Here is the complete ARMD presentation written directly in chat, from basics to advanced, with all tables, flowcharts, and images inline.
👁️ AGE-RELATED MACULAR DEGENERATION (ARMD)
A Comprehensive Review — Basic to Advanced
Sources: Harrison's 22E · Goldman-Cecil Medicine · Robbins Pathology · Wills Eye Manual · Goodman & Gilman · Katzung Pharmacology · AREDS/AREDS2 · PubMed 2023–2026
📋 OUTLINE
| # | Module |
|---|
| 01 | Epidemiology & Global Burden |
| 02 | Normal Macular Anatomy |
| 03 | Classification & Staging |
| 04 | Pathogenesis |
| 05 | Risk Factors & Genetics |
| 06 | Clinical Features & Symptoms |
| 07 | Investigations & Imaging |
| 08 | Dry AMD — Management |
| 09 | Wet AMD — Anti-VEGF Therapy |
| 10 | Landmark Clinical Trials |
| 11 | Emerging Therapies & Gene Therapy |
| 12 | Monitoring, Prognosis & Rehabilitation |
01. EPIDEMIOLOGY & GLOBAL BURDEN
Key Statistics
| Parameter | Data |
|---|
| Global blindness attributable to AMD | ~8.5% of all blindness |
| US prevalence | >1.75 million persons |
| Global affected (2020 estimate) | ~196 million |
| Projected global (2040) | ~288 million |
| Cumulative incidence at age ≥75 | 8% |
| Age of onset (typical) | 6th–9th decade |
| Second eye CNV risk (after unilateral wet AMD) | 10–12% per year |
| Laterality | Bilateral in most cases |
Key Points
- Leading cause of irreversible central vision loss in adults >55 years in developed countries
- Prevalence doubles with each decade after age 55
- Predominantly affects industrialized nations
- Major driver of low-vision services and quality-adjusted life year (QALY) loss
- Peripheral vision is preserved throughout — central vision selectively affected
- "Individuals with advanced disease can walk down a street without difficulty but cannot recognize facial features" — Harrison's 22E
02. NORMAL MACULAR ANATOMY
Structural Layers Relevant to ARMD
VITREOUS
↓
INNER RETINA (ganglion cells, bipolar cells)
↓
OUTER NUCLEAR LAYER (photoreceptor nuclei)
↓
PHOTORECEPTORS — Rods & Cones
↓
RETINAL PIGMENT EPITHELIUM (RPE) ← Key target in ARMD
↓
BRUCH MEMBRANE (5-layered) ← Site of drusen formation
↓
CHORIOCAPILLARIS ← Sole blood supply to outer retina
↓
CHOROID (large vessels)
↓
SCLERA
The Critical Functional Unit (Robbins Pathology)
RPE + Bruch Membrane + Choriocapillaris = the core functional triad
Disturbance in any one component → photoreceptor damage → vision loss
| Structure | Normal Function | Role in ARMD |
|---|
| RPE | Phagocytose shed photoreceptor outer segments; retinoid recycling; blood-retinal barrier | Accumulates lipofuscin; RPE atrophy in dry AMD |
| Bruch Membrane | 5-layer barrier between RPE and choroid; supports RPE attachment | Drusen deposit here; calcification; CNV penetrates through here |
| Choriocapillaris | Sole vascular supply to outer retina and RPE | Obliterated in geographic atrophy |
| Fovea/Foveola | Highest cone density; sharpest central acuity | Primary site of ARMD damage |
| Macula lutea | ~5.5 mm central retinal area temporal to disc | Yellow pigment (lutein/zeaxanthin) — protective role |
03. CLASSIFICATION & STAGING
AREDS Classification System
| Stage | Drusen Size | Pigment Changes | Vision | Management |
|---|
| No AMD | None or small (<63 μm) | None | Normal | Routine review |
| Early AMD | Medium drusen (63–124 μm) | Absent | Usually normal | Lifestyle; monitor |
| Intermediate AMD | Large drusen (≥125 μm) OR pigment change | Present | May have subtle changes | AREDS2 supplements |
| Late AMD — Dry (GA) | Any + geographic atrophy | RPE atrophy, well-defined | Significant central loss | Supplements; complement inhibitors; rehab |
| Late AMD — Wet (nAMD) | Any + choroidal neovascularization (CNV) | SRF, hemorrhage, exudate | Acute central loss | URGENT anti-VEGF |
Two Forms Summarized
| Feature | Dry AMD | Wet AMD |
|---|
| Frequency | 90% of all AMD | 10% of AMD |
| Mechanism | Complement-mediated atrophy | Choroidal neovascularization (CNV) |
| Speed of progression | Slow (months–decades) | Rapid (days–weeks) |
| Vision loss | Gradual, moderate | Sudden, severe |
| Drusen | Always present | Usually present |
| Hemorrhage | Absent | Present |
| Treatment | Supplements; C3/C5 inhibitors | Anti-VEGF injections |
