GI SYSTEM ANATOMY
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
GI System Anatomy - Comprehensive Overview
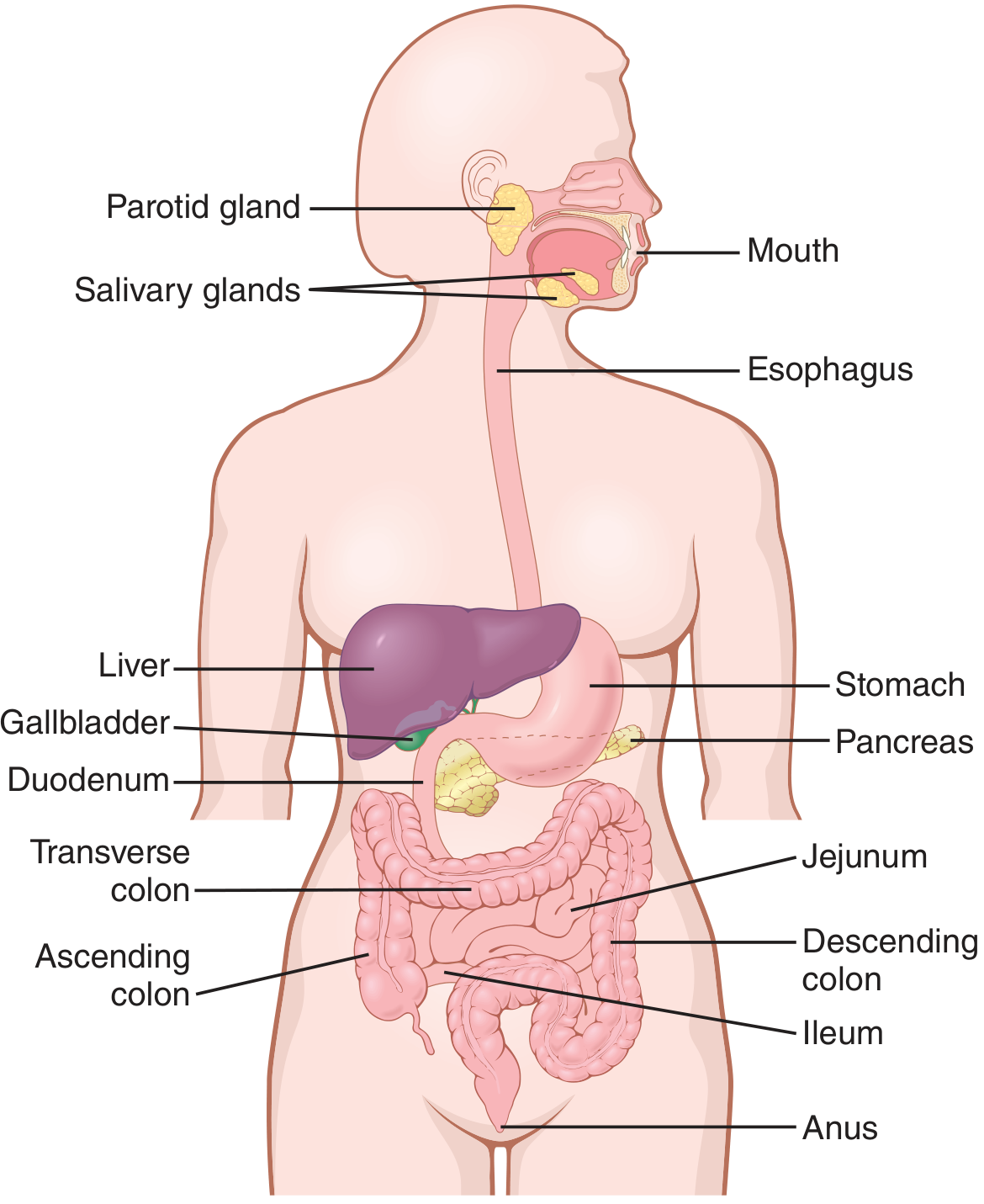
1. GENERAL ORGANIZATION
The GI tract (alimentary canal) extends from mouth to anus and is approximately 5-7 meters in the living adult. It is divided into:
- Upper GI tract: mouth, pharynx, esophagus, stomach, duodenum (to ligament of Treitz)
- Lower GI tract: jejunum, ileum, cecum, colon, rectum, anal canal
Accessory organs - liver, gallbladder, pancreas, salivary glands - contribute secretions essential for digestion.
