Teach me screening chapter from parks everything every topics in the book i need to learn understand and memorise
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need from Park's screening chapter. Let me compile a complete, structured teaching guide.
📚 Park's Screening Chapter - Complete Study Guide
(Park's Textbook of Preventive and Social Medicine)
1. CONCEPT OF SCREENING
Definition (memorise this verbatim):
"The search for unrecognized disease or defect by means of rapidly applied tests, examinations or other procedures in apparently healthy individuals."
Background - Iceberg Phenomenon:
The submerged part of the iceberg = hidden mass of disease (sub-clinical cases, carriers, undiagnosed cases). The floating tip = what the physician sees in practice. Screening targets the hidden part.
Why screening was developed:
- Annual health exams were too costly and time-consuming for large populations
- Screening conserves physician-time - technicians administer tests, physician only interprets
- Original programmes: TB, syphilis, antenatal mothers, school children, occupational groups
How screening differs from periodic health examination:
- Capable of wide application
- Relatively inexpensive
- Requires little physician-time (physician not needed to administer - only to interpret)
2. SCREENING vs. DIAGNOSTIC TESTS (Table - Very Exam Important)
| Screening Test | Diagnostic Test |
|---|---|
| Done on apparently healthy | Done on sick / those with indications |
| Applied to groups | Applied to single patients |
| Test results are arbitrary and final | Diagnosis modified by new evidence |
| Based on one criterion/cut-off point | Based on multiple symptoms, signs, labs |
| Less accurate | More accurate |
| Less expensive | More expensive |
| Not a basis for treatment | Used as basis for treatment |
| Initiative from investigator/agency | Initiative from patient with a complaint |
Note: The same test can sometimes be used for both screening AND diagnosis (e.g., VDRL for syphilis).
3. CASE-FINDING (Important distinction)
Definition: "The application of a diagnostic test, or a group of tests, to apparently healthy individuals who are consulting a physician for some other purpose."
Also called opportunistic screening - physician uses the patient's visit for another reason to screen them.
Examples: Random blood sugar check while patient is being treated for hypertension; urine test for proteinuria during a routine visit.
4. USES OF SCREENING (4 main uses)
a. Case Detection (Prescriptive Screening)
- Presumptive identification of unrecognized disease
- Does NOT arise from a patient's request
- People screened primarily for their own benefit
- Examples: neonatal screening, bacteriuria in pregnancy, breast cancer, cervical cancer, PKU, pulmonary TB, haemolytic disease of newborn
b. Control of Disease (Prospective Screening)
- People examined for the benefit of others
- Examples: screening immigrants for TB and syphilis to protect the home population; screening for streptococcal infection to prevent rheumatic fever
- Can reduce spread of infectious disease and/or mortality
c. Research Purposes
- To study the natural history of diseases whose course is not fully known (e.g., cancer, hypertension)
- Initial screening = prevalence estimate
- Subsequent screening = incidence figure
- Investigator has ethical obligation to treat those found positive
d. Syndromic Surveillance
- Screening populations to detect disease outbreaks early (e.g., influenza-like illness trends)
5. TYPES OF SCREENING (Very Important for MCQs)
a. Mass Screening
- Screening of whole population regardless of risk
- Example: Universal newborn screening for PKU/hypothyroidism
- Advantage: No one is missed
- Disadvantage: Expensive, many low-risk individuals screened unnecessarily
b. Selective / High-Risk Screening
- Screening only the high-risk group (a subgroup of the population)
- More cost-effective than mass screening
- Example: Screening only smokers for lung cancer; screening only hypertensives for target organ damage
- Also called "targeted screening"
c. Multiphasic Screening
- Application of two or more screening tests simultaneously to a large population
- Example: Measuring BP + blood glucose + cholesterol + vision in a single visit
- Advantage: More diseases detected in one contact; cost-effective per person
- Used extensively in health camps and industrial health programmes
6. CRITERIA FOR SCREENING (Wilson & Jungner Criteria - Most Important)
A disease/condition is suitable for screening if:
- The condition sought should be an important health problem (significant morbidity/mortality)
- There should be an accepted treatment for patients with recognized disease
- Facilities for diagnosis and treatment should be available
- There should be a recognizable latent or early symptomatic stage
- A suitable test or examination should be available - acceptable to the population
- The natural history of the condition should be adequately understood
- There should be an agreed policy on whom to treat as patients
- The cost of case-finding (including diagnosis and treatment) should be economically balanced in relation to possible expenditure on medical care as a whole
- Case-finding should be a continuing process and not a "once and for all" project
Memory trick: IACTNACS (Important, Accepted treatment, Cost, Treatment facilities, Natural history, Agreed policy, Continuing process, Suitable test)
7. VALIDITY OF SCREENING TESTS
Validity: The ability of a test to distinguish those who HAVE the disease from those who DO NOT.
Three components: Sensitivity, Specificity, Predictive Value
The 2×2 Table (Must memorise)
DISEASE
Present Absent
TEST Positive a b (a+b)
Negative c d (c+d)
(a+c) (b+d) Total
- a = True Positives (TP)
- b = False Positives (FP)
- c = False Negatives (FN)
- d = True Negatives (TN)
Sensitivity
"The ability of a test to correctly identify those WHO HAVE the disease."
