Let's analysis 4th ventricle of brain in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
I now have more than enough comprehensive content from multiple authoritative textbooks to write a thorough analysis. Let me compile the full response.
The Fourth Ventricle - A Detailed Analysis
Overview
The fourth ventricle is the most caudal of the four brain ventricles. It occupies the posterior cranial fossa, situated between the brainstem anteriorly and the cerebellum posteriorly. It is the key transit point for CSF flowing from the cerebral aqueduct to the subarachnoid space.
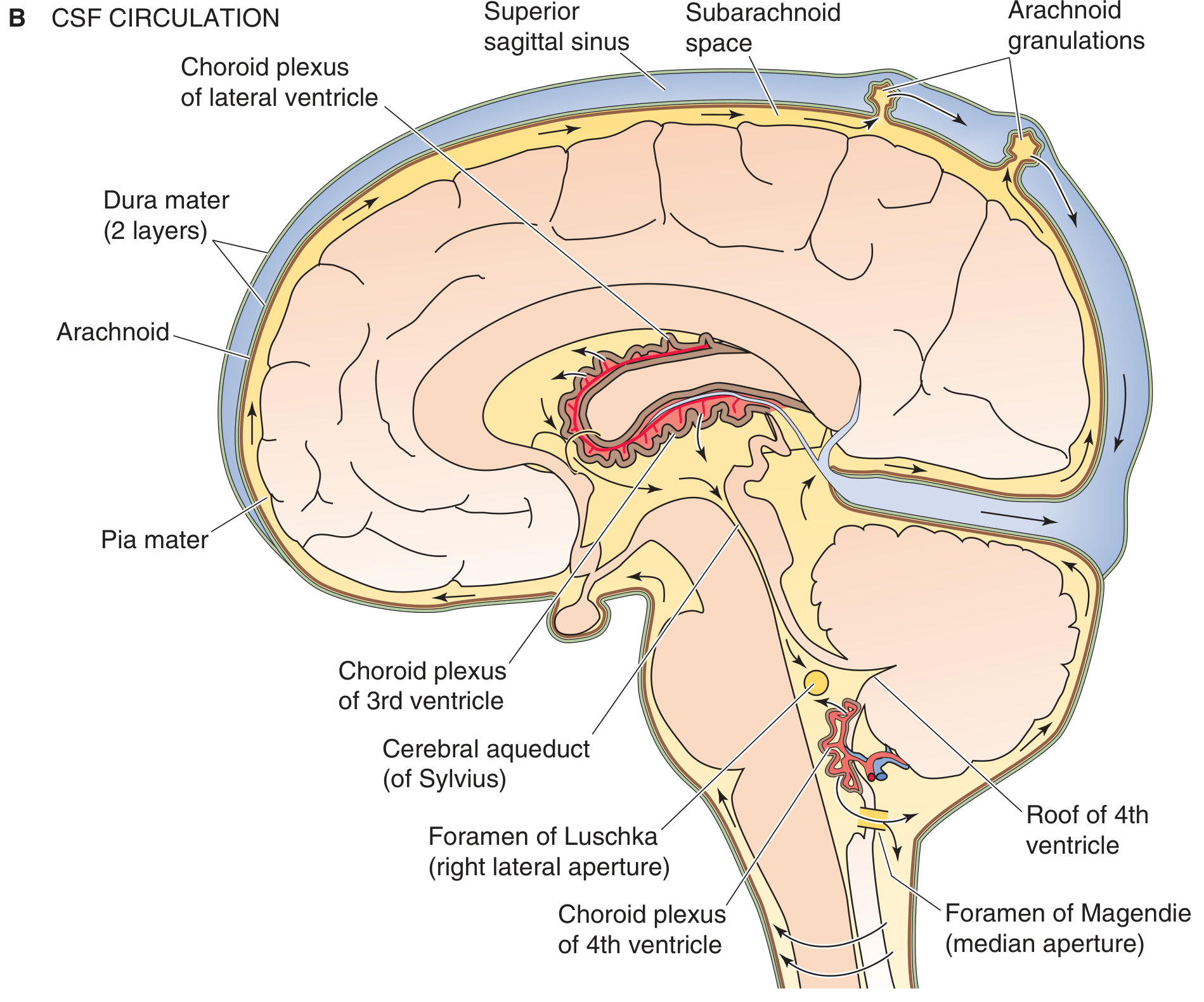
CSF circulation - the fourth ventricle and its connections (Medical Physiology)
1. Location and Anatomical Position
The fourth ventricle is located within the pons, medulla, and cerebellum. Specifically:
- It is bounded superiorly/posteriorly by the cerebellum
- Inferiorly/anteriorly by the pons and medulla oblongata
- It extends rostrally to join the cerebral aqueduct of Sylvius (connecting it to the third ventricle)
- It tapers caudally to the obex, which marks the entry point to the spinal cord's central canal (closed in adults)
- Neuroanatomy through Clinical Cases, 3rd Edition
2. Shape and Subdivisions
The fourth ventricle has a characteristic tent-shaped or diamond (rhomboid) shape when viewed from above (hence the name "rhomboid fossa" for its floor):
- Fastigium: the apex/peak of the tent shape, visible as a pointed superior recess on sagittal imaging
- Lateral recesses: paired pockets that extend laterally into the cerebellopontine angle region and funnel into the foramina of Luschka
- Rhomboid fossa: the floor, shaped like a diamond
- Grainger & Allison's Diagnostic Radiology
3. Boundaries
| Wall | Structure Forming It |
|---|---|
| Roof (posterior wall) | Cerebellum (superior and inferior medullary vela) |
| Floor (anterior wall) | Pons (rostral portion) and medulla oblongata (caudal portion) |
| Lateral walls | Superior, middle, and inferior cerebellar peduncles |
4. The Floor of the Fourth Ventricle (Rhomboid Fossa)
This is the most clinically significant surface. The floor extends from the pons to the rostral half of the medulla. Several visible surface landmarks overlie important cranial nerve nuclei:
- Facial colliculi - bilateral bumps formed by the abducens nucleus (CN VI) and looping fibers of the facial nerve (CN VII)
- Hypoglossal trigone - overlies the hypoglossal nucleus (CN XII)
- Vagal trigone - overlies the dorsal motor nucleus of the vagus nerve (CN X)
- Sulcus limitans - a longitudinal groove separating the medial alar plate (sensory) from the basal plate (motor)
- Medial eminence - a longitudinal ridge medial to the sulcus limitans
