Pterygopalatine fossa anatomy in detail and optic nerve decompression in detail according to standard ENT textbook
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
I now have comprehensive information from multiple standard ENT textbooks. Let me compile the detailed response.
Pterygopalatine Fossa (PTF) - Detailed Anatomy
Shape and Location
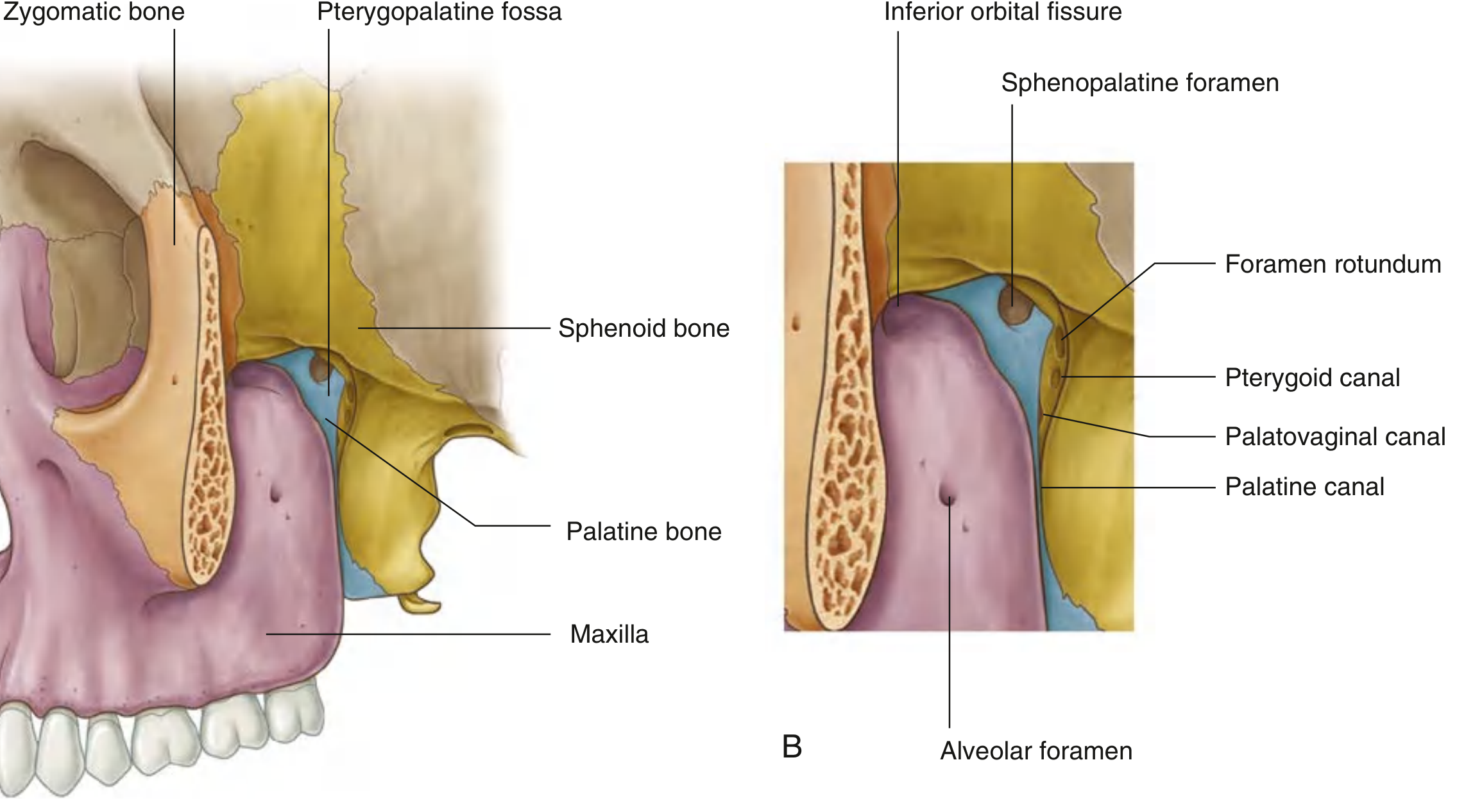
The pterygopalatine fossa is an inverted teardrop-shaped (or inverted cone-shaped) space on the lateral skull, immediately posterior to the maxilla and near the orbital apex. Despite its small size, it is one of the most important junctional spaces in the skull base because it communicates with six major regions and serves as the primary distribution hub for the maxillary nerve (V2) and the terminal maxillary artery.
