what divides compartment of thigh
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete, textbook-sourced answer:
What Divides the Compartments of the Thigh?
The thigh is divided into three compartments by fascial partitions. The outer boundary for all three is the fascia lata (the deep investing fascia of the thigh), and the internal divisions are formed by intermuscular septa that extend inward from the fascia lata to attach to the linea aspera of the femur.
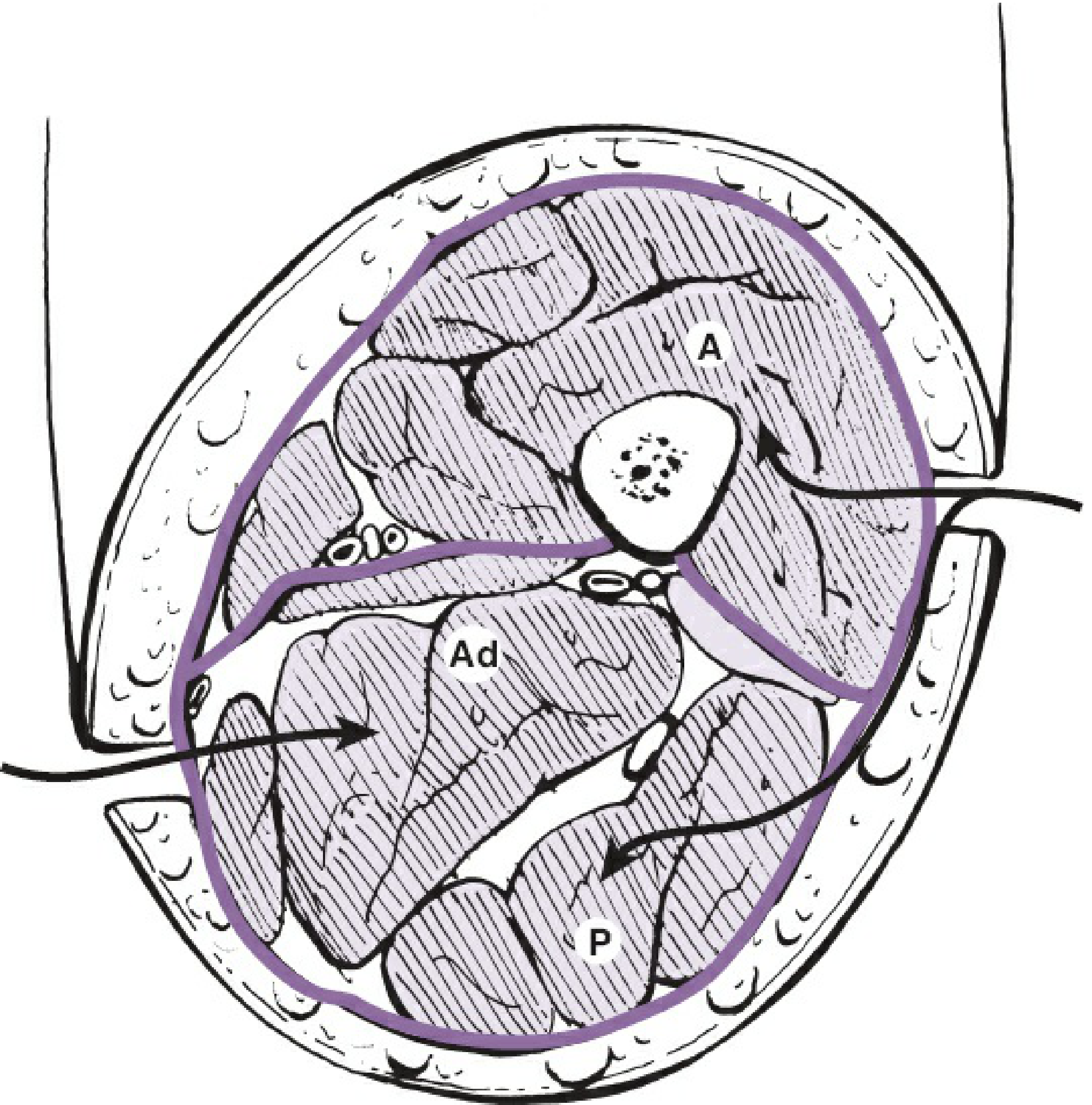
Cross-section of the thigh: A = anterior compartment, Ad = adductor (medial) compartment, P = posterior compartment.