Formula: a / (a+c) × 100
- Sensitivity = TP / (TP + FN) × 100
- A highly sensitive test has few False Negatives
- Used when missing a case is dangerous (e.g., HIV, TB, cancer)
- "Snout" mnemonic: SnNout - Sensitive test, Negative result rules OUT disease
Specificity
"The ability of a test to correctly identify those WHO DO NOT have the disease."
Formula: d / (b+d) × 100
- Specificity = TN / (TN + FP) × 100
- A highly specific test has few False Positives
- Used when a false positive causes harm (e.g., unnecessary surgery, stigma)
- "Spin" mnemonic: SpPin - Specific test, Positive result rules IN disease
Key Trade-off
- Sensitivity and specificity are inversely related
- Raising the cut-off point → ↑ Specificity, ↓ Sensitivity
- Lowering the cut-off point → ↑ Sensitivity, ↓ Specificity
8. PREDICTIVE VALUE (Very High-Yield)
Positive Predictive Value (PPV)
"The probability that a person who tests positive ACTUALLY HAS the disease."
Formula: a / (a+b) × 100 = TP / (TP + FP)
Negative Predictive Value (NPV)
"The probability that a person who tests negative ACTUALLY DOES NOT HAVE the disease."
Formula: d / (c+d) × 100 = TN / (FN + TN)
Effect of Prevalence on Predictive Value
This is a VERY important concept:
- When prevalence is HIGH → PPV increases, NPV decreases
- When prevalence is LOW → PPV decreases (many false positives), NPV increases
- Same test in a high-prevalence population has a higher PPV than in a low-prevalence population
Clinical implication: A screening test that works well in a high-risk population may give mostly false positives if applied to the general low-risk population. This is why selective/targeted screening is often preferred.
9. RELIABILITY (REPRODUCIBILITY / PRECISION)
Definition: The ability of a test to give consistent results on repeated trials under the same conditions.
A test can be reliable but not valid (consistently wrong).
A test cannot be valid but not reliable (if valid, it must also be reliable).
Sources of variation reducing reliability:
A. Observer variation
- Intra-observer variation: Same observer gets different results on repeat measurement
- Inter-observer variation: Two different observers get different results
- Occurs in: reading X-rays, interpreting cervical smears, auscultation of BP
- Minimized by: standardization of procedures, intensive training, using ≥2 independent observers
B. Biological (subject) variation
- Changes in the parameter itself: e.g., cervical smear may be normal one day, abnormal another; BP varies through the day
- Variation in how patients perceive/answer: recall errors, deliberate concealment
- Regression to the mean: Extreme values tend to move toward the average on re-measurement. Important when evaluating drug therapy (e.g., antihypertensives) - improvement may be partly regression to mean, not true drug effect
C. Technical method errors
- Defective instruments, erroneous calibration, faulty reagents
- Test itself may be inappropriate or unreliable
10. DISTRIBUTION OF VARIABLES - The Cut-Off Point
Bimodal Distribution
- Two separate curves: one for "normal" population, one for "diseased"
- Clear separation with a "borderline" zone where the curves overlap
- Cut-off point set at point E (where distributions intersect) minimizes both false positives and false negatives
- Example: Phenylketonuria (PKU)

Unimodal Distribution
- Single continuous curve (e.g., blood pressure, blood sugar, serum cholesterol)
- No sharp dividing line between normal and diseased
- Cut-off point is arbitrary
- Cutting at level C/A (lower) → Higher sensitivity, more false positives
- Cutting at level D/B (higher) → Higher specificity, more false negatives
- Example: Diabetes (blood glucose cut-off)
11. EVALUATION OF SCREENING PROGRAMMES
A screening programme should be evaluated for:
- Yield - number of new cases detected in the screened population
- Sensitivity and Specificity of the test used
- Predictive value in the target population
- Cost-effectiveness - cost per case detected
- Compliance - uptake rate in the target population
- Follow-up - proportion of screen-positives who receive definitive diagnosis and treatment
- Impact - reduction in morbidity/mortality in the screened group vs. unscreened
Factors affecting yield:
- Prevalence of unrecognized disease in the population
- Sensitivity of the test
- Number of persons tested
12. BIAS IN SCREENING (High-Yield Exam Topic)
Lead Time Bias
- Screening detects disease earlier in its natural history
- Survival appears longer from diagnosis - but this is just because diagnosis was moved earlier, not because the patient actually lived longer
- This can make a screening programme appear effective when it is not
Length Bias
- Screening tends to detect slower-progressing (less aggressive) cases, because they spend more time in the detectable pre-clinical phase
- Rapidly progressive (aggressive) cases pass through the detectable phase quickly and are missed
- Result: Screened cases appear to have better outcomes than unscreened cases, even if screening has no real benefit
Selection Bias (Volunteer Bias)
- People who participate in screening tend to be more health-conscious, and thus have better outcomes regardless of screening
- Makes screening appear more effective than it is
13. SOME SPECIFIC SCREENING TESTS (from Table 8 in Park's)
| Disease | Screening Test |
|---|---|
| Tuberculosis | Tuberculin test, Chest X-ray, sputum smear |
| Hypertension | BP measurement |
| Diabetes mellitus | Urine glucose (glycosuria), Random/Fasting blood glucose, OGTT |
| Cervical cancer | Pap smear (Papanicolaou smear) |
| Breast cancer | Self-examination, clinical breast exam, mammography |
| PKU | Guthrie test (blood phenylalanine) |
| Hypothyroidism | TSH (heel-prick blood spot) |
| Anaemia | Haemoglobin / PCV |
| Syphilis | VDRL |
| Gonorrhoea | Endocervical culture |
| Glaucoma | Tonometry |
| Deafness | Audiometry |
| Visual defects | Snellen chart |
| Neural tube defects (prenatal) | Maternal serum AFP |
14. CANCER SCREENING (from Park's block 6)
Key principles:
- Cancer screening is most useful when a detectable pre-clinical phase exists
- Must have an effective treatment that improves outcomes when applied early
- Most evidence-based cancer screening programmes:
- Cervical cancer: Pap smear (every 3 years from age 21, or HPV co-testing every 5 years)
- Breast cancer: Mammography (annual/biennial from age 40-50 depending on guideline)
- Colorectal cancer: Faecal occult blood test (FOBT), colonoscopy
- Oral cancer: Visual inspection with naked eye / acetic acid (VIA)
15. NEONATAL SCREENING
Purpose: Detect inborn errors of metabolism before symptoms appear, when treatment can prevent disability.