2. LAYERS OF THE GI WALL
The basic wall structure is uniform throughout the gut (with regional modifications). From outer to inner:
| Layer | Composition | Key Features |
|---|---|---|
| Serosa | Mesothelial cells + loose CT | Covers intraperitoneal organs completely; only the anterior surface of retroperitoneal segments |
| Longitudinal muscle | Outer smooth muscle | Bundles run parallel to long axis; forms taeniae coli in colon |
| Circular muscle | Inner smooth muscle | Thickened locally at sphincters |
| Myenteric plexus | Auerbach's plexus | Between the two muscle layers; controls motility |
| Submucosa | Dense irregular CT | Meissner's plexus, blood vessels, lymphatics, Brunner's glands (duodenum) |
| Muscularis mucosae | Thin smooth muscle | Separates mucosa from submucosa |
| Lamina propria | Loose CT | Lymphocytes, plasma cells, capillaries, lacteals |
| Epithelium | Varies by region | Stratified squamous (esophagus) → columnar (intestines) |
Smooth muscle syncytium: Individual fibers are 200-500 µm long, 2-10 µm diameter, connected by gap junctions allowing electrical continuity. Each muscle layer functions as a syncytium - an action potential propagates throughout the mass. - Guyton and Hall Textbook of Medical Physiology, p. 776
Enteric Nervous System:
- Myenteric (Auerbach's) plexus: Between longitudinal and circular muscle layers - controls gut motility
- Submucosal (Meissner's) plexus: In the submucosa - controls secretion and mucosal blood flow
3. ESOPHAGUS
Embryology: Arises from the endodermally derived foregut. Tracheobronchial diverticulum separates at week 4. Upper esophageal striated muscle derived from branchial arches 4, 5, 6.
Gross anatomy:
- Begins at the pharyngoesophageal junction (level of thyroid cartilage C6) = Upper Esophageal Sphincter (UES)
- Passes posterior to the trachea and heart, through the diaphragmatic hiatus (at T10)
- Ends at the esophagogastric junction (EGJ), 1-2 cm below the diaphragmatic hiatus, left of T10 vertebral body
- Adult length: ~25 cm
- Three anatomic narrowings (sites of foreign body impaction and strictures):
- UES (cricopharyngeus) - ~15 cm from incisors
- Aortic arch / left mainstem bronchus - ~23 cm
- Lower esophageal sphincter (LES) / diaphragmatic hiatus - ~40 cm
Histology:
- Lined by non-keratinized stratified squamous epithelium
- No serosal layer (clinically important - anastomotic leaks spread freely to the mediastinum)
- Upper 1/3: striated muscle; middle 1/3: mixed; lower 1/3: smooth muscle
LES: Physiologically identified as a 3-4 cm zone of elevated resting pressure. Not an anatomic sphincter but a functional one. Prevents gastroesophageal reflux.
- Yamada's Textbook of Gastroenterology, p. 120
4. STOMACH
Embryology: Recognizable at week 4 as a dilation of the distal foregut. Rotates 90° around its longitudinal axis during development - the dorsal aspect (greater curvature) moves left, ventral aspect (lesser curvature) moves right. This explains why the left vagus innervates the anterior wall and the right vagus innervates the posterior wall.