| Relationship | Usually precedes wet AMD | Complication of dry AMD (not inevitable) |
04. PATHOGENESIS
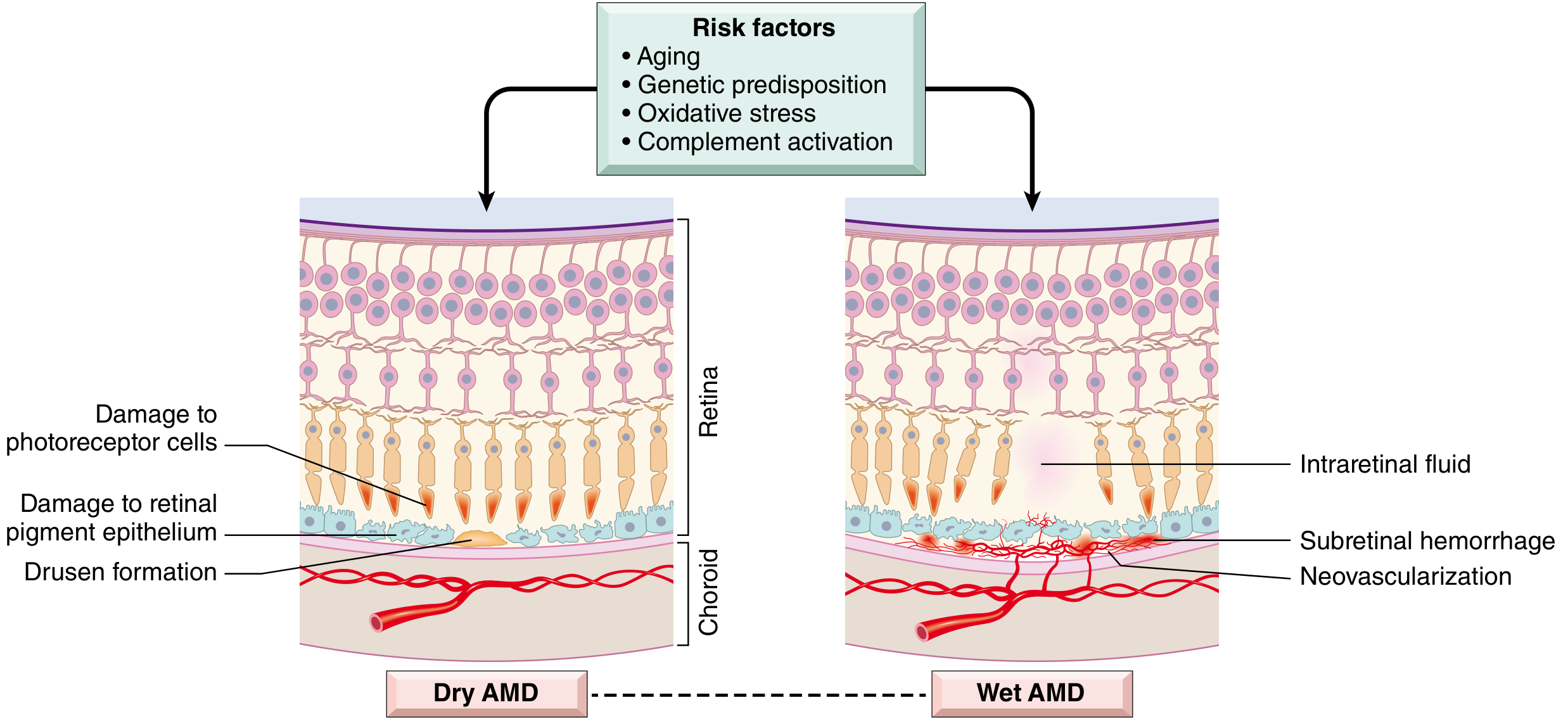
Pathogenesis Diagram (from Robbins Pathology, Fig 29.24)
Fig 29.24 — Robbins, Cotran & Kumar Pathologic Basis of Disease: Schematic illustrating the differences between dry and wet AMD. Dry AMD may progress to wet AMD, and in some patients both forms may coexist.
Dry AMD Pathogenesis
AGING + GENETIC SUSCEPTIBILITY (CFH, ARMS2) + OXIDATIVE STRESS (SMOKING)
↓
Impaired RPE function
↓
Accumulation of LIPOFUSCIN in RPE cells
(oxidized polyunsaturated fatty acids + vitamin A dimers = A2E toxin)
↓
DRUSEN formation in Bruch membrane
(focal lipoprotein deposits; hard → soft → confluent)
↓
Activation of COMPLEMENT SYSTEM (alternative pathway)
(CFH/CFI variants → excess complement activity)
↓
Chronic subclinical inflammation → RPE cell death
↓
GEOGRAPHIC ATROPHY (GA)
(loss of RPE + choriocapillaris + photoreceptors → central blind spot)
Key Molecules in Dry AMD:
- CFH (Complement Factor H): major regulator of alternative complement pathway — Y402H variant in 35% of AMD cases
- CFI (Complement Factor I): serine protease that inactivates C3b
- C3, C9: effector complement proteins found in drusen
- Lipofuscin / A2E: phototoxic waste products accumulating in stressed RPE
Wet AMD Pathogenesis
DRY AMD (geographic atrophy or large drusen)
↓
RPE cells under HYPOXIA / OXIDATIVE STRESS
↓
Overexpression of VEGF-A (Vascular Endothelial Growth Factor A)
+ Angiopoietin-2 (Ang-2) — destabilizes existing vessels
↓
Neovascular sprouting from CHORIOCAPILLARIS
↓
New vessels penetrate BRUCH MEMBRANE
↓
CHOROIDAL NEOVASCULARIZATION (CNV) under RPE or subretinal space
↓
Frail neovascular channels LEAK plasma, lipids → subretinal exudates
↓
SUBRETINAL HEMORRHAGE → acute central visual loss
↓
Organization by RPE cells → DISCIFORM SCAR (macular fibrosis)
↓
IRREVERSIBLE CENTRAL VISUAL LOSS
CNV Types (by location):
| Type | Location | Angiographic appearance |
|---|
| Classic CNV (Type 2) | Above RPE, subretinal | Well-defined, bright early leakage on FFA |
| Occult CNV (Type 1) | Below RPE | Fibrovascular PED; late irregular leakage |
| RAP (Type 3) | Intraretinal origin | Focal telangiectatic vessels; IRF + RPE detachment |
| PCV | Polypoidal dilations of inner choroid | Serosanguineous PED; ICGA characteristic |
05. RISK FACTORS & GENETICS
Risk Factor Summary
| Category | Risk Factor | Relative Risk |
|---|
| Non-modifiable | Advanced age | Strongest factor |
| Family history | 3–4× if first-degree relative |
| White/European ancestry | Higher than Asian/African |
| Female sex | Slight increase |
| Hyperopia | Increased risk |
| Light iris color (blue/grey) | Modest increase |
| Modifiable | Cigarette smoking | 2–4× increase (strongest modifiable) |
| Systemic hypertension | Increased risk |
| High dietary fat, low lutein/zeaxanthin | Increased risk |
| Obesity / metabolic syndrome | Increased risk |
| Sedentary lifestyle | Modest increase |
| Chronic UV exposure | Modest increase |
| Ocular | Soft large drusen (≥125 μm) | Major risk for progression |
| RPE pigment clumping | Risk for CNV development |
| Wet AMD in fellow eye | 10–12% per year CNV risk in other eye |
| Nutritional | Low serum lutein, zeaxanthin | Modifiable |
| Omega-3 deficiency | Modifiable |
Genetics of ARMD
ARMD is polygenic and multifactorial — GWAS identified >40 susceptibility loci
| Gene / Locus | Chromosome | Function | Risk Allele |
|---|
| CFH Y402H | 1q32 | Complement Factor H — regulates alternative pathway | rs1061170 — 2–4× risk |
| ARMS2/HTRA1 | 10q26 | ARMS2 function unclear; HTRA1 is a serine protease | rs10490924 — major risk |
| C3 | 19p13 | Central complement effector | R102G variant |
| CFI | 4q25 | Inactivates C3b — dampens complement | Variants increase activity |
| CFB / C2 | 6p21 | Alternative / classical pathway | Protective haplotype known |
| C9 | 5p13 | Terminal complement complex | Variants identified |
| VEGF pathway | Various | Neovascular susceptibility | Multiple loci |
Genetic Model:
Genetic susceptibility (CFH + ARMS2) × Environmental exposure (smoking, diet) = Clinical phenotype
(Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.)