The Dividing Structures
| Structure | What it separates |
|---|---|
| Fascia lata | Forms the outer boundary of all three compartments |
| Lateral intermuscular septum | Separates the anterior compartment from the posterior compartment (runs between vastus lateralis and the short head of biceps femoris) |
| Anteromedial (medial) intermuscular septum | Separates the anterior compartment from the adductor (medial) compartment (runs between vastus medialis and the adductor muscles) |
| Posteromedial intermuscular septum | Separates the adductor compartment from the posterior compartment (runs between adductor magnus and the hamstrings) |
Both the lateral and medial septa are attached to the linea aspera of the femur, using the bone itself as a rigid anchor point.
The Three Compartments and Their Contents
| Compartment | Main Muscles | Key Nerve | Key Vessel |
|---|---|---|---|
| Anterior | Quadriceps femoris (vastus lateralis, medialis, intermedius, rectus femoris), sartorius | Femoral nerve | Femoral artery/vein |
| Medial (Adductor) | Adductor longus, adductor brevis, adductor magnus, gracilis | Obturator nerve | Obturator vessels |
| Posterior | Biceps femoris, semimembranosus, semitendinosus (hamstrings) | Sciatic nerve | Perforating branches of profunda femoris |
Quick Summary
The key dividers are:
- Fascia lata - the outer sleeve
- Lateral intermuscular septum - between anterior and posterior
- Medial (anteromedial) intermuscular septum - between anterior and adductor
- Posteromedial intermuscular septum - between adductor and posterior
All septa attach to the linea aspera of the femur, which acts as the bony anchor for all three compartment walls.
- Rockwood and Green's Fractures in Adults, 10th ed., p. 684
- Fischer's Mastery of Surgery, 8th ed., p. 6658
explain about knee joint
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, well-structured explanation of the knee joint drawn from authoritative anatomy textbooks:
The Knee Joint
1. Basic Classification
The knee joint is the largest synovial joint in the body. It is classified as a modified hinge joint (ginglymus) that primarily allows flexion and extension, with a limited degree of rotation that increases as flexion increases.
It actually consists of two articulations within a single joint capsule:
- Tibiofemoral joint - the weight-bearing articulation between the femoral condyles and the tibial plateau
- Patellofemoral joint - between the patella and the anterior femoral surface, allowing the quadriceps to act efficiently without tendon wear
The shape of the joint surfaces makes it inherently unstable, so it depends heavily on ligaments, menisci, and muscles for stability.
2. Articular Surfaces
All surfaces are covered by hyaline cartilage. The key surfaces are:
- Two femoral condyles (medial and lateral) - the posterior curved surfaces articulate with the tibia in flexion; the inferior flat surfaces articulate in full extension
- Superior tibial condyle surfaces (tibial plateau)
- Patella (posterior surface) and the V-shaped patellar groove (trochlea) on the anterior distal femur
3. Menisci
There are two fibrocartilaginous C-shaped structures sitting between the femoral condyles and the tibial plateau:
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | C-shaped, larger | More circular/O-shaped |
| Attachment to capsule | Firmly attached | Not attached (more mobile) |
| Attachment to collateral ligament | Attached to tibial (MCL) collateral ligament | Not attached to fibular (LCL) ligament |
| Connected to popliteus | No | Yes (via tendon passing between it and capsule) |
| Injury risk | More commonly torn | Less commonly torn (more mobile) |
The two menisci are interconnected anteriorly by the transverse ligament of the knee.