Gross anatomy:
- J-shaped dilation; volume ~30 mL (neonate) to 1.5-2 L (adult)
- EGJ lies left of T10, 1-2 cm below diaphragmatic hiatus
- Gastroduodenal junction (pylorus) lies at L1, right of midline
Four anatomic regions:
| Region | Location | Key Cell Types |
|---|---|---|
| Cardia | Just distal to EGJ; ill-defined | Mucous cells |
| Fundus | Dome above EGJ; contacts left hemidiaphragm | Oxyntic (parietal + chief) cells |
| Body (Corpus) | Largest region | Parietal cells (HCl, IF), Chief cells (pepsinogen) |
| Antrum/Pylorus | Distal 20-25%; ends at pyloric sphincter | G cells (gastrin), D cells (somatostatin) |
Peritoneal relationships:
- Lesser omentum (gastrohepatic ligament) from lesser curvature to liver
- Greater omentum hangs from fundus/greater curvature: to transverse colon (gastrocolic ligament), spleen (gastrosplenic ligament), diaphragm (gastrophrenic ligament)
- Posterior stomach = anterior wall of omental bursa (lesser sac)
- Posterior relations: pancreas, transverse colon, diaphragm, spleen, left kidney, left adrenal
Histology (oxyntic glands - fundus/body):
- Parietal cells (oxyntic cells): Large, eosinophilic, with extensive intracellular canalicular system; secrete HCl and intrinsic factor
- Chief cells (zymogen cells): Basophilic (rich in RER); secrete pepsinogen I & II
- ECL cells (argyrophilic/enterochromaffin-like): In oxyntic glands; contain histamine - stimulate parietal cells via H2 receptors
- D cells (closed endocrine cells): Secrete somatostatin via long processes (paracrine)
Antral glands:
-
G cells (open endocrine cells): Secrete gastrin; stimulated by gastric distension, vagal stimulation, amino acids
-
Mucous cells predominate
-
Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 830-834
5. SMALL INTESTINE
Overview: Spans pylorus to ileocecal valve; 5-7 m in adults; represents >60% of alimentary tract length. Three divisions:
| Segment | Length | Key Features |
|---|---|---|
| Duodenum | 25-30 cm (C-shaped) | Mostly retroperitoneal; 4 parts; ampulla of Vater in D2 |
| Jejunum | Proximal 2/5 distal to ligament of Treitz | Wider lumen, more prominent plicae circulares, long vasa recta |
| Ileum | Distal 3/5 | Shorter vasa recta with more arborization, Peyer's patches, terminal ileum absorbs B12 & bile salts |
No clear anatomic boundary between jejunum and ileum; the ligament of Treitz (suspensory muscle of duodenum) marks the duodenojejunal flexure.
Embryology: Midgut undergoes 270° counterclockwise rotation - 90° at 8 weeks (during herniation), then additional 180° on return at ~10 weeks. Failure = malrotation.
Wall layers:
- Mucosa: Epithelium + lamina propria + muscularis mucosae
- Villi: Finger-like projections; each contains a central lacteal (lymphatic), capillary plexus, and central arteriole/venule
- Crypts of Lieberkühn: Base of villi; contain stem cells, Paneth cells, goblet cells
- Microvilli (brush border): Increase surface area ~30x; coated by glycocalyx
- Plicae circulares (valvulae conniventes): Circular folds from D2 onward - increase surface area 3x
- Submucosa: Contains Brunner's glands (duodenum only) - secrete alkaline mucus
- Muscle layers: Outer longitudinal + inner circular; myenteric plexus between them
- Serosa: Covers mobile (mesenteric) small bowel completely
Surface area amplification: Plicae circulares (×3), villi (×10), microvilli (×30) = total surface area of ~250 m²
Vascular supply:
-
Superior Mesenteric Artery (SMA) supplies the entire small intestine
-
Vasa recta are the terminal intestinal arterial branches (no anastomosis within the wall - clinically vulnerable to ischemia)
-
Jejunum: Long, straight vasa recta; fewer arterial arcades
-
Ileum: Short vasa recta with greater arborization; more arcades (→ better collateral, less at risk per unit)
-
Venous drainage via Superior Mesenteric Vein (SMV) → portal vein
-
Mulholland and Greenfield's Surgery, p. 2362-2370
6. LARGE INTESTINE
Total length: ~150 cm. Distinguishing features vs. small bowel:
| Feature | Large Intestine | Small Intestine |
|---|---|---|
| Taeniae coli | 3 longitudinal bands of outer muscle | Continuous outer muscle layer |
| Haustra | Sacculations between taeniae | Absent |
| Epiploic appendices | Fat-filled peritoneal tags | Absent |
| Villi | Absent | Present |
| Diameter | Larger | Smaller |
Cecum
- Saccular beginning; diameter ~7.5 cm, length ~10 cm
- Intraperitoneal, no mesentery; thin wall (highest risk of perforation in obstruction)
- Ileocecal valve: Thickened, nipple-shaped invagination of circular muscle; terminal ileum enters medial border
- Cecal dilation >12 cm on plain film = risk of ischemic necrosis/perforation
Appendix
- Arises ~3 cm below ileocecal valve; 8-10 cm long, blind-ending tube
- Positions: retrocecal (65%) > pelvic (31%) > subcecal (2.3%) > preileal (1%) > retroileal (0.4%)
- Located by following the anterior taenia coli to its convergence at the appendix base
Ascending Colon
- From ileocecal junction to hepatic flexure; ~15 cm long
- Posterior surface retroperitoneal (fixed by fascia of Toldt)
- Mobilized by incising the white line of Toldt; beware of proximity to 2nd part of duodenum
Transverse Colon
- Hepatic to splenic flexure; ~45 cm; completely intraperitoneal