Conditions screened (Indian national programme):
- Congenital hypothyroidism (CHT) - most common
- Phenylketonuria (PKU)
- G6PD deficiency
- Congenital adrenal hyperplasia (CAH)
- Sickle cell disease
Method: Heel-prick blood spot on filter paper (Guthrie card) collected at 48-72 hours after birth.
Treatment:
- CHT: Thyroxine supplementation (prevents cretinism)
- PKU: Phenylalanine-restricted diet (prevents intellectual disability)
QUICK REVISION FLASHCARDS
Q: Define screening.
A: Search for unrecognized disease/defect by rapidly applied tests in apparently healthy individuals.
Q: What are the 3 types of screening?
A: Mass (whole population), Selective/High-risk (targeted group), Multiphasic (multiple tests simultaneously).
Q: Sensitivity formula?
A: TP / (TP + FN) × 100. It identifies TRUE POSITIVES correctly.
Q: Specificity formula?
A: TN / (TN + FP) × 100. It identifies TRUE NEGATIVES correctly.
Q: Sensitive test negative → ?
A: Rules OUT disease (SnNout).
Q: Specific test positive → ?
A: Rules IN disease (SpPin).
Q: When prevalence rises, what happens to PPV?
A: PPV rises. NPV falls.
Q: What is lead-time bias?
A: Earlier diagnosis appears to prolong survival but the patient doesn't actually live longer - just diagnosed earlier.
Q: What is multiphasic screening?
A: Two or more screening tests applied simultaneously to a large population.
Q: What is regression to the mean?
A: Extreme values tend to move toward the average on repeat measurements - important to remember when evaluating therapy effectiveness.
Q: Prospective vs. Prescriptive screening?
A: Prospective = for benefit of others (e.g., screening immigrants for TB). Prescriptive = for benefit of the individual (e.g., neonatal screening).
Q: Wilson & Jungner - how many criteria?
A: 9 criteria. Key ones: important health problem, accepted treatment available, recognizable latent stage, suitable/acceptable test, facilities available, cost balanced, continuing process.
HIGH-YIELD MCQ TRAPS
- Screening is not a diagnostic test - screen positives need further workup
- A highly sensitive test is preferred for serious diseases where missing a case is dangerous
- A highly specific test is preferred where a false positive causes harm (unnecessary surgery, stigma)
- Reliability ≠ Validity - a test can be reliable (reproducible) but invalid (consistently wrong)
- PPV depends heavily on prevalence - the same test has a lower PPV in low-prevalence settings
- Multiphasic screening is the most cost-effective strategy per person screened
- The Guthrie test is the screening test for PKU
- Pap smear is the screening test for cervical cancer (not diagnosis)
- Lead time bias overestimates benefit of screening by shifting apparent survival without real benefit
- In bimodal distribution, cut-off at intersection point (E) minimizes misclassification
This covers every topic in the screening chapter of Park's - from the concept, through types and criteria, to validity/reliability statistics, bias, specific programme tests, neonatal screening, and cancer screening. Focus especially on the 2×2 table formulas (sensitivity, specificity, PPV, NPV), the Wilson & Jungner criteria, and the three types of bias - these are the highest-yield exam areas.
Concept of health and disease
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the chapter. Let me compile the full teaching guide.
📚 Park's Chapter 2: Concept of Health and Disease - Complete Study Guide
"Health is NOT mainly an issue of doctors, social services and hospitals. It is an issue of social justice."