(Gray's Anatomy for Students; K.J. Lee's Essential Otolaryngology)
Boundaries
| Wall | Structure |
|---|---|
| Superior (roof/base) | Body of sphenoid bone + orbital process of palatine bone |
| Inferior (apex) | Greater palatine canal (inverted cone narrows here) |
| Anterior | Posterior wall of the maxillary antrum (sinus) |
| Posterior | Pterygoid process and greater wing of sphenoid |
| Medial | Perpendicular plate of the palatine bone / lateral nasal wall; sphenopalatine foramen opens here |
| Lateral | Open (deficient) - communicates with the infratemporal fossa inferiorly via the pterygomaxillary fissure, and with the orbit superiorly via the inferior orbital fissure |
(K.J. Lee's Essential Otolaryngology, p. 632; Scott-Brown's Vol.2, p. 1249)
Foramina and Communications
The fossa is strategically connected to six regions through the following openings:
| Foramen/Fissure | Location | Communication | Structures Transmitted |
|---|---|---|---|
| Foramen rotundum | Posterior wall | Middle cranial fossa | V2 (maxillary nerve) |
| Pterygoid (Vidian) canal | Posterior wall (medial) | Foramen lacerum / Middle cranial fossa | Vidian nerve (union of greater & deep petrosal nerves) |
| Palatovaginal canal | Posterior wall (most medial) | Nasopharynx | Posterior nasal nerve, pharyngeal branch |
| Sphenopalatine foramen | Medial wall | Lateral nasal cavity | Sphenopalatine artery and nerve |
| Inferior orbital fissure | Superior/lateral | Orbit (orbital floor) | V2 (as infraorbital nerve), infraorbital artery |
| Pterygomaxillary fissure | Lateral | Infratemporal fossa | Internal maxillary artery enters PTF here |
| Greater palatine canal | Inferior | Hard palate and oral cavity | Greater and lesser palatine nerves and vessels |
| Lesser palatine canal | Inferior | Soft palate | Lesser palatine nerves |
| Alveolar foramen | Inferior/anterior | Upper teeth | Posterior superior alveolar nerves |
Key spatial relationships: Vascular structures lie anterior to neural structures and are therefore encountered first during surgical access. The foramen rotundum (V2) is posterolateral, Vidian canal is more medial, and the palatovaginal canal is the most medial of the posterior foramina.
(K.J. Lee's Essential Otolaryngology; Gray's Anatomy for Students; Cummings Otolaryngology)
Contents of the PTF
1. Maxillary Nerve (V2)
- Enters the PTF through foramen rotundum from the middle cranial fossa
- Exits superiorly through the inferior orbital fissure as the infraorbital nerve
- Branches within the fossa:
- Posterior superior alveolar nerve (to upper molar teeth)
- Zygomatic nerve (exits via inferior orbital fissure)
- Ganglionic branches (2 short roots connecting V2 to the pterygopalatine ganglion - carry sensory fibers through the ganglion without synapsing)
2. Pterygopalatine Ganglion (Sphenopalatine Ganglion)
- The largest parasympathetic ganglion in the head
- Lies in the PTF just anterior to the pterygoid canal opening
- Parasympathetic (secretomotor) root: Preganglionic fibers travel via the greater petrosal nerve (from CN VII, geniculate ganglion) → joins deep petrosal nerve (sympathetic, from ICA plexus) → forms Vidian nerve (nerve of the pterygoid canal) → enters ganglion and synapses → postganglionic fibers hitchhike on V2 branches to supply:
- Lacrimal gland (via zygomatic nerve → lacrimal nerve)
- Nasal and palatine glands
- Sympathetic root: Deep petrosal nerve (no synapse - passes through)
- Sensory root: Ganglionic branches from V2 (no synapse - passes through)
- Branches distributed: nasopalatine nerve, greater palatine nerve, lesser palatine nerves, posterior superior nasal nerves, pharyngeal branch
3. Internal (3rd part of the) Maxillary Artery
- The terminal portion of the maxillary artery enters the PTF via the pterygomaxillary fissure
- Branches:
- Sphenopalatine artery (exits through sphenopalatine foramen → supplies lateral nasal wall and septum; the terminal branch is the dominant blood supply to the nose)
- Descending palatine artery (descends through greater palatine canal → divides into greater and lesser palatine arteries)
- Infraorbital artery (exits via inferior orbital fissure → infraorbital canal)
- Posterior superior alveolar artery (to upper molars/premolars)
- Artery of pterygoid canal (Vidian artery)
- Pharyngeal artery
4. Fat (Adipose tissue filling)
Clinical Significance of the PTF
-
Spread of disease: Malignant sinonasal tumors use the PTF as a highway - tumors can spread from the maxillary sinus posteriorly into the PTF, then via foramen rotundum to the middle cranial fossa (perineural spread along V2), or laterally into the infratemporal fossa. PTF involvement upgrades most sinonasal tumors to T4.