06. CLINICAL FEATURES & SYMPTOMS
Dry AMD — Symptoms & Signs
Symptoms:
- Gradual, insidious loss of central vision (months to years)
- Amsler grid distortion (metamorphopsia)
- Difficulty reading, watching TV, recognizing faces
- Often asymptomatic in early/intermediate stages
- Peripheral vision preserved throughout
Signs on Fundus Examination:
- Drusen — small hard (bright, discrete) → soft (large, indistinct, >125 μm) → confluent
- RPE pigment clumping — hyperpigmented spots in outer retina
- Geographic atrophy (GA) — well-defined areas of RPE depigmentation with visible choroidal vessels
- Bilateral involvement (typically asymmetric)
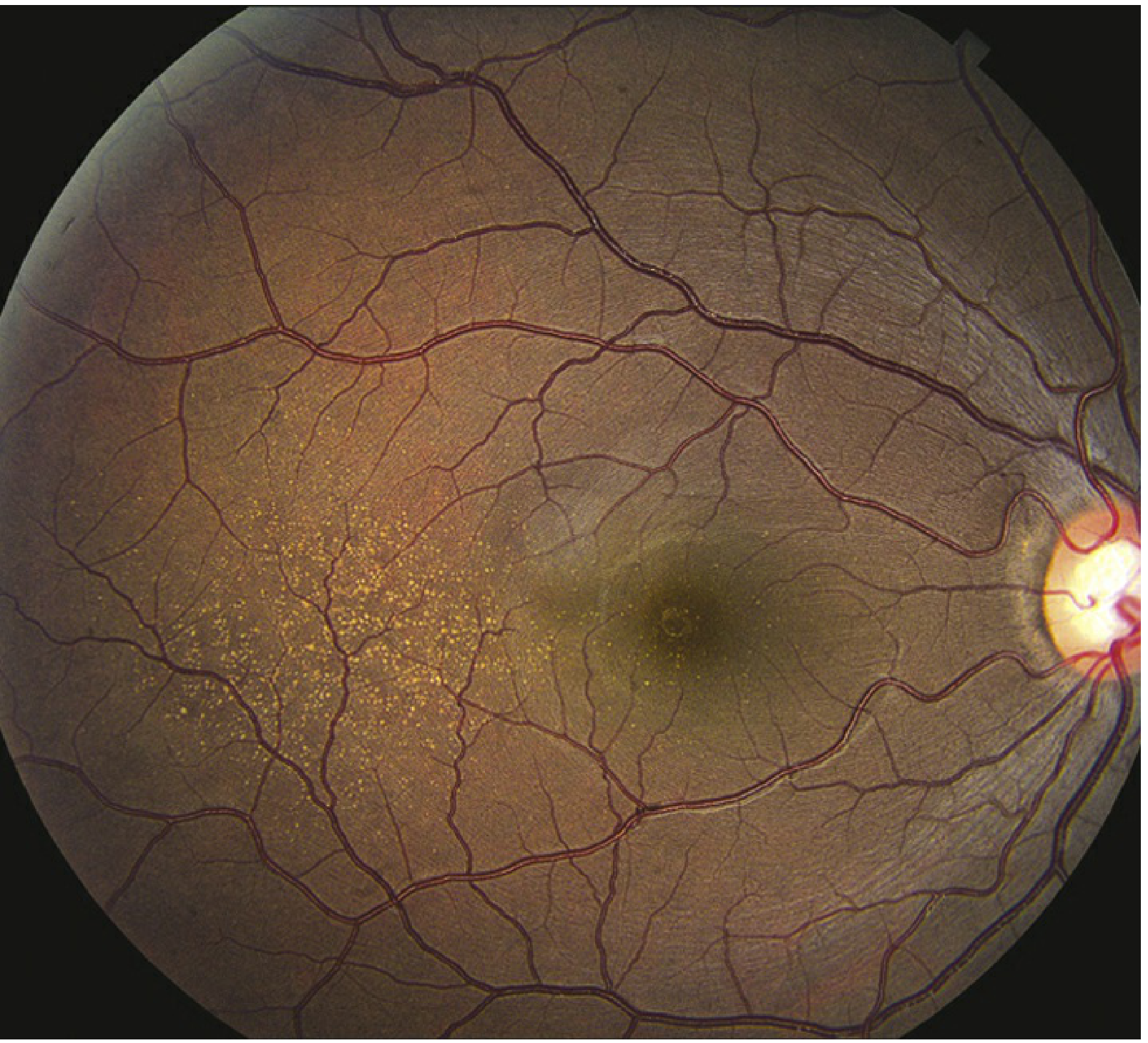
Fundus Photo: Dry AMD with Fine Drusen (Wills Eye Manual)
Figure 11.16.1 — Dry AMD with fine drusen. Multiple hard and soft drusen scattered in the macula. Absence of hemorrhage or exudate. (Wills Eye Manual, 7th Ed.)