- Suspended by transverse mesocolon; greater omentum attached superiorly
Descending Colon
- Splenic flexure to sigmoid; retroperitoneal; ~25 cm
Sigmoid Colon
- Redundant, mobile loop; most common site of diverticular disease
- Transitions to rectum at rectosigmoid junction (~15 cm from anal verge)
Rectum
-
15-20 cm long; begins at rectosigmoid junction, ends at anus
-
Divided into thirds by peritoneal reflections:
- Upper 1/3: Covered by peritoneum anteriorly and laterally (>10 cm above dentate line)
- Middle 1/3: Peritoneum anteriorly only (5-10 cm above dentate line)
- Lower 1/3: Completely extraperitoneal (1-5 cm above dentate line)
-
Three valves of Houston: Lateral folds - proximal and distal fold right, middle folds left
-
No taeniae coli, no haustra, no epiploic appendices
-
Mesorectum: Visceral mesentery of rectum; contains lymphovascular supply - key in Total Mesorectal Excision (TME)
-
Anterior relations: rectovesicular pouch (male), pouch of Douglas (female) - lowest point of peritoneal cavity; site of "drop metastases" - Blumer shelf
-
Sabiston Textbook of Surgery, p. 2058-2063
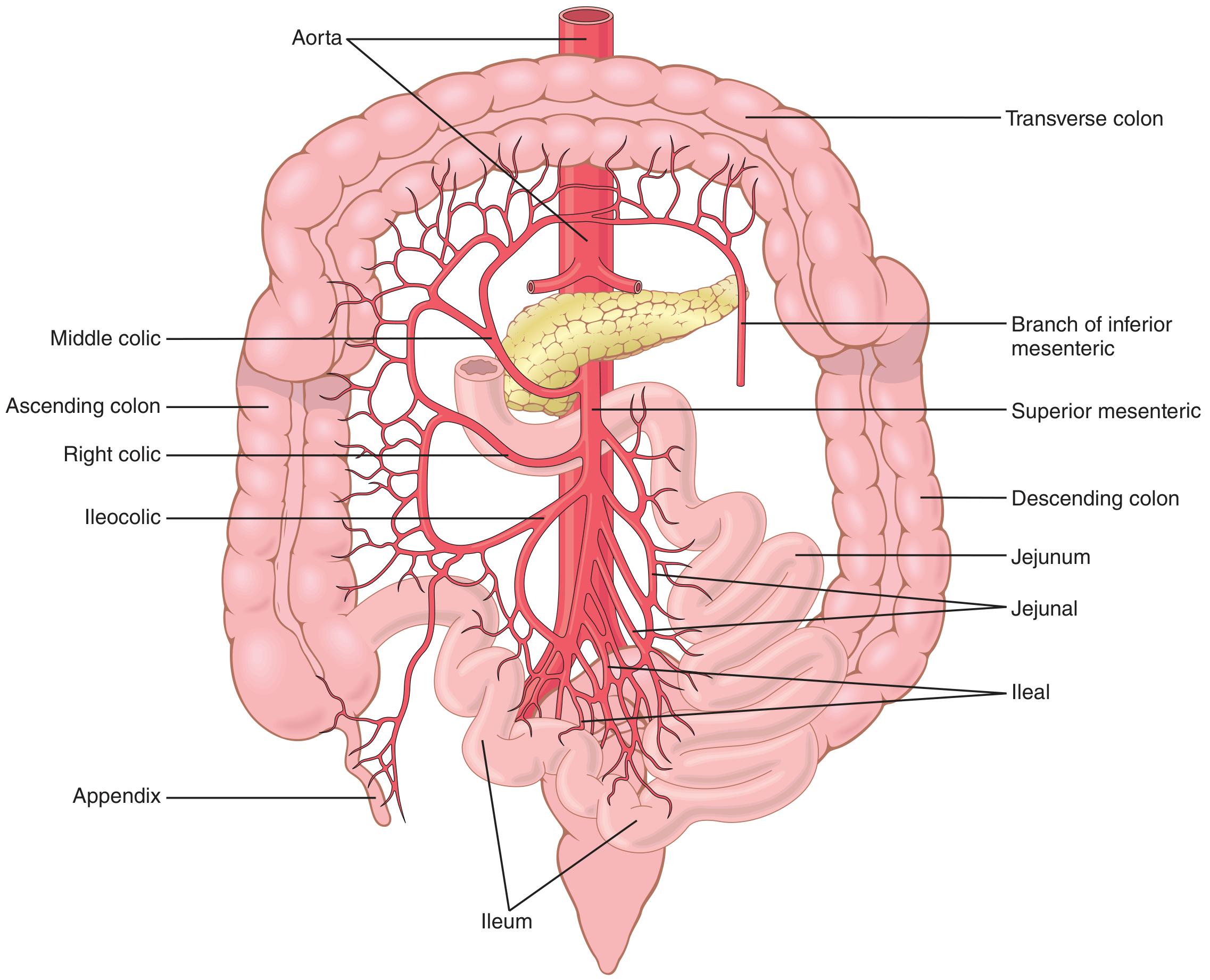
7. BLOOD SUPPLY - OVERVIEW
Arterial supply (three celiac axis territories):
| Region | Artery | Origin |
|---|---|---|
| Esophagus (lower) | Branches of left gastric + inferior phrenic | Celiac axis |
| Stomach | Left/right gastric, left/right gastroepiploic, short gastric | Celiac axis |
| Duodenum | Gastroduodenal → superior pancreaticoduodenal; inferior pancreaticoduodenal (from SMA) | Celiac + SMA watershed |
| Small intestine | SMA (jejunal + ileal branches) | SMA |
| Right colon (cecum, ascending, proximal transverse) | Ileocolic, right colic, middle colic arteries | SMA |
| Left colon (distal transverse, descending, sigmoid) | Left colic, sigmoid arteries | IMA |
| Rectum | Superior rectal (from IMA), middle rectal (from internal iliac), inferior rectal (from internal pudendal) | IMA + internal iliac |
Watershed zones (clinically vulnerable to ischemia):
- Griffiths' point: Splenic flexure (junction SMA/IMA territories)
- Sudeck's point: Rectosigmoid junction (superior rectal artery terminal branches)
Venous drainage:
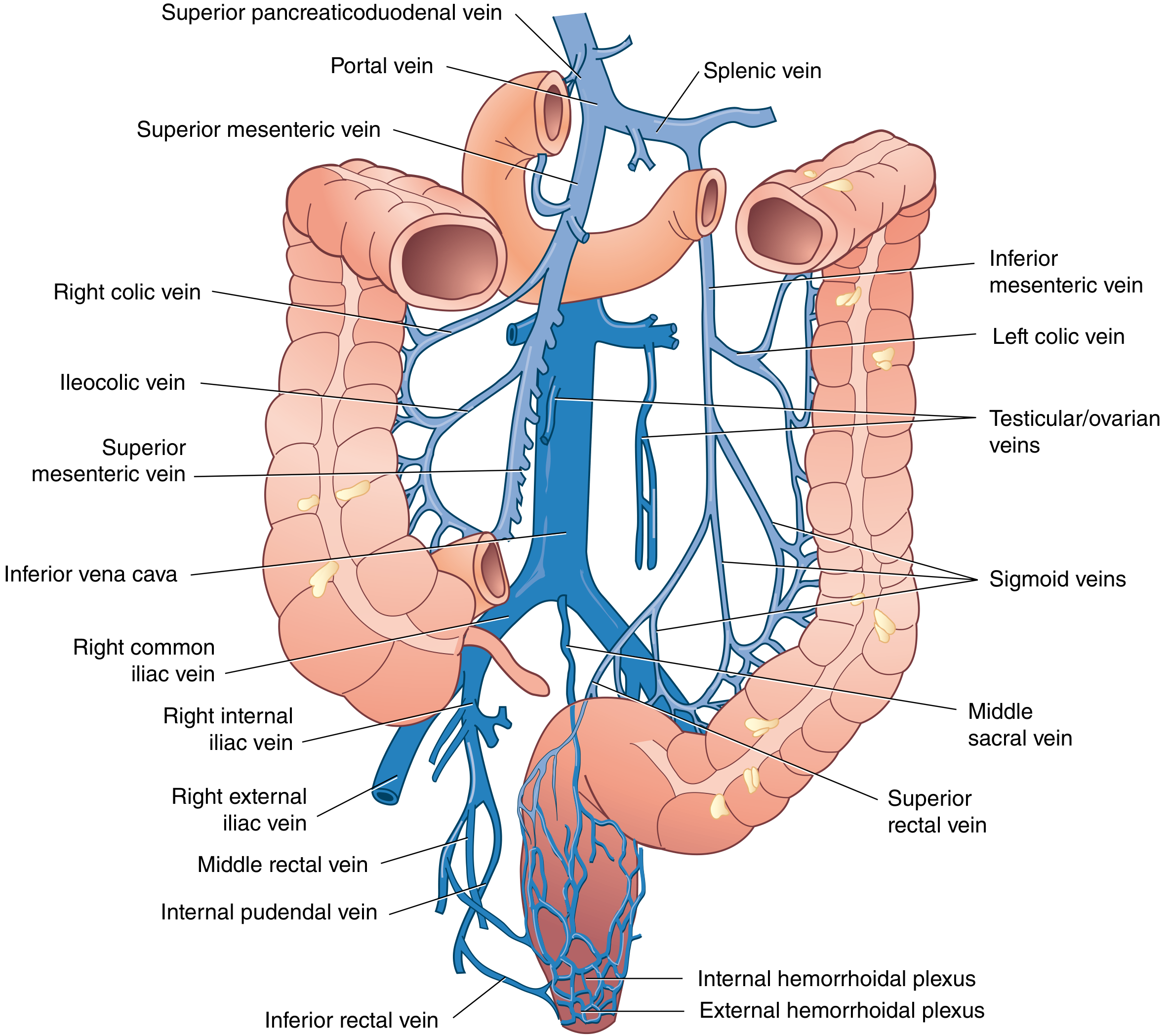
- SMV + splenic vein = portal vein (behind neck of pancreas)
- IMV drains into splenic vein
- Portal-systemic anastomoses (clinically important in portal hypertension):
- Esophageal veins (left gastric ↔ azygos) → esophageal varices
- Rectal veins (superior rectal/IMV ↔ middle & inferior rectal/systemic) → hemorrhoids
- Paraumbilical veins → caput medusae
- Retroperitoneal veins of Retzius
8. LYMPHATIC DRAINAGE