PART A: CONCEPT OF HEALTH
1. CHANGING CONCEPTS OF HEALTH
Health has evolved from an individual concern to a worldwide social goal. Four major conceptual models:
1. Biomedical Concept
- Oldest and most traditional view: "health = absence of disease"
- Basis: Germ theory of disease (dominated early 20th century)
- Viewed the body as a machine, disease = machine breakdown, doctor = mechanic
- Criticism: Ignores environmental, social, psychological, cultural determinants
- Failed to solve problems like malnutrition, chronic disease, drug abuse, mental illness, pollution
2. Ecological Concept
- Health = dynamic equilibrium between man and his environment
- Disease = maladjustment of the human organism to environment
- Dubos' definition: "Health implies the relative absence of pain and discomfort and a continuous adaptation and adjustment to the environment to ensure optimal function"
- Raises two issues: imperfect man and imperfect environment
- Improvement in human adaptation to natural environments can lead to longer life, even without modern health services
3. Psychosocial Concept
- Health is NOT only a biomedical phenomenon
- Influenced by social, psychological, cultural, economic, and political factors
- Health is both a biological AND social phenomenon
4. Holistic Concept (Current - most comprehensive)
- Synthesis of all three above concepts
- Recognizes strength of social, economic, political, environmental influences
- Health = unified/multidimensional process involving well-being of the whole person in the context of their environment
- Corresponds to the ancient view: "sound mind, in a sound body, in a sound family, in a sound environment"
- All sectors of society have an effect on health
2. WHO DEFINITION OF HEALTH (Must memorise verbatim)
"Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity."
- Adopted in the Preamble to the Constitution of WHO (1948)
- Three dimensions: Physical + Mental + Social
- Later, a 4th dimension was proposed: Spiritual health
- Some also add: Vocational health
Criticism of WHO definition:
- The word "complete" is unrealistic - no one can be in complete health all the time
- It is not measurable (no objective criteria)
- It is static - doesn't account for dynamic nature of health
- Ignores economic and political dimensions
3. DIMENSIONS OF HEALTH
| Dimension | Description |
|---|---|
| Physical | Functioning of body at cellular/organ level; absence of disease |
| Mental | Ability to think clearly, feel comfortable, behave appropriately |
| Social | Ability to make and maintain relationships; fulfil social roles |
| Spiritual | Personal beliefs, purpose, meaning in life |
| Vocational | Ability to perform work productively |
| Emotional | Ability to express emotions appropriately |
4. POSITIVE HEALTH vs NEGATIVE HEALTH
| Positive Health | Negative Health |
|---|---|
| Perfect functioning of body and mind | Presence of disease |
| Biologically: every cell/organ at optimum capacity | Morbidity, disability |
| Psychologically: sense of perfect well-being and mastery | Death |
| Socially: optimal capacity for participation in social system | - |
Dubos' caution: "The concept of perfect positive health cannot become a reality because man will never be so perfectly adapted to his environment that his life will not involve struggles, failures and sufferings."
→ Positive health is a mirage - always something to strive for, never fully achieved.
5. HEALTH AS A RELATIVE CONCEPT
- Health is NOT universal - it is culturally, geographically, and socio-economically relative
- A newborn in India weighs 2.8 kg on average vs 3.5 kg in developed countries - yet both are healthy in their context
- Height/weight standards vary between countries and socio-economic groups