Wet AMD — Symptoms & Signs
Symptoms:
- Sudden onset central or paracentral scotoma
- Acute metamorphopsia (lines appear wavy, distorted)
- Photopsias (flashes) in central visual field
- Rapid, profound central visual loss (hours to days)
Signs on Fundus Examination (Wills Eye Manual, Section 11.17):
- Critical: Drusen + subretinal fluid (SRF), macular edema (ME), or RPE detachment associated with CNV
- Subretinal or intraretinal hemorrhage
- Retinal exudates (hard exudates/lipid deposition)
- Subretinal fibrosis (disciform scar) — late stage
- Retinal angiomatous proliferation (RAP) — intraretinal telangiectatic vessels with focal hemorrhage
- Pigment epithelial detachment (PED)
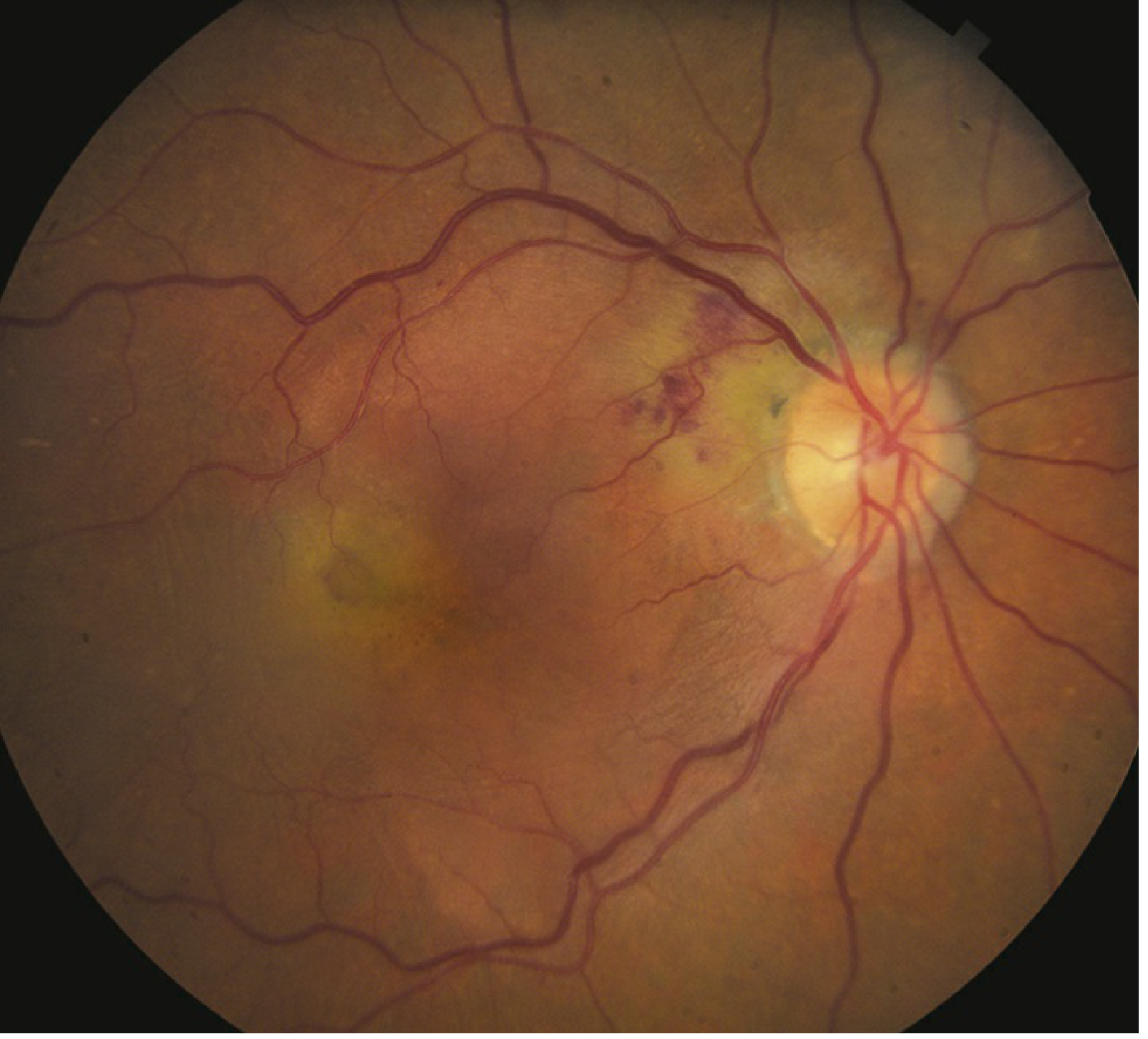
Fundus Photo: Wet (Exudative) AMD (Wills Eye Manual)
Figure 11.17.1 — Exudative AMD. Note the subretinal hemorrhage, exudates and irregular pigmentation consistent with active choroidal neovascularization. (Wills Eye Manual, 7th Ed.)
Visual Field in ARMD
Fig F24.3.1 — Simulated visual field in ARMD. The central vision (playing field) is absent due to macular changes. Peripheral vision (stadium stands) remains intact. Patients are taught eccentric fixation to maximize remaining vision. (Histology: A Text and Atlas, Pawlina)
Differential Diagnosis
| Condition | Key Differentiating Features | Age | Drusen |
|---|
| Dry AMD | Bilateral, macular drusen, RPE atrophy, slow progression | ≥55 | Yes — macular |
| Wet AMD | CNV, subretinal fluid/blood, rapid loss, urgency | ≥55 | Usually present |
| Peripheral drusen | Drusen only peripheral to macula; no central involvement | Variable | Yes — peripheral |
| Myopic degeneration | High myopia, lacquer cracks, peripapillary changes, no drusen | Any | No |
| CSCR | RPE/serous detachment, young males, self-limiting, no drusen | <50 | No |
| Stargardt disease | Familial, yellow-white flecks, early onset, ABCA4 mutation | <50 | No (flecks) |
| Pattern dystrophy | Bilateral macular pigment changes, familial, <50 years | <50 | No |
| Chloroquine toxicity | Bull's-eye maculopathy, ring hyperpigmentation, drug history | Any | No |