- Small intestine: Lacteals → mesenteric lymph nodes → superior mesenteric nodes → cisterna chyli → thoracic duct
- Stomach: Along gastric arteries to celiac lymph nodes
- Colon: Epicolic → paracolic → intermediate (along named vessels) → principal (at SMA/IMA origin)
- Rectum: Upper rectum → inferior mesenteric nodes; lower rectum → internal iliac nodes; anal canal below dentate line → inguinal nodes
- Fat-soluble nutrients absorbed as chylomicrons bypass the portal system and enter via thoracic duct directly into systemic circulation
9. INNERVATION
Extrinsic (autonomic)
| Division | Fibers | Effect |
|---|---|---|
| Parasympathetic (vagus - CN X) | To transverse colon; pelvic splanchnics (S2-S4) to left colon/rectum | ↑ motility, ↑ secretion |
| Sympathetic (T5-L2) | Via splanchnic nerves to celiac, SMA, IMA ganglia | ↓ motility, vasoconstriction |
Intrinsic (Enteric Nervous System)
- Myenteric (Auerbach's) plexus: Between longitudinal and circular muscle - controls peristalsis
- Submucosal (Meissner's) plexus: In submucosa - controls secretion/absorption and mucosal blood flow
- ENS contains ~500 million neurons (more than the spinal cord) and functions semi-independently
10. PERITONEAL RELATIONSHIPS SUMMARY
| Organ | Peritoneal Status | Clinical Note |
|---|---|---|
| Stomach | Intraperitoneal | Mobile |
| Duodenum (D2-D4) | Retroperitoneal | Fixed behind peritoneum |
| Jejunum/Ileum | Intraperitoneal | Mobile on mesentery |
| Cecum | Intraperitoneal | No mesentery |
| Ascending colon | Retroperitoneal | Fixed - mobilize via line of Toldt |
| Transverse colon | Intraperitoneal | Suspended by mesocolon |
| Descending colon | Retroperitoneal | Fixed |
| Sigmoid colon | Intraperitoneal | Mobile, redundant |
| Rectum (upper) | Intraperitoneal (anterior + lateral) | |
| Rectum (lower) | Extraperitoneal | Completely below peritoneum |
| Liver | Intraperitoneal (except bare area) | Bare area contacts diaphragm |
| Gallbladder | Intraperitoneal (fundus/body) | Liver bed = bare |
| Pancreas | Retroperitoneal | Fixed |
11. ACCESSORY ORGANS (Overview)
Liver
- Largest organ; ~1500 g; lies in RUQ under right hemidiaphragm
- Couinaud segments (I-VIII) based on portal and hepatic vein distribution - each is a functionally independent unit with its own portal triad and hepatic vein branch
- Falciform ligament divides anatomic left and right lobes; contains ligamentum teres (obliterated umbilical vein)
- Functional division: Right and left lobes divided by Cantlie's line (Rex-Cantlie line) = from gallbladder fossa to IVC - this corresponds to the right and left branches of the portal vein