- Many "normal" people have heart murmurs, enlarged tonsils, X-ray shadows yet show no ill health
- Implication: Each country should define its own norms based on prevailing ecological conditions, rather than universal health standards
6. HEALTH AS A HUMAN RIGHT
Key milestones (important for exam):
- 1946: WHO Constitution - health as a fundamental human right
- 1977: 30th World Health Assembly - "Health for All by 2000" (HFA 2000)
- 1978: Alma-Ata Declaration on Primary Health Care
- 1979: UN adopted health as integral part of socio-economic development
- 1986: Ottawa Charter for Health Promotion
- 2000: Millennium Development Goals (MDGs) - health centrally positioned
- 2015: Sustainable Development Goals (SDGs) - 2030 Agenda
- Right to health recognized in at least 115 countries' constitutions
7. DETERMINANTS OF HEALTH
Health is multifactorial - lies both within the individual and in society.
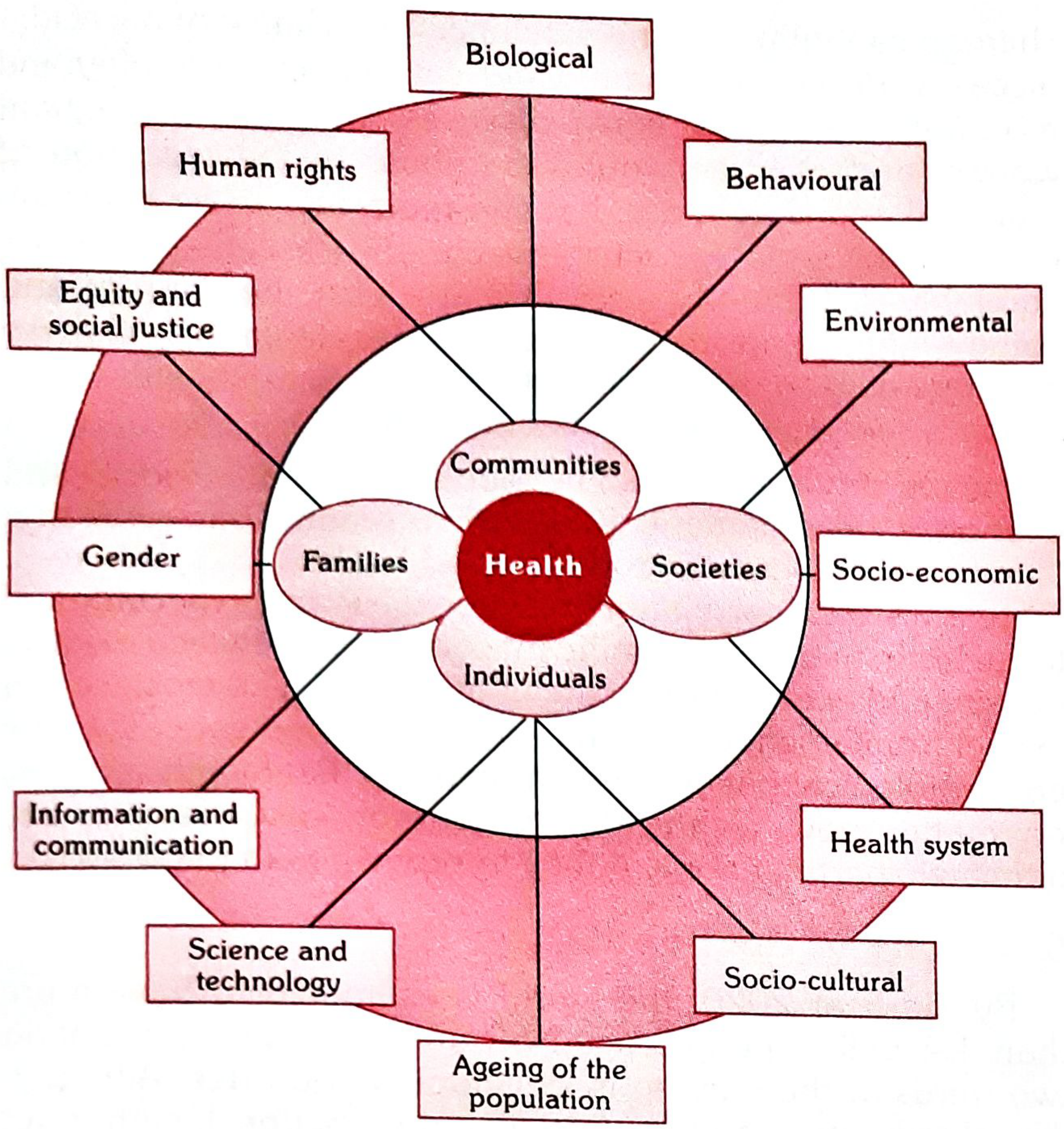
1. Biological Determinants
- Genetic make-up at conception (cannot be altered after)
- Chromosomal anomalies, errors of metabolism, mental retardation, some types of diabetes
- Role of medical genetics: genetic screening, gene therapy
2. Behavioural and Socio-cultural Determinants
- Lifestyle, habits, customs, behaviours (smoking, diet, exercise, substance use)
- Social norms, cultural practices, education level
- Lifestyle diseases now dominate: obesity, CVD, type 2 DM, lung cancer
3. Environment
- Physical: climate, housing, water, sanitation
- Social: social support networks, social cohesion
- Biological: microorganisms in the environment
- All diseases reflect, to some degree, failure of the organism to successfully adapt to the environment
4. Socio-economic Conditions
- Poverty is the single most important determinant of ill-health
- Education, occupation, income strongly correlate with health outcomes
- Social class gradients in health are seen globally
5. Health Services
- Availability, accessibility, affordability, acceptability
- Quality and coverage of preventive, promotive, curative services
6. Ageing of Population
- Changing demographic structure brings shift in disease pattern
- Rise of non-communicable diseases, degenerative conditions
8. RESPONSIBILITY FOR HEALTH
Three levels:
1. Individual responsibility (Self-care)
- Health is primarily an individual responsibility - cannot be given by others
- Self-care definition: "Health activities including promotion, maintenance, treatment care and health-related decision making, carried out by individuals and families"
- Includes: diet, sleep, exercise, weight control, avoiding tobacco/alcohol/drugs, personal hygiene, immunization, early reporting when sick, family planning
2. Community responsibility
- Things individuals cannot achieve alone - achieved through collective action
- Community involvement in health planning, resource mobilization, implementing programmes
- Social support systems, group behaviours
3. State responsibility
- Create conditions for health through legislation, policy, resource allocation
- Health system governance, social protection, sanitation laws
PART B: CONCEPT OF DISEASE
1. DEFINITIONS OF DISEASE
- Webster: "A condition in which body health is impaired, a departure from a state of health, an alteration of the human body interrupting the performance of vital functions"
- Oxford: "A condition of the body in which its functions are disrupted or deranged"
- Ecological: "A maladjustment of the human organism to the environment"
- Simple: Disease = opposite of health = any deviation from normal functioning
WHO has defined health but NOT disease. Why? Because disease has many shades - the "spectrum of disease" from inapparent (subclinical) to severe manifest illness.