| Ocular histoplasmosis | White chorioretinal scars, peripapillary atrophy, endemic | Any | No |
| Angioid streaks | Subretinal red-brown bands radiating from disc | Any | No |
| IPCV | Polypoidal choroidal dilations, serosanguineous PED, ICGA | ≥50 | Sometimes |
07. INVESTIGATIONS & IMAGING
Workup Algorithm
PATIENT WITH SUSPECTED ARMD
↓
1. Best Corrected Visual Acuity (ETDRS/Snellen)
↓
2. Amsler Grid (10° central field, both eyes)
↓
3. Slit-Lamp Biomicroscopy + Dilated Fundus Exam
(90D / 78D lens — grade drusen, RPE changes)
↓
4. OCT (Optical Coherence Tomography) — MANDATORY
[Cross-sectional retinal imaging: SRF, IRF, drusen, PED]
↓
┌──────────────────────────────────────┐
↓ ↓
DRY AMD WET AMD suspected
↓ ↓
FAF (Fundus Autofluorescence) FFA (Fluorescein Angiography)
→ GA extent, RPE viability → CNV leakage characterization
↓ ↓
Document, monitor + OCT-A (non-invasive CNV mapping)
↓
± ICGA (if PCV suspected)
Imaging Modalities Compared
| Modality | What It Shows | Key Use in ARMD |
|---|
| Fundus Photography | Color retinal image | Baseline documentation; drusen grading |
| OCT (gold standard) | Cross-section retinal layers; SRF, IRF, PED, drusen volume | Diagnosis + treatment monitoring of wet AMD |
| FFA (Fluorescein Angiography) | Leakage, CNV type, extent | Classic vs occult CNV; leakage pattern |
| ICGA (Indocyanine Green) | Choroidal circulation, polyps | PCV diagnosis; type 1 occult CNV |
| FAF (Fundus Autofluorescence) | RPE metabolic activity (lipofuscin signal) | GA extent, margins; progression tracking |
| OCT-A | Blood flow in retinal/choroidal layers non-invasively | CNV detection without dye injection |
| Amsler Grid | 10° central field distortion | Home monitoring; detect metamorphopsia |
| PHP (ForeseeHome) | Preferential Hyperacuity Perimetry | Home monitoring device; FDA cleared |
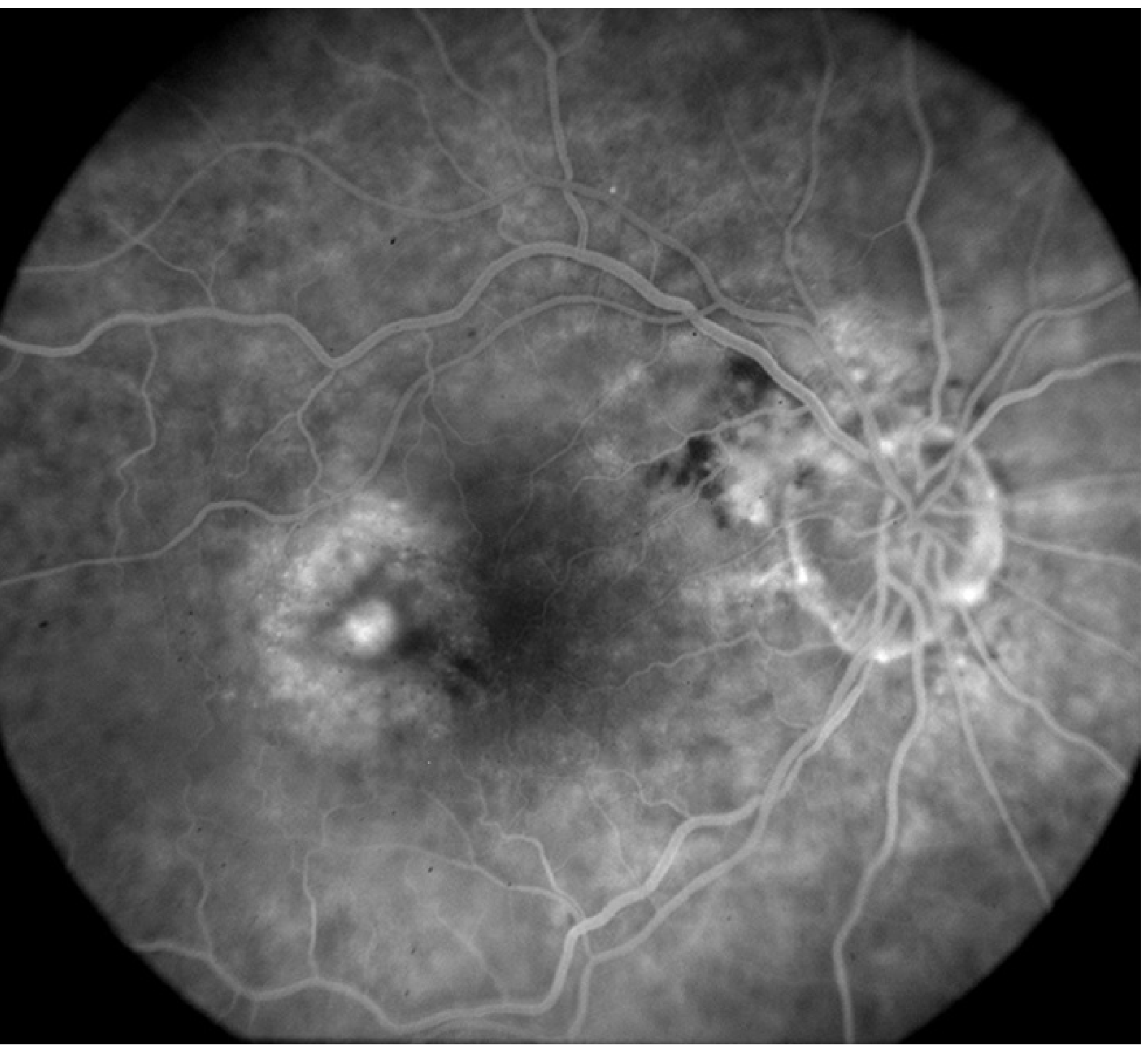
FFA in Wet AMD
Figure 11.17.2 — Intravenous fluorescein angiography of exudative AMD. The hyperfluorescent areas indicate CNV leakage; dark areas represent blocked fluorescence from subretinal hemorrhage. (Wills Eye Manual, 7th Ed.)