- Porta hepatis: Entry of portal vein, hepatic artery, exit of bile duct - all within hepatoduodenal ligament (right free edge of lesser omentum)
- Blood supply: Dual - portal vein (~75%) + hepatic artery (~25%)
Gallbladder & Biliary Tree
- Gallbladder: Pear-shaped, 7-10 cm long; capacity ~50 mL; sits in a fossa on the visceral surface of the liver (segment IV/V junction)
- Triangle of Calot (hepatocystic triangle): Bounded by cystic duct (lateral), common hepatic duct (medial), and liver edge (superior) - contains the cystic artery (typically from right hepatic artery) - must be identified in cholecystectomy
- Bile duct anatomy: Right and left hepatic ducts → common hepatic duct → (joined by cystic duct) → common bile duct (CBD) → passes posterior to duodenum → joins pancreatic duct → enters duodenum at ampulla of Vater (papilla of Vater, in D2) - guarded by the sphincter of Oddi
Pancreas
- Retroperitoneal organ; 12-20 cm long; lies at the level of L1-L2
- Parts: head (nestled in C-loop of duodenum), uncinate process (posterior to SMA/SMV), neck (anterior to portal/SMV confluence), body, tail (reaches splenic hilum)
- Main duct (Wirsung): Runs length of gland, joins CBD at ampulla of Vater
- Accessory duct (Santorini): Drains upper head, opens at minor papilla (~2 cm proximal to major papilla)
- Annular pancreas: Failure of ventral pancreatic bud rotation → ring around duodenum → duodenal obstruction
- Blood supply: Pancreaticoduodenal arteries (from gastroduodenal and SMA) for the head; splenic artery branches for body and tail
Quick Revision Table - Key Measurements
| Structure | Key Measurement |
|---|---|
| Esophagus length | ~25 cm |
| Esophagus from incisors: UES | ~15 cm |
| Esophagus from incisors: aortic arch | ~23 cm |
| Esophagus from incisors: LES | ~40 cm |
| Stomach volume (adult) | 1.5-2 L |
| Duodenum length | 25-30 cm |
| Small intestine total length | 5-7 m |
| Large intestine total length | ~150 cm |
| Appendix length | 8-10 cm |
| Appendix position (most common) | Retrocecal (65%) |
| Rectum length | 15-20 cm |
| Cecum diameter (perforation risk if obstructed) | >12 cm |
| Rectovesicular pouch (male) | 7-9 cm from anal verge |
| Pouch of Douglas (female) | 5-7.5 cm from anal verge |
| Gallbladder capacity | ~50 mL |
| Pancreas: vertebral level | L1-L2 |
Sources: Guyton and Hall Textbook of Medical Physiology | Sleisenger and Fordtran's Gastrointestinal and Liver Disease | Sabiston Textbook of Surgery | Mulholland and Greenfield's Surgery | Yamada's Textbook of Gastroenterology
This is a shared conversation. Sign in to Orris to start your own chat.