Functions of the menisci:
- Improve congruency between femoral condyles and the flat tibial plateau
- Distribute load across a wider area
- Act as shock absorbers
- Prevent capsular and synovial impingement
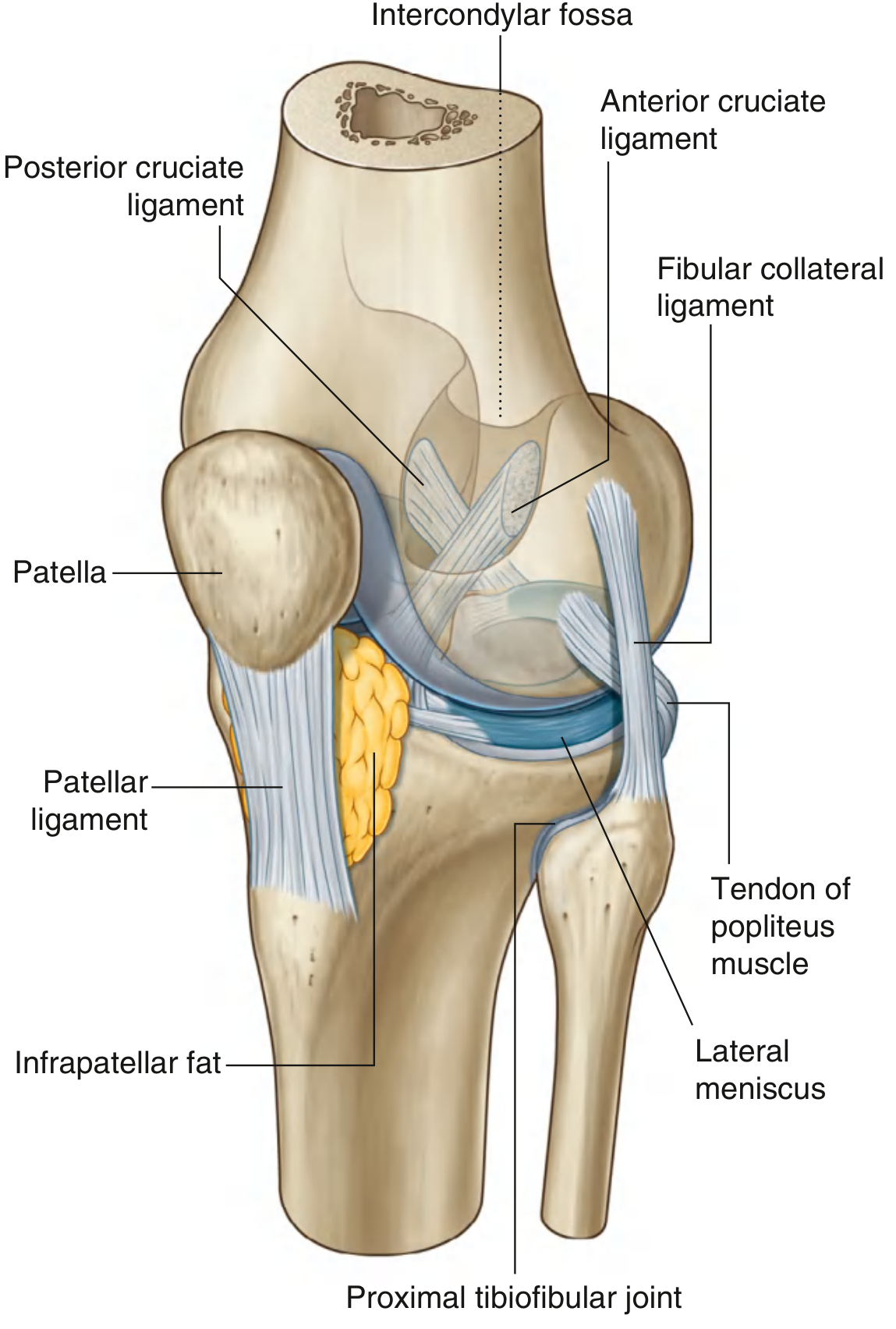
4. Ligaments
Patellar Ligament
- Continuation of the quadriceps femoris tendon below the patella
- Runs from the apex/margins of the patella to the tibial tuberosity
- The patella acts as a pulley, increasing the mechanical advantage (lever arm) of the quadriceps - capable of withstanding loads up to 20 times body weight during jumping
Collateral Ligaments
These stabilize the hinge motion and resist sideways movement:
| Ligament | Attachment (Superior) | Attachment (Inferior) | Resists |
|---|---|---|---|
| Tibial (Medial) Collateral Ligament (MCL) | Medial femoral epicondyle | Medial surface of tibia (behind sartorius, gracilis, semitendinosus) | Valgus force |
| Fibular (Lateral) Collateral Ligament (LCL) | Lateral femoral epicondyle | Head of fibula | Varus force |
The MCL is fused to the fibrous capsule and attached to the medial meniscus. The LCL is separate from the capsule, separated by a bursa.
Cruciate Ligaments
These are intracapsular but extrasynovial (inside the fibrous capsule but outside the synovial cavity). They cross each other in the sagittal plane - hence "cruciate" (Latin for cross-shaped):
| Ligament | Tibial Attachment | Femoral Attachment | Function |
|---|---|---|---|
| ACL (Anterior Cruciate) | Anterior intercondylar area of tibia | Posterior part of lateral wall of intercondylar fossa | Prevents anterior displacement of tibia on femur |
| PCL (Posterior Cruciate) | Posterior intercondylar area of tibia | Medial wall of intercondylar fossa | Prevents posterior displacement of tibia on femur |
The ACL crosses lateral to the PCL as they pass through the intercondylar region.