2. DISEASE vs. ILLNESS vs. SICKNESS (Susser's Distinction - Very Exam Important)
| Term | Literal meaning | Definition |
|---|---|---|
| Disease | "Without ease" | Physiological/psychological dysfunction |
| Illness | - | Subjective state - individual's perception and behaviour in response to disease; impact on psychosocial environment |
| Sickness | - | State of social dysfunction - a role the individual assumes when ill ("sickness role") |
Key points:
- You can have disease without feeling ill (e.g., asymptomatic hypertension, subclinical diabetes)
- You can be ill without physical impairment (e.g., hypochondria, psychosomatic illness)
- The clinician sees people who are ill - not the disease - which he must diagnose and treat
3. CONCEPT OF CAUSATION OF DISEASE
Old Theories (Pre-Pasteur)
- Supernatural theory
- Theory of humors (body fluids out of balance - shared by ancient Indians and Greeks)
- Concept of contagion
- Miasmatic theory (bad air causes disease)
- Theory of spontaneous generation
Germ Theory of Disease (Pasteur era, 19th century)
- A single microbe causes a specific disease (one-to-one relationship)
- Disease model: Disease agent → Man → Disease
- Limitation: Not everyone exposed to TB develops TB; exposure + susceptibility (host factors) both matter
- Modern medicine has moved AWAY from strict germ theory
Epidemiological Triad (Agent-Host-Environment)
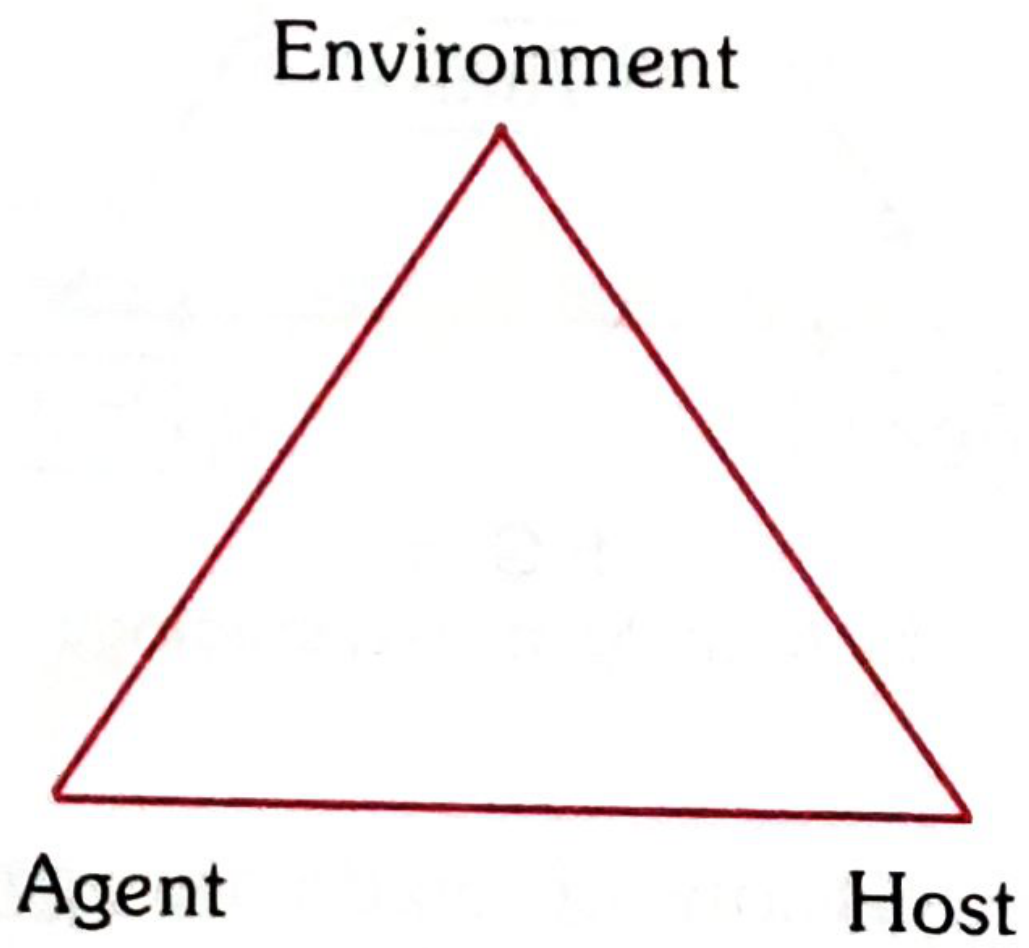
The model recognizes three interacting components:
AGENT - the cause of disease
HOST - the organism that harbors the disease
ENVIRONMENT - surroundings external to the host that allow/cause disease
Time is also a fourth factor - accounts for incubation periods, duration of exposure, latency.
4. AGENTS OF DISEASE (Classification)
1. Biological agents
- Bacteria, viruses, fungi, parasites, rickettsia, prions
2. Nutritional agents
- Protein-energy malnutrition (PEM), anaemia, goitre, obesity, vitamin deficiencies
3. Physical agents
- Excessive heat, cold, humidity, pressure, radiation, electricity, sound
4. Chemical agents
- Endogenous: Produced in body due to dysfunction - urea (uraemia), serum bilirubin (jaundice), ketones (ketosis), uric acid (gout), calcium carbonate (kidney stones)
- Exogenous: Allergens, metals, fumes, dust, gases, insecticides - acquired by inhalation, ingestion, or inoculation
5. Mechanical agents
- Chronic friction and mechanical forces causing crushing, tearing, sprains, dislocations, death
6. Absence/excess of a necessary factor
- Chemical: hormones (insulin, oestrogens), enzymes
- Structural: absence of thymus, cardiac defects
- Chromosomal: Mongolism (Down syndrome), Turner's syndrome
- Immunological: agammaglobulinaemia
7. Social agents
- Poverty, smoking, drug/alcohol abuse, unhealthy lifestyles, social isolation, maternal deprivation
- Modern concept of "agent" is very broad - includes both living and non-living agents
5. HOST FACTORS (Intrinsic)
In epidemiology: host = "soil", agent = "seed"
- (i) Demographic: Age, sex, ethnicity
- (ii) Biological: Genetic factors, biochemical blood levels (cholesterol), blood groups, enzymes, immunological factors, physiological function (BP, FEV)
- (iii) Social/economic: Socio-economic status, education, occupation, stress
- (iv) Lifestyle: Diet, exercise, smoking, alcohol, drug use
6. ENVIRONMENTAL FACTORS
- Physical: Climate, geography, housing, water supply, sanitation
- Biological: Flora, fauna, vectors, reservoirs of infection
- Social: Overcrowding, population density, social norms, cultural practices
- Economic: Poverty, income inequality, employment
7. SPECTRUM OF DISEASE
The term "spectrum of disease" is a graphic representation of variations in manifestations of disease - like the spectrum of light, where colours vary from end to end with no sharp borders.