08. DRY AMD — PREVENTION & MANAGEMENT
Management Flowchart: Dry AMD
┌─────────────────────────────────────────────────────┐
│ EARLY DRY AMD │
│ Small/medium drusen, no central visual symptoms │
└─────────────────────┬───────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ LIFESTYLE MODIFICATION │
│ • STOP SMOKING (most important single intervention)│
│ • UV-blocking sunglasses │
│ • Mediterranean diet (leafy greens, omega-3) │
│ • Control blood pressure, blood sugar, lipids │
│ • Regular aerobic exercise │
└─────────────────────┬───────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ INTERMEDIATE DRY AMD │
│ Large drusen (≥125 μm) or pigment changes │
└─────────────────────┬───────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ AREDS2 SUPPLEMENTS (daily) │
│ Vitamin C 500 mg │
│ Vitamin E 400 IU │
│ Lutein 10 mg + Zeaxanthin 2 mg │
│ Zinc 80 mg + Copper 2 mg │
│ (Beta-carotene AVOIDED — lung cancer risk in smokers)│
└─────────────────────┬───────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ HOME MONITORING │
│ Daily Amsler grid / ForeseeHome PHP device │
│ Any new metamorphopsia → URGENT CLINIC REVIEW │
└─────────────────────┬───────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ ADVANCED DRY AMD / GEOGRAPHIC ATROPHY (GA) │
└─────────────────────┬───────────────────────────────┘
↓
┌────────────────────────────────────────────────────────────────┐
│ COMPLEMENT INHIBITORS (FDA approved 2023): │
│ Pegcetacoplan (Syfovre) — C3 inhibitor │
│ Monthly or every-other-month IVT injection │
│ OAKS trial: ~22% reduction in GA lesion growth │
│ Avacincaptad pegol (Izervay) — C5 inhibitor │
│ Monthly IVT injection │
│ GATHER2: ~14.5% reduction in GA growth vs sham │
└────────────────────────────────────────────────────────────────┘
↓
┌─────────────────────────────────────────────────────┐
│ LOW VISION REHABILITATION │
│ • Magnification spectacles, video magnifiers │
│ • Eccentric fixation training │
│ • Large-print / e-reader technology │
│ • Orientation & mobility training │
│ • Psychosocial support / Macular Society │
└─────────────────────────────────────────────────────┘
AREDS & AREDS2 Trials — Key Evidence
| Trial | Year | n | Key Finding |
|---|
| AREDS | 2001 | 4,757 | Supplements (Vit C/E + beta-carotene + zinc/copper) reduced progression from intermediate → advanced AMD by 25% (NNT ~8 over 5 years) |
| AREDS2 | 2013 | 4,203 | Replacing beta-carotene with lutein/zeaxanthin (10 mg/2 mg): similar efficacy; safer in smokers — no increase in lung cancer risk |
Important Caveats:
- Beta-carotene NOT recommended for smokers/recent ex-smokers — 28% increased lung cancer risk (ATBC and CARET trials)
- AREDS2 formula is now the standard recommendation
- Supplements do NOT benefit early AMD or prevent AMD in healthy eyes
- Diet: high lutein/zeaxanthin (kale, spinach), omega-3 (oily fish), low glycaemic index
09. WET AMD — ANTI-VEGF THERAPY
Anti-VEGF Agents: Pharmacology & Comparison
| Agent | Class | Mechanism | Dose | FDA Approval | Notes |
|---|
| Pegaptanib (Macugen) | Aptamer | Binds VEGF165 isoform only | 0.3 mg IVT q6w | 2004 | First approved; largely superseded |
| Ranibizumab (Lucentis) | Fab fragment | Binds all VEGF-A isoforms | 0.5 mg IVT | 2006 | Monthly → PRN/T&E; landmark MARINA/ANCHOR |
| Bevacizumab (Avastin) | Full IgG1 antibody | Binds VEGF-A | 1.25 mg IVT | Off-label | Non-inferior to ranibizumab (CATT); compounded; very widely used |
| Aflibercept 2 mg (Eylea) | Fusion protein (decoy receptor) | Binds VEGF-A, VEGF-B, PlGF | 2 mg IVT | 2011 | Q8w after 3 monthly loads; VIEW 1&2 |
| Brolucizumab (Beovu) | Single-chain Fv (scFv) | Pan-VEGF-A | 6 mg IVT | 2019 | Q12w; smaller molecule; rare retinal vasculitis/occlusion risk |
| Aflibercept 8 mg (Eylea HD) | Fusion protein (higher dose) | Same as above | 8 mg IVT | 2023 | Q12–16w dosing; PULSAR/PHOTON trials |
| Faricimab (Vabysmo) | Bispecific IgG antibody | Anti-VEGF-A + Anti-Ang-2 | 6 mg IVT | 2022 | Up to Q16w; TENAYA/LUCERNE; dual pathway |
(Source: Goodman & Gilman's Pharmacological Basis of Therapeutics, Table 74-15)
Mechanism of Action — Anti-VEGF Agents
HYPOXIA / OXIDATIVE STRESS in RPE
↓
VEGF-A overexpression
↓
Binds VEGFR1/VEGFR2 on endothelial cells
↓ ↓
ANGIOGENESIS PERMEABILITY↑
(new vessel sprouting) (fluid leakage)
↓ ↓
CNV growth SRF / IRF / PED
↓
┌────────────────────────────────┐
│ ANTI-VEGF AGENTS │
│ Block VEGF → halt CNV growth │
│ Reduce vascular permeability │
│ → Dry macula on OCT │
└────────────────────────────────┘
FARICIMAB DUAL MECHANISM:
Anti-VEGF-A + Anti-Ang-2
↓ ↓
Block new CNV Stabilize existing vessels
↓
Superior vascular stability
↓
Longer dosing intervals (up to Q16w)
Treat-and-Extend (T&E) Protocol — Wet AMD
STEP 1: CONFIRM WET AMD
OCT (SRF / IRF / PED) + BCVA + FFA/OCT-A
↓
STEP 2: LOADING PHASE
3 monthly IVT injections (fixed interval)
↓
STEP 3: ASSESS RESPONSE ON OCT
↓
┌─────────────────┴──────────────────┐
↓ ↓
MACULA DRY FLUID PRESENT
(no SRF/IRF) (SRF or IRF)
↓ ↓
EXTEND interval by 2 weeks MAINTAIN or SHORTEN
(Q6w → Q8w → Q10w → Q12w → Q16w) interval by 2 weeks
↓ ↓
CONTINUE T&E Re-assess next visit
↓
PERSISTENT FLUID at maximum interval (Q4w)
↓
SWITCH anti-VEGF agent
(e.g., ranibizumab → faricimab → aflibercept 8mg)
↓
REASSESS after 3 injections of new agent
Treatment Goals:
- Achieve anatomically dry macula on OCT (no SRF, no IRF)
- Maintain or improve BCVA
- Reduce injection burden while maintaining disease control
Photodynamic Therapy (PDT) — Verteporfin
(Goodman & Gilman, Chapter 74)
| Feature | Detail |
|---|
| Drug | Verteporfin (Visudyne) 2 mg/mL |
| Route | IV infusion (dosed by body surface area) |