-
Sphenopalatine artery ligation: The primary surgical approach for intractable posterior epistaxis involves endoscopic ligation of the sphenopalatine artery at the sphenopalatine foramen as it exits the PTF.
-
Pterygopalatine ganglion block: Used for cluster headaches, trigeminal neuralgia, and as a regional anesthetic technique.
-
Vidian neurectomy: Transection of the Vidian nerve was historically performed for vasomotor rhinitis.
-
Surgical corridor: The PTF is an important corridor for approaches to the skull base, infratemporal fossa, and nasopharynx.
(Cummings Otolaryngology Head and Neck Surgery, p. 1759; Scott-Brown's Vol. 2, p. 1249)
Endoscopic Optic Nerve Decompression
Overview
Surgical decompression of the optic nerve addresses visual loss secondary to traumatic or compressive optic neuropathy. The intracanalicular segment of the optic nerve is uniquely susceptible because it lies within the fixed bony confines of the optic canal - it cannot expand when swelling occurs, creating a compartment-syndrome effect. The endoscopic endonasal approach is considered superior for most cases because it offers: no external scars, preserved olfaction, quicker recovery, and excellent intraoperative visualization.
(Cummings Otolaryngology, p. 975; Scott-Brown's Vol. 1, p. 1297)
Relevant Anatomy
- The optic canal is formed by two struts of the lesser wing of the sphenoid, containing:
- The optic nerve
- The ophthalmic artery (generally courses superolateral to the optic nerve, but takes an inferior/inferomedial course in approximately 20% of orbits - critical surgical consideration)
- Endonasally, the intracanalicular optic nerve appears as a prominence along the superolateral aspect of the sphenoid sinus
- When a sphenoethmoid cell (Onodi cell) is present, the optic nerve prominence will be within this posterior ethmoid air cell rather than the sphenoid sinus
- The intra-canalicular segment retains all three meningeal layers including the subarachnoid space with CSF; these layers condense at the orbital apex to form the annulus of Zinn
- The opticocarotid recess lies between the optic canal and the carotid canal and is a key surgical landmark
(Cummings Otolaryngology, p. 975)
Indications
- Traumatic optic neuropathy (TON) - Most common indication
- Occurs in 1.5-4% of all head trauma patients
- Mechanism: indirect force transmission → edema of optic nerve within the fixed bony canal → compartment syndrome → apoptosis of retinal ganglion cells
- Compressive optic neuropathy:
- Fibro-osseous lesions of the sphenoid
- Meningiomas of the skull base (hyperostotic reaction compresses canal)
- Benign sinonasal tumors, sinonasal malignancies
- Inflammatory: orbital pseudotumor, Graves' orbitopathy/thyroid eye disease
- Orbital tumors at the apex
(Cummings Otolaryngology, p. 975; Scott-Brown's Vol. 1, p. 1297)
Controversies in TON Management
Significant controversy surrounds indirect TON management. Three options exist:
- Expectant management - some spontaneous recovery
- Corticosteroid therapy - one meta-analysis showed improved outcomes; the subsequent International Optic Nerve Trauma Study (IONTS) failed to show a difference vs. other treatments; high-dose steroids carry increased mortality risk in acute head trauma
- Surgical decompression
The IONTS remains the landmark study and treatment should be individualized to the patient and clinical scenario.
Nerve sheath incision debate: Optic nerve sheath fenestration after bony decompression has a theoretic advantage (more maximal decompression, drainage of intra-sheath hematoma), but has NOT been shown superior to bony decompression alone. Risks include injury to optic nerve or ophthalmic artery and increased CSF leak risk. However, for compressive optic neuropathy from intra-sheath tumors, sheath opening is required for tumor removal.
(Cummings Otolaryngology, p. 975)
Pre-Operative Evaluation
- Complete ophthalmologic examination:
- Visual acuity
- Color vision (dyschromatopsia - alteration in color vision, an early sensitive sign)
- Relative afferent pupillary defect (RAPD)
- Visual field testing
- CT sinuses (fine cut, without contrast): assess for optic canal fracture, bone displacement, sinus anatomy for endoscopic planning
- MRI orbits with and without contrast: evaluate the entire course of the optic nerve, orbital contents, and relationship of lesion to the optic nerve
- In unresponsive patients: visual evoked potentials (though often impractical)
- Patients with compressive lesions: CT angiography if vascular lesion suspected
(Cummings Otolaryngology, p. 975; Scott-Brown's Vol. 1, p. 1297)
Surgical Technique - Endoscopic Endonasal Approach
Surgery for TON should ideally be performed within 72 hours of injury.