| End of spectrum | Manifestation |
|---|---|
| One end | Subclinical (inapparent) infections |
| Middle | Mild to moderate to severe illness |
| Other end | Fatal illness |
- Different manifestations reflect individuals' different states of immunity and receptivity
- In infectious diseases, also called "gradient of infection"
- Leprosy is the classic example of a spectral disease
- Exception: Rabies - almost always fatal (no spectrum of severity)
- The spectrum can be interrupted at any point by early diagnosis, treatment, or preventive measures
8. ICEBERG OF DISEASE (Closely related to Spectrum)
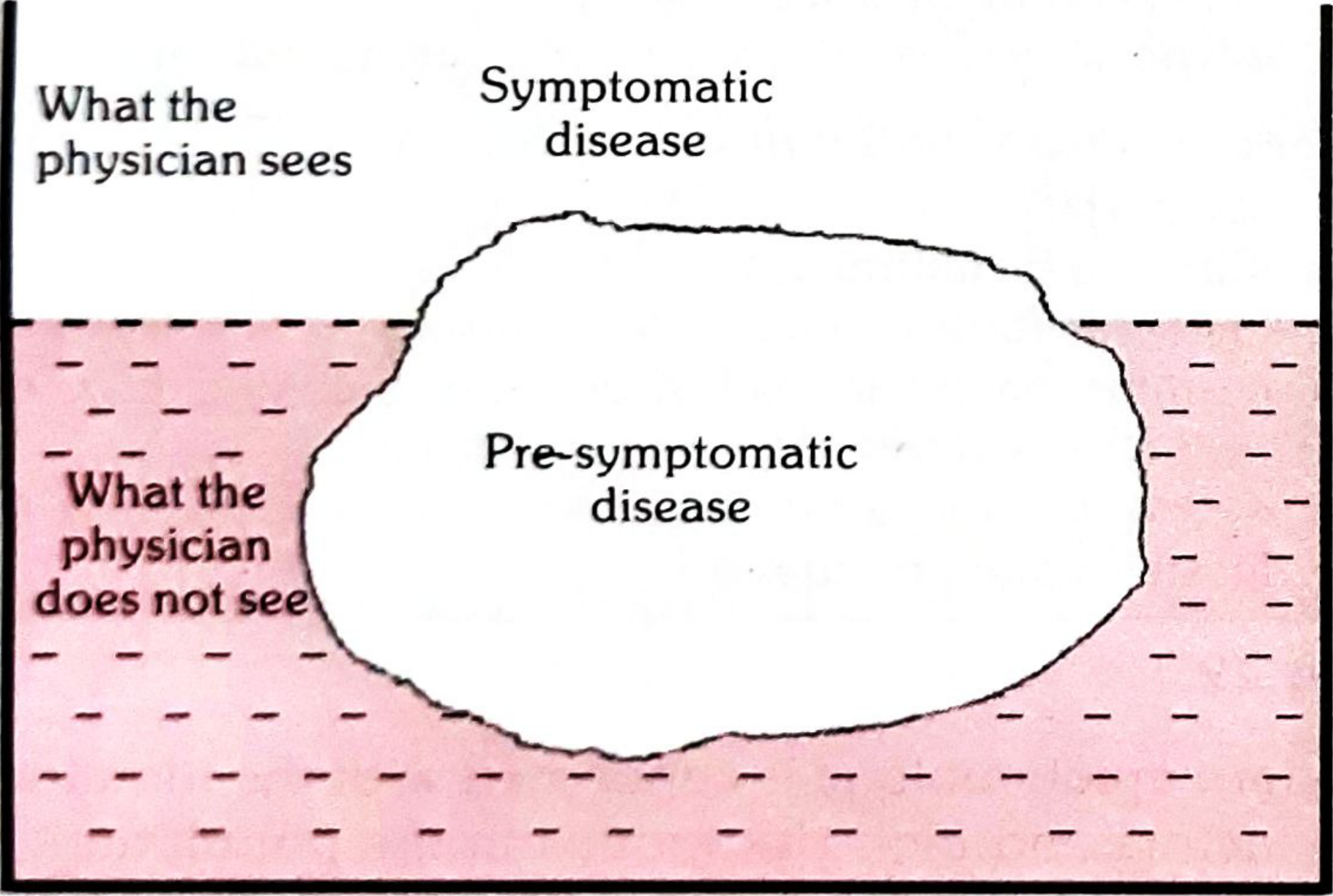
- Floating tip (above waterline) = Clinical cases - what the physician sees
- Submerged portion (below waterline) = Hidden mass of disease: latent, inapparent, presymptomatic, undiagnosed cases, and carriers
- Waterline = Demarcation between apparent and inapparent disease
Examples with massive submerged portion:
- Hypertension, diabetes, anaemia, malnutrition, mental illness
Significance: The hidden portion = undiagnosed reservoir of infection/disease in the community. Detecting and controlling it is the challenge of preventive medicine. This is why screening is so important (links directly to Chapter 8).
