Prolactin hormone , production , various diseases and treatment
Reading File
Finding Sources
Searching PubMed
prolactin hyperprolactinemia management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have all the information needed for a comprehensive answer. Let me compile it.
Prolactin: Production, Regulation, Diseases, and Treatment
1. What Is Prolactin?
Prolactin (PRL) is a 198-amino-acid single-chain polypeptide hormone with 3 internal disulfide bridges, structurally related to growth hormone. It is synthesized and secreted by lactotrophs in the anterior pituitary gland. Lactotrophs make up ~15-20% (and up to 50% during pregnancy) of anterior pituitary cells, making them the most common cell type and the most likely to give rise to pituitary tumors.
- Costanzo Physiology 7th Ed., p.416
- Goldman-Cecil Medicine, p.2407
2. Production and Chemistry
Prolactin is produced exclusively in the anterior pituitary lactotrophs. Stimuli increase or decrease prolactin secretion by altering transcription of the prolactin gene:
- TRH (a stimulant) increases prolactin gene transcription
- Dopamine (an inhibitor) decreases prolactin gene transcription
A biologically inactive variant called macroprolactin ("big prolactin" or "big big prolactin") forms when prolactin dimerizes with itself or complexes with circulating IgG. These variants are immunoreactive but biologically inactive - they can cause false elevations on assay without clinical significance.
- Costanzo Physiology 7th Ed., p.416
3. Regulation of Prolactin Secretion
Prolactin regulation is unique among pituitary hormones - it is predominantly under inhibitory (tonic) control by dopamine.
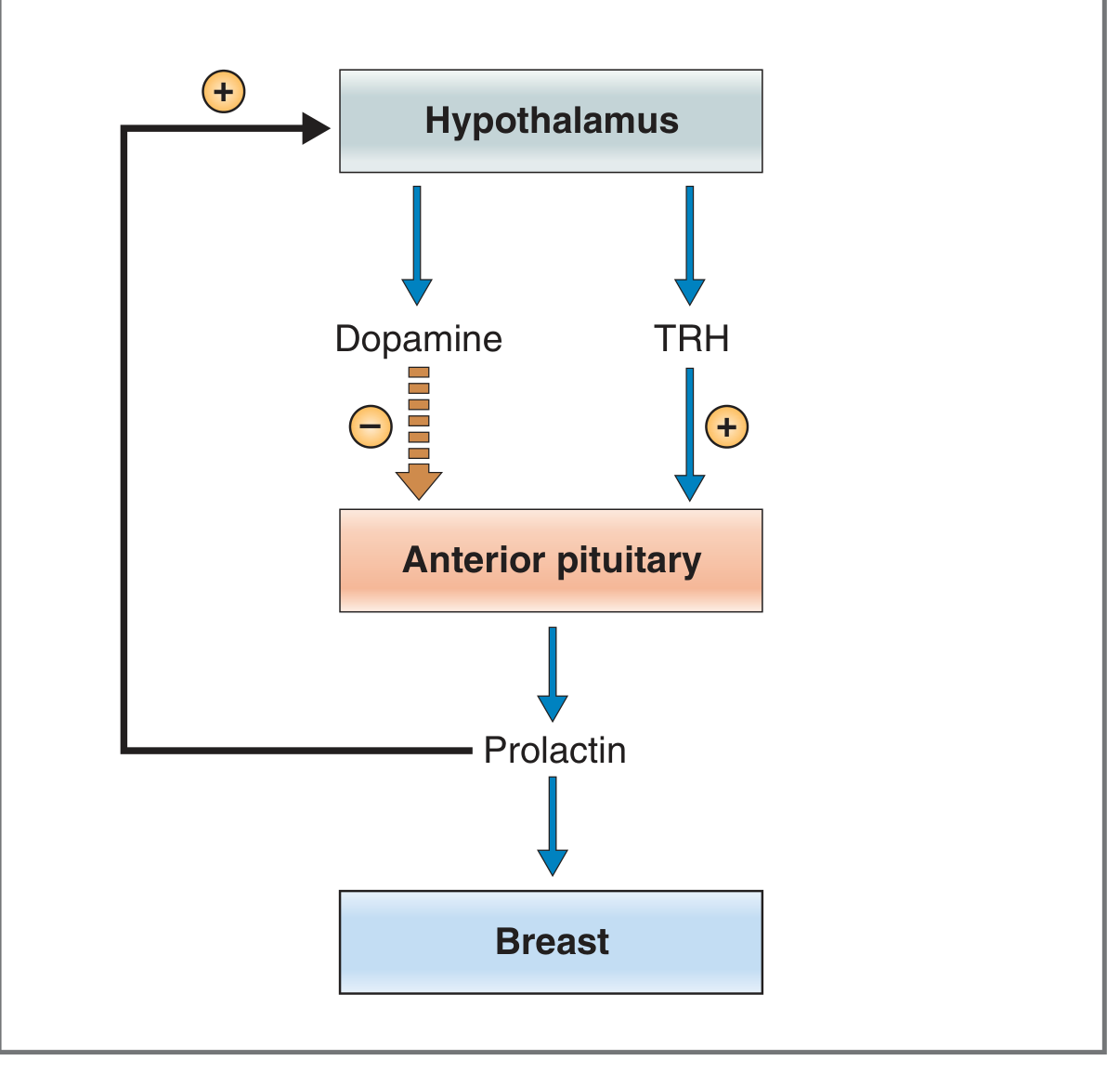
Fig. 9.12 from Costanzo Physiology 7th Ed. - Regulation of prolactin secretion. TRH = Thyrotropin-releasing hormone.
Inhibitory pathway (dominant)
Dopamine (prolactin-inhibiting factor, PIF) from the hypothalamus reaches the anterior pituitary via three routes:
- Hypothalamic dopaminergic neurons secrete dopamine into the median eminence → hypothalamic-hypophysial portal vessels → anterior pituitary (major route)
- Dopaminergic neurons of the posterior pituitary → short connecting portal veins
- Non-lactotroph anterior pituitary cells secrete dopamine in a paracrine manner
Dopamine acts through D2-type receptors on lactotrophs, decreasing cAMP levels.
Stimulatory pathway
- TRH (thyrotropin-releasing hormone)
- VIP (vasoactive intestinal peptide)
- Estrogen (stimulates prolactin gene transcription)
Negative Feedback
Prolactin itself stimulates dopamine synthesis and secretion from the hypothalamus, constituting a classic negative feedback loop.
Factors Affecting Prolactin Secretion
| Stimulatory | Inhibitory |
|---|---|
| Pregnancy (estrogen) | Dopamine |
| Breast-feeding / suckling | Bromocriptine (dopamine agonist) |
| Sleep | Somatostatin |
| Stress | Prolactin itself (negative feedback) |
| TRH | |
| Dopamine antagonists (drugs) |
- Costanzo Physiology 7th Ed., p.417
4. Actions of Prolactin
- Breast development - at puberty, with estrogen and progesterone, stimulates proliferation and branching of mammary ducts; during pregnancy, promotes growth and development of mammary alveoli
- Lactogenesis (milk production) - the primary action; stimulates synthesis of lactose, casein, and lipids in response to suckling. During pregnancy, high estrogen/progesterone inhibit lactation; their postpartum decline permits lactation
- Suppression of ovulation - prolactin suppresses GnRH, and thereby LH and FSH, providing a physiologic basis for lactational amenorrhea
- Maternal behavior - supports bonding and caregiving behavior
- Inhibition of reproductive function - in both sexes, excess prolactin suppresses gonadotropins
Normal levels: <20 pg/mL in women; <10-15 pg/mL in men.
- Goldman-Cecil Medicine, p.2407
5. Diseases Related to Prolactin
A. Hyperprolactinemia
The most clinically significant prolactin disorder. Present in <1% of the general population but up to 14% of women with abnormal menses.