| Mechanism | Drug circulates to choroidal vasculature → non-thermal 689 nm laser activation → free radical generation → platelet activation → thrombosis → CNV occlusion |
| Half-life | 5–6 hours; excreted in feces |
| Indication (classic) | Predominantly classic subfoveal CNV in wet AMD |
| Side effects | Photosensitization (avoid sunlight 5 days), transient visual disturbance, back pain (IV infusion) |
| Current role | Limited in anti-VEGF era; combination therapy in polypoidal choroidal vasculopathy (PCV) |
10. LANDMARK CLINICAL TRIALS
Wet AMD Trials
| Trial | Year | Drug | n | Design | Key Result |
|---|
| MARINA | 2006 | Ranibizumab 0.3/0.5 mg | 716 | Phase 3 RCT vs sham | 95% maintained vision; 35% gained ≥15 letters (vs 5% sham) |
| ANCHOR | 2006 | Ranibizumab vs PDT | 423 | Phase 3 RCT | Ranibizumab superior to PDT in all visual outcomes — established anti-VEGF as standard of care |
| CATT | 2011 | Ranibizumab vs Bevacizumab | 1,208 | Non-inferiority RCT | Bevacizumab non-inferior to ranibizumab at 2 years; PRN=monthly outcomes; major cost-saving implications |
| VIEW 1 & 2 | 2012 | Aflibercept 2 mg vs Ranibizumab | 2,457 | Phase 3 RCT | Q8w aflibercept non-inferior to monthly ranibizumab; reduced injection burden — first extended dosing |
| HAWK/HARRIER | 2019 | Brolucizumab 6 mg vs Aflibercept | 1,817 | Phase 3 RCT | Non-inferior; 56% on Q12w; rare retinal vasculitis/occlusion (1–3.3%) — post-marketing safety signal |
| TENAYA/LUCERNE | 2022 | Faricimab 6 mg vs Aflibercept | 1,329 | Phase 3 RCT | Non-inferior; ~80% on ≥Q12w; bispecific Ang-2 + VEGF-A mechanism validated → FDA approval Jan 2022 |
| PULSAR | 2023 | Aflibercept 8 mg vs Afl 2 mg | 669 | Phase 3 RCT | Q12–16w dosing achieved; non-inferior → FDA approval Aug 2023 (Eylea HD) |
| AVONELLE-X | 2025 | Faricimab long-term extension | 800+ | Extension study | ~80% on Q12–16w at 4 years; durable with no new safety signals (AAO 2025 data) |
Dry AMD / Geographic Atrophy Trials
| Trial | Year | Drug | n | Key Result |
|---|
| AREDS | 2001 | Antioxidant vitamins + zinc | 4,757 | 25% reduction in progression to advanced AMD; defined standard supplement formula |
| AREDS2 | 2013 | Lutein/zeaxanthin replacing beta-carotene | 4,203 | Similar efficacy; safer in smokers — no lung cancer risk increase |
| FILLY | 2018 | Lampalizumab (CFD inhibitor) | 906 | Promising Phase 2 results in CFI-positive patients; Phase 3 failed (negative 2018) |
| OAKS/DERBY | 2023 | Pegcetacoplan (C3 inhibitor) | 637 | ~20–22% reduction in GA lesion growth vs sham → FDA approved Feb 2023 |
| GATHER1/GATHER2 | 2021–23 | Avacincaptad pegol (C5 inhibitor) | ~500 | ~14.5% reduction in GA growth; foveal sparing preserved → FDA approved Aug 2023 |
| PHOENIX | 2025 | Tinlarebant (RBP4 inhibitor, oral) | ~500 | Phase 3 ongoing — reduces retinol delivery to RPE → slows GA progression |
| ArMaDa | 2025 | OCU410 (nuclear receptor modifier gene therapy) | ~60 | Phase 1/2 ongoing — Ocugen modifier gene therapy for GA |
| 4FRONT | 2025 | 4D-150 (gene therapy dual anti-VEGF/VEGF-C RNAi) | 400 | Phase 3 ongoing — single IVT injection for sustained anti-VEGF |
11. EMERGING & GENE THERAPIES
Complement-Based Therapies (FDA Approved 2023)
| Drug | Target | Trial | Result |
|---|
| Pegcetacoplan (Syfovre, Apellis) | C3 (complement 3) inhibitor | OAKS/DERBY Phase 3 | 22% (monthly) / 18% (EOM) reduction in GA growth; IVT injection |
| Avacincaptad pegol (Izervay, Iveric Bio/Astellas) | C5 (complement 5) inhibitor | GATHER1 & 2 | 14.5% reduction in GA; preserved foveal sparing; monthly IVT |
| BI 771716 (Boehringer Ingelheim) | Novel target | VERDANT Phase 2 | Active-controlled vs pegcetacoplan — ongoing 2025 |
| VOY-101 (Voyager) | C3 — gene therapy | JOURNEY Phase 1/2 | First gene therapy targeting complement for GA |
Rationale: CFH/CFI genetic variants → insufficient complement regulation → excess C3/C5 activation → RPE destruction → GA progression. Blocking C3 (upstream) or C5 (downstream) slows this cascade.
Gene Therapy Pipeline
The concept: a single intravitreal injection of a viral vector (AAV) transfects retinal cells to produce therapeutic proteins continuously — eliminating the injection burden of monthly IVT anti-VEGF.
| Program | Company | Vector/Target | Stage (2025) | Route |
|---|
| RGX-314 | AbbVie / Regenxbio | AAV8-anti-VEGF (ranibizumab-like Fab) | AAVIATE Phase 2 + ASCENT Phase 3 (n=500) | Subretinal / suprachoroidal |
| ADVM-022 / Ixo-vec | Adverum Biotechnologies | AAV.7m8-anti-VEGF | LUNA Phase 2 + ARTEMIS Phase 3 (n=400) | IVT single injection |
| 4D-150 | 4D Molecular Therapeutics | AAVv66-anti-VEGF + VEGF-C RNAi | PRISM Phase 1/2 + 4FRONT Phase 3 (n=400) | IVT single injection |
| OCU410 | Ocugen | Nuclear receptor modifier (RORA gene) | ArMaDa Phase 1/2 | IVT |
| VOY-101 | Voyager | C3 inhibitor gene therapy | JOURNEY Phase 1/2 | IVT |
| SAR402663 | Sanofi | AAV-anti-VEGF | Phase 1/2 | IVT |
| LX102-C01 | Lees Pharmaceutical | Anti-VEGF gene therapy | Phase 1 — 12-month safety data published 2025 | IVT |
If successful: one injection every 2–5 years vs current 6–12 injections per year
Other Emerging Treatments
| Approach | Drug / Device | Mechanism | Stage |
|---|
| Sustained-release TKI | EYP-1901 (Vorolanib) | Biodegradable intravitreal implant releasing tyrosine kinase inhibitor (anti-VEGF pathway) | Phase 3 LUCIA/LUGANO (2025) |
| Sustained-release TKI implant | OTX-TKI (Axitinib, Ocular Therapeutix) | Biodegradable hydrogel depot in vitreous; anti-VEGFR | Phase 3 (2025) |
| Bispecific novel | AXT107 (AsclepiX) | Peptide blocking VEGFR2 + αvβ3 integrin | Phase 1/2 DISCOVER |
| Stem cell therapy | iPSC-derived RPE cells | Replace diseased RPE in dry AMD | Early clinical trials |