9. CONCEPT OF RISK (Risk Factors and At-Risk Groups)
Risk factor: An attribute or exposure that is significantly associated with the development of a disease.
Risk approach: Directing resources to those most at risk - "something for all, but more for those in need - in proportion to the need."
At-risk groups (WHO guidelines):
a. Biological:
- Age groups (infants, toddlers, elderly)
- Sex (females in reproductive age)
- Physiological state (pregnancy, high cholesterol, high BP)
- Genetic factors (family history)
- Existing disease/unhealthy behaviour
b. Physical:
- Rural/urban slums
- Overcrowding, poor living conditions
- Proximity to industries, poor water supply
c. Sociocultural:
- Low social class
- Ethnic/cultural group
- Family disruption, poor education, poor housing
- Smoking, lack of exercise, overeating, drug addiction
- Poor access to health services
PART C: INDICATORS OF HEALTH (Measurement of Health)
Since no single indicator can measure health, a profile of indicators is used:
- Mortality indicators
- Morbidity indicators
- Disability rates
- Nutritional status indicators
- Health care delivery indicators
- Utilization rates
- Indicators of social and mental health
- Environmental indicators
- Socio-economic indicators
- Health policy indicators
- Indicators of quality of life
- Other indicators
Requirements of a good health indicator:
- Valid - measures what it is supposed to measure
- Reliable and objective - same answer regardless of who measures
- Sensitive - picks up changes in the situation
- Specific - reflects changes only in that specific situation
- Feasible - data can actually be obtained
- Relevant - contributes to understanding the phenomenon
Problem with measuring health: Health, like happiness, cannot be defined in exact measurable terms. No existing definition (including WHO) contains criteria for measurement. We end up measuring illness (the antithesis of health) - morbidity, disability, death.
QUICK REVISION FLASHCARDS
Q: WHO definition of health?
A: "A state of complete physical, mental and social well-being and not merely the absence of disease or infirmity." (1948)
Q: Four changing concepts of health in order?
A: Biomedical → Ecological → Psychosocial → Holistic
Q: Dubos' definition (Ecological concept)?
A: "Health implies the relative absence of pain and discomfort and a continuous adaptation and adjustment to the environment to ensure optimal function."
Q: Difference between disease, illness, and sickness (Susser)?
A: Disease = physiological/psychological dysfunction. Illness = subjective feeling of being unwell. Sickness = social dysfunction (sick role).
Q: What is the Epidemiological Triad?
A: Agent + Host + Environment (+ Time). Replaced the one-to-one germ theory.
Q: What is the waterline in the Iceberg of Disease?
A: Demarcation between apparent (clinical) disease and inapparent (subclinical, undiagnosed) disease.
Q: Classic example of spectrum of disease?
A: Leprosy. Disease with no spectrum (almost always fatal)? Rabies.
Q: What is the gradient of infection?
A: Spectrum of disease applied to infectious diseases.
Q: Social agents of disease?
A: Poverty, smoking, drug/alcohol abuse, unhealthy lifestyles, social isolation, maternal deprivation.
Q: What is self-care?
A: "Health activities including promotion, maintenance, treatment care and health-related decision making, carried out by individuals and families."
Q: Health for All - target year?
A: "Health for All by the year 2000" - declared by 30th World Health Assembly (1977).
Q: Why can't WHO define disease?
A: Disease has many shades (spectrum) - from subclinical to fatal; same organism can cause different manifestations; same disease can be caused by different organisms; no sharp border between normal and abnormal.
Q: What is positive health?
A: Perfect functioning of body (every cell/organ at optimum capacity), mind (sense of well-being and mastery), and social function (optimal capacity for social participation). Dubos said it always remains a mirage.
HIGH-YIELD MCQ TRAPS
- WHO defined health in 1948 in the Preamble to its Constitution - but has NOT defined disease
- The holistic concept is the synthesis of all three other concepts - not just biomedical
- Dubos gave the ecological concept definition - remember his name
- Germ theory = one-to-one (agent → disease). Epidemiological triad = multifactorial
- Disease = physiological dysfunction; Illness = subjective; Sickness = social dysfunction
- Rabies is the exception to the spectrum of disease (almost no mild cases)
- Floating tip of iceberg = clinical cases (visible to physician); submerged = hidden mass
- Leprosy = best example of spectrum (from tuberculoid to lepromatous)
- Regression to the mean - extreme values move toward average on re-measurement (trap in evaluating drug therapy)
- The waterline in the iceberg = the cut-off between apparent and inapparent disease
- Positive health - Dubos said it is always a mirage (not achievable in reality)
- Self-care = activities by individuals and families WITHOUT professional assistance
- The right to health is recognized in at least 115 countries' constitutions
This is a shared conversation. Sign in to Orris to start your own chat.