Step-by-Step Procedure
Step 1 - Complete Ethmoidectomy
- Perform a full anterior and posterior ethmoidectomy
- Expose the ethmoid roof (skull base) superiorly and lamina papyracea laterally
- Remove all bony partitions off the lamina papyracea
Step 2 - Wide Sphenoidotomy
- Open the sphenoid sinus maximally, especially laterally toward the orbital apex
- Extend to the planum sphenoidale superiorly
- Identify: optic nerve prominence, carotid canal, and the opticocarotid recess (OCR) between them
- If an Onodi cell is present: remove the partition between the Onodi cell and the sphenoid sinus to fully expose the optic nerve
Step 3 - Lamina Papyracea Removal (Orbital Decompression Component)
- Fracture the lamina papyracea in the posterior ethmoid region using an "eggshell fracture" technique
- Remove approximately 1 to 1.5 cm of lamina anterior to the face of the sphenoid
- Extreme care must be taken not to penetrate the periorbita - if orbital fat herniates into the field, it will preclude safe optic nerve decompression
Step 4 - Identification of Landmarks
- At the orbital apex, the periorbita condenses to form the annulus of Zinn and the dense bone of the optic strut is encountered
- Image-guided surgery (navigation) is ideally employed at this stage
Step 5 - Drilling the Optic Canal (Bone Removal)
- Use a high-speed drill with a coarse diamond burr (not cutting burr)
- Copious irrigation throughout to prevent thermal injury to the optic nerve
- Begin drilling laterally and work medially along the optic strut
- Drill along the nerve, not across it to avoid shearing injury
- Thin the bone until it can be lifted in an inferomedial direction
- Use a blunt elevator to lift thinned bone fragments away from the nerve, then remove them
- Extent of decompression: 1 cm posterior to the face of the sphenoid sinus for TON and thyroid eye disease
Step 6 - Nerve Sheath Incision (if indicated)
- Performed after bony decompression is complete
- Use a disposable sickle knife along the entire length of the exposed nerve
- Direction: posterior to anterior, incorporating the annulus of Zinn
- Watch for the ophthalmic artery (may lie inferior or inferomedial in 20% of cases)
- Egress of CSF will be seen after incision
Step 7 - Reconstruction
- If nerve sheath has been incised: apply a mucosal onlay graft to prevent postoperative rhinorrhoea
(Cummings Otolaryngology, p. 975; Scott-Brown's Vol. 1, pp. 1297-1298)
Complications
- CSF leak (especially after nerve sheath incision)
- Direct injury to the optic nerve (rare but devastating)
- Injury to the ophthalmic artery - can cause visual loss; risk is higher when it takes an anomalous inferomedial course
- Risks of standard endoscopic sinus surgery: orbital entry, bleeding, anosmia
- Deterioration of vision post-operatively (uncommon)
Outcomes
- Approximately 40-60% of patients who undergo decompression for TON demonstrate improvement in visual acuity
- Patients with no light perception at initial evaluation have a poorer prognosis
- Outcomes for compressive optic neuropathy (non-traumatic) tend to be better than for TON
- Visual deterioration after surgery is uncommon
(Cummings Otolaryngology, p. 975-976)
Summary Comparison Table
| Feature | PTF Anatomy | Optic Nerve Decompression |
|---|---|---|
| Key book references | Gray's Anatomy for Students; K.J. Lee; Scott-Brown's Vol 2; Cummings | Cummings; Scott-Brown's Vol 1 |
| Critical structures | V2, pterygopalatine ganglion, maxillary artery, Vidian nerve | Optic nerve, ophthalmic artery, opticocarotid recess |
| Key surgical steps | Medial maxillectomy, sphenopalatine artery ligation, PTF fat exposure | Ethmoidectomy, sphenoidotomy, optic strut drilling |
| Key danger | Internal carotid artery in ITF extension; V2 injury | Ophthalmic artery anomalous course (20%); thermal nerve injury |
Sources:
- Gray's Anatomy for Students, p. 1132
- K.J. Lee's Essential Otolaryngology, pp. 632, 700
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 1249
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, pp. 1297-1298
- Cummings Otolaryngology Head and Neck Surgery, pp. 975-976, 1759
This is a shared conversation. Sign in to Orris to start your own chat.