks incorporated above)
| Application | Probe | Frequency | Key Benefit |
|---|---|---|---|
| Central venous access (IJV) | Linear | 10-15 MHz | ↓ arterial puncture, ↓ pneumothorax |
| Arterial cannulation | Linear | 10-15 MHz | ↑ first-attempt success |
| Nerve blocks (superficial) | Linear | 10-15 MHz | Direct visualisation, ↓ LAST |
| Nerve blocks (deep - e.g., femoral) | Curved/Linear | 5-10 MHz | Depth penetration |
| Cardiac (FoCUS/TOE) | Phased array | 2-5 MHz | Haemodynamic assessment |
| Lung | Curved/Linear | 2-10 MHz | Pneumothorax, effusion, oedema |
| Gastric assessment | Curved | 2-5 MHz | Aspiration risk |
| Airway/CTM | Linear | 10-15 MHz | FONA planning |
References
- Miller RD et al. Miller's Anesthesia, 10th ed. Elsevier, 2023 - Chapter 33 (Monitoring), Chapter 42 (Regional Anaesthesia)
- Barash PG et al. Clinical Anesthesia, 9th ed. Wolters Kluwer, 2022
- European Society of Anaesthesiology Guidelines for Central Venous Access (1B evidence for IJV ultrasound guidance)
- Agency for Healthcare Research and Quality. Making Health Care Safer - 11 practices including ultrasound for CVC
- Koscielniak-Nielsen ZJ. Ultrasound-guided peripheral nerve blocks: what are the benefits? Acta Anaesthesiol Scand. 2008
- Pietroski Dos Santos N et al. Systemic review with meta-analysis: long-acting vs mixed local anaesthetics for US-guided peripheral nerve blocks. Reg Anesth Pain Med. 2026 [PMID: 39779278]
- La Grange P, Foster PA, Pretorius LK. Application of the Doppler ultrasound blood-flow detector. Br J Anaesth. 1978
This is a shared conversation. Sign in to Orris to start your own chat.