The floor thus provides a surface map to the nuclei of cranial nerves V, VI, VII, VIII, IX, X, and XII.
- Neuroanatomy through Clinical Cases, 3rd Edition
5. The Roof of the Fourth Ventricle
The roof is formed by:
- Superior medullary velum (rostral part) - a thin white matter sheet between the superior cerebellar peduncles
- Inferior medullary velum (caudal part)
- Tela choroidea - a vascular pia-ependymal membrane formed by the thin ependymal roof covered externally by pia mater
The tela choroidea invaginates to form the choroid plexus of the fourth ventricle through active proliferation of the pia mater. The embryonic roof of the fourth ventricle evaginates at three locations, which then rupture to form the foramina (apertures).
- The Developing Human: Clinically Oriented Embryology
6. Foramina (Apertures) - CSF Exit Routes
The fourth ventricle has three openings through which CSF exits into the subarachnoid space:
| Foramen | Position | Drains Into |
|---|---|---|
| Foramen of Magendie (median aperture) | Single midline opening in the caudal roof | Cisterna magna (cerebellomedullary cistern) |
| Foramina of Luschka (lateral apertures) | Two lateral openings via lateral recesses | Cerebellopontine cisterns |
CSF pathway:
Lateral ventricles → foramina of Monro → third ventricle → aqueduct of Sylvius → fourth ventricle → foramina of Magendie & Luschka → subarachnoid space → arachnoid granulations → dural venous sinuses
- Medical Physiology; Morgan and Mikhail's Clinical Anesthesiology, 7e
7. Choroid Plexus of the Fourth Ventricle
The choroid plexus of the fourth ventricle:
- Lies along only a portion of the tent-shaped roof (not the entire roof)
- Extends laterally into both foramina of Luschka, often projecting into the subarachnoid space (visible on CT as calcified tufts in older adults)
- Blood supply comes from branches of three cerebellar arteries:
- PICA (posterior inferior cerebellar artery) - primary supply
- AICA (anterior inferior cerebellar artery)
- SCA (superior cerebellar artery)
- Grainger & Allison's Diagnostic Radiology
8. CSF Production and Composition
- Normal CSF production: ~21 mL/hour (500 mL/day); total CSF volume ~150 mL
- Primarily secreted by choroid plexus (active sodium secretion drives isotonic fluid production)
- CSF is isotonic with plasma but has lower K+, HCO3-, and glucose, and very low protein
- The fourth ventricle drains into the cisterna magna, after which CSF circulates around brain and spinal cord before absorption at arachnoid granulations over the cerebral hemispheres
Note: Whether true unidirectional "circulation" of CSF exists is currently debated in the literature.