Causes of Hyperprolactinemia (with prolactin ranges)
| Category | Examples | Mechanism | PRL range (pg/mL) |
|---|---|---|---|
| Antiemetics | Metoclopramide, domperidone, prochlorperazine | Dopamine receptor blockade | 20-70 |
| Antipsychotics | Haloperidol, fluphenazine; paliperidone, risperidone | Dopamine receptor blockade | 20-70 |
| Cyclic antidepressants | Clomipramine | Unknown | 20-70 |
| Narcotics | Methadone, morphine | Opioid mu-receptor activation | 20-70 |
| Estrogen | Oral contraceptives | Stimulates PRL gene transcription | 20-70 |
| Stress | - | Hypothalamic | 20-70 |
| Pregnancy | - | Estrogen | 20-500 |
| Pituitary adenoma | Microprolactinoma | - | 20-250 |
| Pituitary adenoma | Macroprolactinoma | - | 200->10,000 |
| Hypothyroidism | Primary hypothyroidism | Increased TRH | Moderate; <100 |
| Chronic renal failure / cirrhosis | - | Decreased clearance + central effects | Moderate; <100 |
| Chest wall injury / nipple stimulation | - | Unknown | 20-70 |
| Hypothalamic lesions | Structural/infiltrative disease, non-secreting pituitary adenoma | Decreased dopamine delivery | Usually <100 |
- Goldman-Cecil Medicine, Table 205-8
Key point: Drug causes and hypothalamic lesions cause modest hyperprolactinemia (<100 pg/mL). Prolactinomas commonly elevate levels 5 to 50 times higher (>100 pg/mL), and macroprolactinomas can reach >10,000.
Clinical Features
In premenopausal women:
- Galactorrhea (milk discharge outside lactation)
- Oligomenorrhea / amenorrhea
- Infertility, decreased libido, vaginal dryness (from secondary estrogen deficiency)
- Osteopenia (direct prolactin effect on bone + indirect via estrogen suppression)
In men (often detected late because symptoms are subtle):
- Decreased libido, impotence
- Reduced muscle mass, increased fat mass (from low testosterone)
- Gynecomastia and rarely galactorrhea (when estrogen co-elevated, e.g. cirrhosis)
- Osteopenia
In both sexes (large tumors):
- Headaches
- Visual field defects (bitemporal hemianopia from optic chiasm compression)
In children:
-
Rare (<2-3% of intracranial tumors); usually macroadenomas causing neurologic symptoms, delayed puberty, or growth retardation
-
Goldman-Cecil Medicine, p.2408
B. Prolactinoma
The most common cause of pathological hyperprolactinemia and the most common pituitary adenoma type.
- Microprolactinoma: <10 mm; PRL 20-250 pg/mL
- Macroprolactinoma: ≥10 mm; PRL 200->10,000 pg/mL; more likely to cause mass-effect symptoms
- Giant prolactinoma: very large macroadenomas; rare; a 2023 systematic review of 196 cases found these require careful multimodal management
Note: When MRI shows a large pituitary mass with only modest prolactin elevation (<100), it is likely a non-secreting adenoma compressing the stalk (stalk-effect hyperprolactinemia), NOT a prolactinoma.
C. Prolactin Deficiency
-
Less common and clinically less significant
-
Can occur in hypopituitarism (with other pituitary hormone deficiencies)
-
Seen in hyperthyroidism (TRH suppressed → less prolactin stimulus)
-
Main consequence: failure of lactation in nursing mothers
-
No cases of isolated prolactin deficiency have been reported in men
-
Goldman-Cecil Medicine, p.2407
D. Macroprolactinemia
An assay artifact rather than true disease. Large prolactin aggregates (bound to IgG) register as elevated PRL but are biologically inactive. The patient has no symptoms. Diagnosed by:
- Gel filtration chromatography (gold standard)
- PEG (polyethylene glycol) precipitation (simpler, inexpensive alternative)
Recognition prevents unnecessary imaging and treatment.