| Oral RPE protection | Tinlarebant (Belite Bio) | RBP4 inhibitor — reduces subretinal accumulation of all-trans-retinol (A2E precursor) | Phase 3 PHOENIX (2025) |
| Photobiomodulation | LumiThera device | 670 nm light → stimulates mitochondrial activity, reduces drusen/inflammation | NCT04065490 Phase 3 |
| Neuroprotection | Elamipretide (Stealth BioTherapeutics) | Mitochondrial-targeted peptide | Phase 3 ReNEW (2025) |
| AI / Digital health | AI-OCT platforms | Automated fluid detection, progression prediction, screening | Entering clinical integration |
12. MONITORING, PROGNOSIS & REHABILITATION
Monitoring Protocol by Disease Stage
| Stage | Frequency | Tools | Action Triggers |
|---|
| Early dry AMD | Annual | Dilated exam + OCT | New symptoms → urgent review |
| Intermediate dry AMD | Every 6 months | OCT + FAF + daily Amsler | Metamorphopsia → same-week assessment |
| Advanced dry (GA) | Every 3–6 months | OCT + FAF (GA area) | Consider complement inhibitor; low vision referral |
| Wet AMD — on treatment | Per T&E protocol (Q4w–Q16w) | OCT + BCVA every visit | Recurrent fluid → shorten interval; non-response → switch drug |
| Fellow eye monitoring | Every 3–6 months | OCT + Amsler | CNV in fellow eye — urgent treatment |
Home Monitoring Tools
| Tool | Description | Advantage |
|---|
| Amsler Grid | 10° central field distortion grid | Free, instant, daily use |
| ForeseeHome (PHP) | Preferential Hyperacuity Perimetry device | FDA-cleared; early CNV detection; telemedicine link |
Prognosis
| Scenario | Prognosis |
|---|
| Dry AMD — early/intermediate | Slow progression; supplements reduce 25% conversion risk |
| Dry AMD — geographic atrophy | Progressive; no cure; complement inhibitors slow growth ~15–22% |
| Wet AMD — untreated | 60–70% lose ≥3 lines of vision within 2 years |
| Wet AMD — with anti-VEGF (current) | ~95% maintain vision; 30–40% gain ≥15 letters (3 lines) |
| Wet AMD — gene therapy (future) | Long-term single-injection control — Phase 3 results awaited |
Predictors of Poor Visual Outcome:
- Late presentation (>6 weeks from symptom onset)
- Large subretinal hemorrhage
- Subfoveal CNV at baseline
- Subretinal fibrosis / disciform scar
- Poor anti-VEGF response after 3 loading doses
Low Vision Rehabilitation
- Optical aids: high-plus reading glasses, hand/stand magnifiers, binoculars for distance
- Electronic aids: video magnifiers (CCTV), e-readers with adjustable font, screen-reading software
- Eccentric fixation training: using peripheral retina for tasks previously done by fovea
- Orientation & mobility: safe navigation, home adaptations
- Psychological support: depression is common with AMD-related vision loss; CBT, peer support
- Legal & social support: registration as visually impaired; DVLA/DMV driving regulations
- Support organizations: Macular Society, AMD Alliance International, Fighting Blindness
📌 KEY TAKE-HOME MESSAGES
| # | Message |
|---|
| 1 | ARMD is the leading cause of blindness in adults >55 — bilateral, progressive, affects central vision only; peripheral vision is preserved |
| 2 | Two forms: Dry (90%, slow, complement-driven drusen/atrophy) and Wet (10%, rapid, VEGF-driven CNV) — dry precedes wet but both may coexist |
| 3 | Pathogenesis: RPE + Bruch membrane + choriocapillaris is the critical unit; CFH/ARMS2 variants + smoking + aging = AMD phenotype |
| 4 | AREDS2 supplements reduce progression by 25% in intermediate AMD — avoid beta-carotene in smokers; lutein/zeaxanthin is the safer alternative |
| 5 | STOP SMOKING — the single most impactful, cost-free intervention; doubles risk if continued |
| 6 | Wet AMD = ophthalmic emergency — urgent anti-VEGF (faricimab or aflibercept 8 mg first-line); treat-and-extend protocol; goal = dry macula on OCT |
| 7 | Geographic atrophy now treatable (2023): Pegcetacoplan (C3 inhibitor) and avacincaptad pegol (C5 inhibitor) — first-ever FDA-approved drugs for dry AMD |
| 8 | Gene therapy is coming — single IVT injection for sustained anti-VEGF production; RGX-314, 4D-150, ADVM-022 all in Phase 3 trials (2025) |
📚 REFERENCES
- Harrison's Principles of Internal Medicine, 22nd Edition (2025, McGraw Hill) — Chapter 391, Sections on Macular Degeneration
- Goldman-Cecil Medicine International Edition — Section 391: Age-Related Macular Degeneration
- Robbins, Cotran & Kumar: Pathologic Basis of Disease — Chapter 29: Retina — Age-Related Macular Degeneration (Figs 29.24, 29.25)
- The Wills Eye Manual, 7th Edition — Sections 11.16 (Dry AMD) & 11.17 (Wet AMD)
- Goodman & Gilman's Pharmacological Basis of Therapeutics — Chapter 74: Ocular Pharmacology, Table 74-15
- Katzung's Basic & Clinical Pharmacology, 16th Edition — Macular Degeneration (Block 12)
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina) — Chapter 24, Clinical Correlation ARMD
- Thompson & Thompson Genetics and Genomics in Medicine, 9th Ed — GWAS in AMD
- AREDS Research Group (2001). Arch Ophthalmol. Original supplement trial
- AREDS2 Research Group (2013). JAMA. Lutein/zeaxanthin substitution
- Kalavar M, Sridhar J. Clinical trials examining faricimab and high-dose aflibercept for wet AMD. Curr Opin Ophthalmol 2025. PMID: 39937692
- Marchesi N et al. Different Therapeutic Approaches for Dry and Wet AMD. Int J Mol Sci 2024. PMID: 39684764
- Rowe LW, Ciulla TA. Gene Therapy for Non-Hereditary Retinal Disease. Genes (Basel) 2024. PMID: 38927656
- Wheeler S et al. Treatment for dry AMD: where we stand in 2024. Curr Opin Ophthalmol 2024. PMID: 38869976
- Clinical Trial Update May 2025. Retinal Physician — faricimab CONSTANCE, 4D-150 4FRONT, VERDANT, PHOENIX trials
End of ARMD Comprehensive Review — Orris Medical Education, June 2026