- Morgan and Mikhail's Clinical Anesthesiology, 7e
9. Radiological Appearance
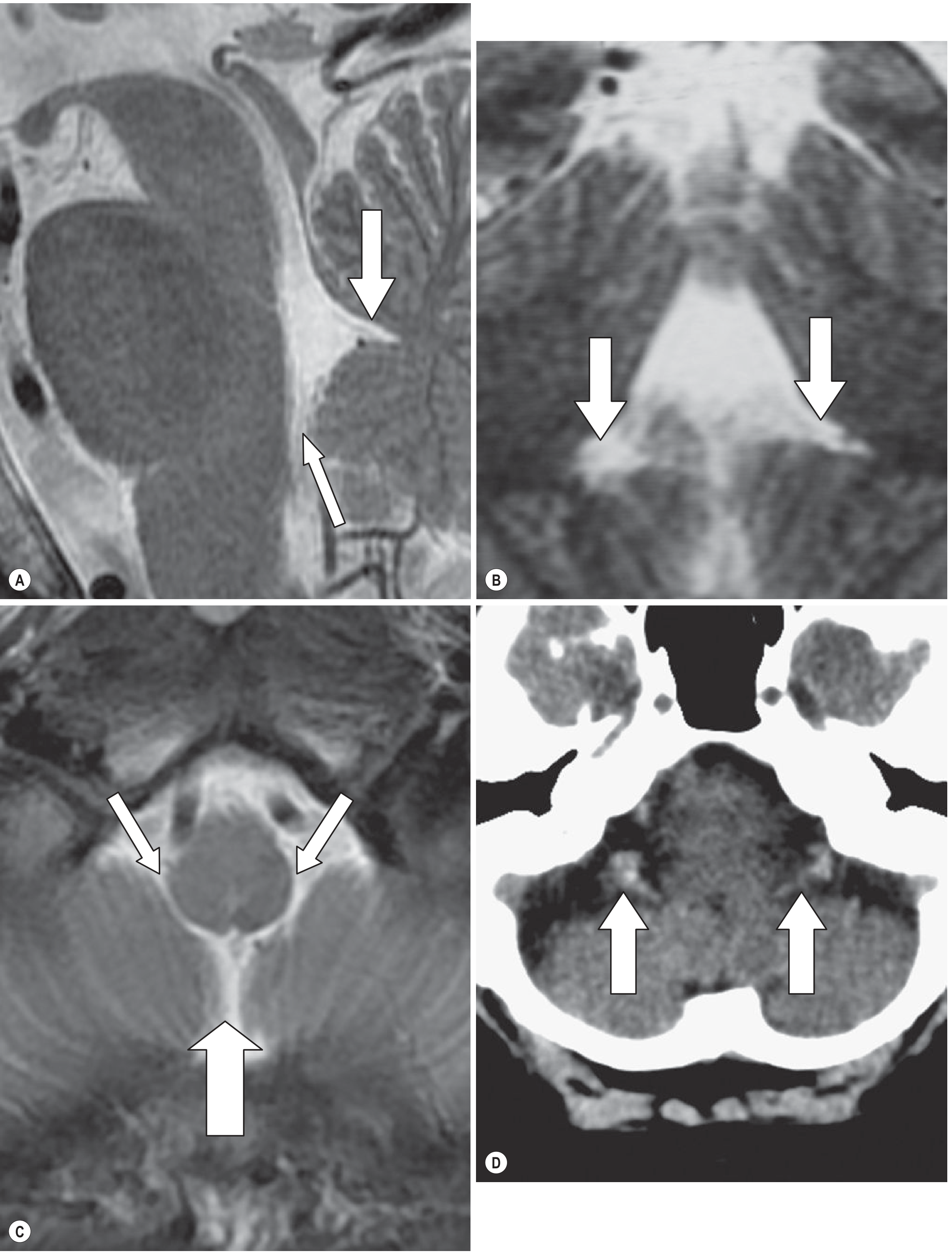
MRI/CT of the fourth ventricle: (A) Sagittal T2 showing fastigium (large arrow) and foramen of Magendie (small arrow); (B) Coronal image showing rhomboid shape and lateral recesses; (C) Axial MR showing foramen of Magendie (large arrow) and foramina of Luschka (small arrows); (D) CT showing calcified choroid plexus tufts projecting through the foramina of Luschka.