- Textbook of Family Medicine 9e, p.1006
6. Diagnosis
- Serum prolactin immunoassay - straightforward; levels >100 pg/mL suggest adenoma
- Important pitfall - Hook effect: Very high prolactin (>1000 pg/mL) in large macroprolactinomas can overwhelm the antibody, giving a falsely low result. Always dilute 1:100 alongside undiluted sample
- Brain MRI - recommended when PRL >100 ng/mL or when symptomatic (galactorrhea, amenorrhea, visual changes)
- Full pituitary hormone panel - essential when a mass is found (check TSH, cortisol, GH/IGF-1, LH, FSH, testosterone/estrogen)
- Thyroid function tests - rule out hypothyroidism as a cause
- Renal/liver function - rule out systemic causes
Features favoring a true prolactinoma (vs. drug-induced or stalk compression):
-
PRL >150 ng/mL
-
Loss of normal sleep-associated PRL rise
-
No rise in PRL in response to exogenous TRH
-
Textbook of Family Medicine 9e, p.1006-1007; Goldman-Cecil Medicine, p.2408
7. Treatment
Step 1: Treat reversible causes
- Discontinue offending drugs (antipsychotics, metoclopramide, etc.) where safe
- Treat hypothyroidism with levothyroxine
- Treat renal/hepatic disease
Step 2: Medical Therapy (First-line for prolactinomas)
Dopamine agonists are the first-line treatment for prolactinomas - they reduce prolactin levels AND shrink tumor size:
| Drug | Notes |
|---|---|
| Cabergoline | Preferred first-line; greater efficacy (normalizes PRL in ~90% of patients); better tolerability; twice-weekly dosing. Not preferred in pregnancy. |
| Bromocriptine | FDA-approved; preferred when pregnancy is desired (more safety data); daily dosing; more side effects (nausea, orthostatic hypotension) |
| Pergolide | Alternative ergot derivative; not FDA-approved for hyperprolactinemia |
Cardiac valve caution: All ergot derivatives carry rare risk of valvular heart damage at very high doses/prolonged use. Consider yearly echocardiogram in patients with known valve disease or on doses >5 mg/week of cabergoline.
Below is a real macroprolactinoma that shrank dramatically after cabergoline (prolactin went from 8000 ng/dL → 15 ng/dL after 6 months):
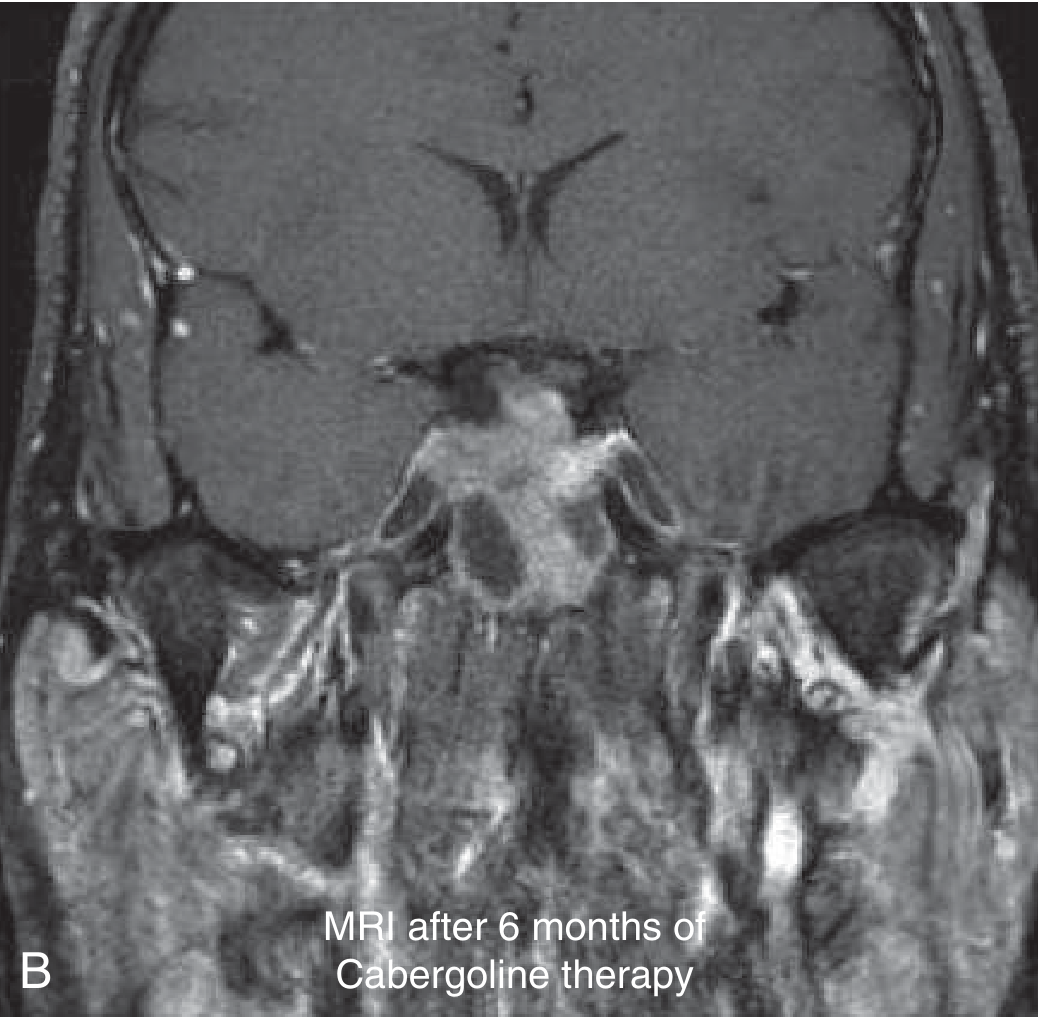
Goldman-Cecil Medicine, Fig. 205-6
Stopping / Reducing Treatment