5. Joint Capsule
Fibrous Membrane
- Extensive, reinforced by tendons of surrounding muscles
- Medially: blends with MCL and attaches internally to medial meniscus
- Laterally: separated from LCL by a bursa; not attached to lateral meniscus
- Anteriorly: reinforced by expansions from vastus lateralis and medialis
- Posterolaterally: reinforced by the iliotibial tract
- Posteromedially: reinforced by the oblique popliteal ligament (extension from semimembranosus tendon)
Synovial Membrane
- Attaches to the margins of articular surfaces and outer edges of the menisci
- The cruciate ligaments lie outside the synovial cavity (synovial membrane loops around them)
- Anteriorly it is separated from the patellar ligament by the infrapatellar fat pad
- Forms the suprapatellar bursa superiorly (between the femoral shaft and quadriceps)
- Forms the subpopliteal recess posterolaterally (between lateral meniscus and popliteus tendon)
Bursae
Several bursae are associated with the knee joint (most do not normally communicate with the joint cavity):
| Bursa | Location | Clinical relevance |
|---|---|---|
| Suprapatellar bursa | Above patella, between femur and quadriceps | Communicates with joint; distends in effusion |
| Prepatellar bursa | Anterior to patella (subcutaneous) | "Housemaid's knee" when inflamed |
| Infrapatellar bursa (deep) | Deep to patellar ligament | "Clergyman's knee" |
| Infrapatellar bursa (superficial) | Subcutaneous, below patella | Kneeling injuries |
6. Locking Mechanism
The knee has a unique "screw-home" locking mechanism to reduce muscle energy when standing:
- As the knee reaches full extension, the articular surface shifts from the small curved posterior femoral condyle surfaces to the large flat inferior surfaces - increasing contact area and stability
- Medial rotation of the femur on the tibia during the final stages of extension tightens all the associated ligaments
- The body's center of gravity passes anterior to the knee joint, helping maintain extension
The popliteus muscle unlocks the knee by initiating lateral rotation of the femur on the tibia (or medial rotation of tibia on femur when the foot is fixed).
7. Movements and Range of Motion
| Movement | Range | Prime Movers |
|---|---|---|
| Flexion | 0-135° | Hamstrings (biceps femoris, semimembranosus, semitendinosus), gastrocnemius |
| Extension | 0-5° hyperextension | Quadriceps femoris |
| Medial rotation (tibia on femur) | Limited, increases with flexion | Popliteus, semimembranosus, semitendinosus |
| Lateral rotation (tibia on femur) | Limited | Biceps femoris |
8. Stabilizers Summary
| Type | Structure |
|---|---|
| Static (ligamentous) | Joint capsule, MCL, LCL, ACL, PCL, menisci |
| Dynamic (muscular) | Quadriceps (anterior stability), hamstrings (posterior stability), popliteus (rotational control) |
9. Vascular Supply
A rich anastomotic network around the knee is formed by:
- Descending genicular artery (from femoral artery)
- Genicular branches of the popliteal artery (5 branches: superior medial and lateral, inferior medial and lateral, middle)
- Circumflex fibular artery
- Anterior tibial recurrent artery
10. Nerve Supply
The knee joint is innervated by branches from four nerves (Hilton's Law - nerves supplying a joint also supply the muscles moving it and the skin over them):
- Femoral nerve (anterior)
- Obturator nerve (medial)
- Tibial nerve (posterior)
- Common fibular (peroneal) nerve (lateral)
Key Clinical Points
-
"Unhappy triad" (O'Donoghue triad): simultaneous injury to ACL + MCL + medial meniscus from a valgus + rotational force
-
ACL tear: anterior tibial displacement test (Lachman test / anterior drawer test); treated with surgical reconstruction in active individuals
-
PCL tear: posterior tibial sag sign; usually from hyperextension or dashboard injury
-
Meniscal tears: MRI is gold standard; patterns include vertical, horizontal, and bucket-handle tears
-
Prepatellar bursitis ("Housemaid's knee"): repeated friction from kneeling
-
Gray's Anatomy for Students, pp. 709-717
-
Bailey and Love's Short Practice of Surgery, 28th ed.
This is a shared conversation. Sign in to Orris to start your own chat.