Key imaging features:
- Sagittal MRI: shows the tented apex (fastigium), the CSF flow void in the aqueduct, and the foramen of Magendie
- Coronal MRI: demonstrates the rhomboid shape and lateral recesses
- Axial MRI/CT: shows all three foramina and any calcification of the choroid plexus
- Grainger & Allison's Diagnostic Radiology
10. Embryological Development
The fourth ventricle develops from the rhombencephalon (hindbrain):
- The metencephalon (upper hindbrain) gives rise to the pons and cerebellum
- The myelencephalon (lower hindbrain) gives rise to the medulla
- These together bound the fourth ventricle
- The choroid plexus differentiates from tela choroidea via active pia proliferation and invagination
- The three apertures form by rupture of evaginations in the ependymal roof - failure of these to open causes non-communicating hydrocephalus
- The Developing Human: Clinically Oriented Embryology
11. Clinical Significance
A. Hydrocephalus
Obstruction at the level of the fourth ventricle (or its foramina) produces obstructive (non-communicating) hydrocephalus. Common causes include tumors and congenital malformations.
B. Tumors of the Fourth Ventricle
| Tumor | Key Features |
|---|---|
| Medulloblastoma | Most common posterior fossa tumor in children; arises from undifferentiated neuroectodermal cells of the roof of the fourth ventricle (superior/inferior medullary velum, vermis); 25% of all pediatric brain tumors; typically hyperdense midline mass on CT; a cleft of CSF beneath the tumor in the ventricular canal helps distinguish it |
| Ependymoma | Arises from ependymal lining of the fourth ventricle floor/walls; tends to extend out through the foramina of Luschka ("plastic" ependymoma); second most common posterior fossa tumor in children |
| Hemangioblastoma | Cystic cerebellar tumor with mural nodule; associated with Von Hippel-Lindau syndrome |
| Choroid plexus papilloma | Rare; presents with overproduction hydrocephalus |
- Adams and Victor's Principles of Neurology, 12th Edition; Bradley and Daroff's Neurology in Clinical Practice
C. Dandy-Walker Malformation
A posterior fossa malformation spectrum defined by:
- Cystic dilatation of the fourth ventricle opening into a large posterior fossa cyst
- Aplasia or hypoplasia of the cerebellar vermis with vermian rotation
- Enlarged posterior fossa with elevated torcula (venous confluence elevated above the lambdoid suture - visible on plain X-ray, CT, and MRI)
- Associated with hydrocephalus and other midline CNS anomalies
- Spectrum ranges from classic Dandy-Walker to the benign mega cisterna magna (incidental finding)
- Grainger & Allison's Diagnostic Radiology
D. MS Plaques
Demyelinating plaques can occur in the floor of the fourth ventricle, causing cranial nerve deficits (e.g., internuclear ophthalmoplegia from MLF involvement along the floor).
- Neuroanatomy through Clinical Cases, 3rd Edition
E. Auditory Brainstem Implant
The cochlear nucleus is located in the floor of the lateral recess of the fourth ventricle, entered through the foramen of Luschka. This is the surgical access point for placing auditory brainstem implants (ABI) in patients who are not candidates for cochlear implants.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Summary Table
| Feature | Detail |
|---|---|
| Location | Posterior cranial fossa; within pons, medulla, and cerebellum |
| Inflow | Cerebral aqueduct of Sylvius (from 3rd ventricle) |
| Outflow | Foramen of Magendie (1, midline) + Foramina of Luschka (2, lateral) |
| Floor formed by | Pons (rostral) and medulla (caudal) - rhomboid fossa |
| Roof formed by | Cerebellum, superior + inferior medullary velum, tela choroidea |
| Choroid plexus supply | PICA, AICA, SCA |
| Caudal end | Obex (entry to spinal cord central canal) |
| Key clinical tumors | Medulloblastoma, ependymoma, hemangioblastoma |
| Key malformation | Dandy-Walker spectrum |
This is a shared conversation. Sign in to Orris to start your own chat.