- Dose reduction can be considered after PRL normalization for 1 year + significant tumor reduction
- Withdrawal can be considered after 2 years if: normal PRL + MRI shows no tumor or >50% reduction + tumor >5 mm from optic chiasm with no cavernous sinus invasion
- Monitor with MRI + PRL at 3 months, 6 months, then yearly after stopping
- Macroprolactinomas are more likely to recur than microprolactinomas
Step 3: Surgery (Second-line)
Transsphenoidal resection is indicated when:
- Medical treatment fails or is not tolerated
- Very large tumors threatening visual pathways
- Hemorrhagic infarction (pituitary apoplexy)
- Patient preference
Success rates:
- Microprolactinomas: 65-85% normalization; ~20% recurrence at 10 years
- Macroprolactinomas: 30-40% normalization (only ~30% of macroadenomas can be completely removed)
Step 4: Radiation
Rarely used; reserved for large residual tumor post-surgery that is unresponsive to medical therapy.
Special situation: Pregnancy
-
Discontinue dopamine agonist once pregnancy confirmed
-
Monitor for visual symptoms (up to 10% of microprolactinomas and 30% of macroprolactinomas can enlarge during pregnancy)
-
Bromocriptine preferred over cabergoline if treatment must be restarted during pregnancy (more safety data)
-
Serial visual field testing each trimester for macroprolactinomas
-
Textbook of Family Medicine 9e, p.1007; Goldman-Cecil Medicine, p.2408-2409
Summary at a Glance
| Feature | Details |
|---|---|
| Site of production | Anterior pituitary lactotrophs |
| Primary regulator | Dopamine (inhibitory, tonic) |
| Secondary stimulator | TRH, estrogen |
| Main physiologic role | Lactation, breast development |
| Key disease | Hyperprolactinemia / Prolactinoma |
| Most common cause of PRL >100 | Prolactinoma |
| Most common drug cause | Antipsychotics / metoclopramide (dopamine blockade) |
| First-line treatment | Dopamine agonists (cabergoline > bromocriptine) |
| Second-line treatment | Transsphenoidal surgery |
Recent evidence note: A 2024 systematic review (PMID: 38819244) highlights specific management challenges when prolactinomas coexist with psychiatric illness - dopamine agonists conflict with antipsychotic treatment, requiring careful individualization of care.
This is a shared conversation. Sign in to Orris to start your own chat.