Heimlich maneuover
Reading File
Finding Sources
Finding Sources
Searching Images
Heimlich maneuver abdominal thrust choking
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of the Heimlich maneuver based on authoritative emergency medicine textbooks.
Heimlich Maneuver (Abdominal Thrust Maneuver)
Mechanism
The Heimlich maneuver creates an artificial cough by forcefully elevating the diaphragm and expelling air from the lungs, generating enough intrathoracic pressure to dislodge a foreign body obstructing the airway. It is most effective when a solid food bolus is obstructing the larynx.
— Tintinalli's Emergency Medicine, p. 189
Technique
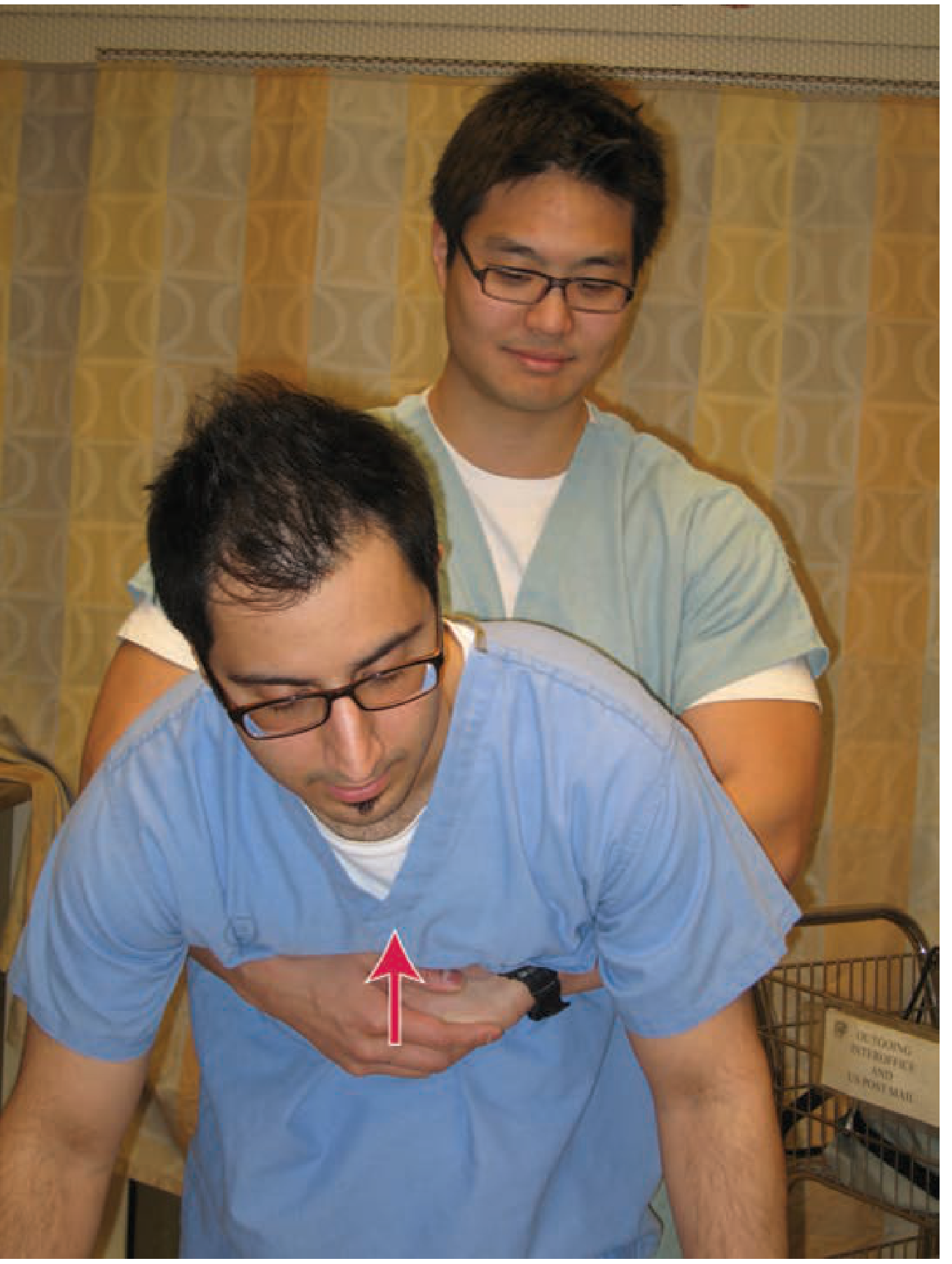
Conscious Patient (Standing or Sitting)
- Stand behind the patient.
- Place the thumb side of a clenched fist against the victim's abdomen — midline, just above the umbilicus, well below the xiphoid process.
- Grasp the fist with the other hand.
- Deliver a forceful, quick inward and upward thrust.
- Repeat until the object is expelled or the patient loses consciousness.
Unconscious Patient (Supine)
- Place the victim supine on a firm surface.
- Kneel astride or beside the victim's thighs.
- Place the heel of the dominant hand midline, just above the umbilicus.
- Place the other hand on top.
- Deliver quick upward thrusts.
Self-Administration
The individual can use their own fist, or lean forcibly against a firm object (e.g., a chair back or porch railing).
Special Populations
| Situation | Modification |
|---|---|
| Morbid obesity / Late pregnancy | Use chest thrusts instead — place fist on sternum, avoiding costal margins and xiphoid |
| Infants | Back blows (head-down position) + chest thrusts — abdominal thrusts are not recommended due to higher risk of iatrogenic visceral injury |
| Unconscious patient | Transition to chest compressions (CPR) — these generate similar or higher peak airway pressures; perform 30 compressions, attempt 2 breaths, and remove the object if visualized |
When to Intervene
Act immediately when a patient:
- Makes the universal choking sign (clutching the neck)
- Becomes cyanotic
- Is unable to cough or speak effectively
- Becomes unconscious
Do not intervene if the patient is coughing forcefully — an effective cough generates more expulsive force than any manual thrust.
Airway Clearance Evidence
The International Consensus Conference on CPR and Emergency Cardiovascular Care found good evidence for chest thrusts, abdominal thrusts, and back blows — but insufficient evidence to determine which is superior. In practice, more than one technique is often required, so they should be applied in rapid sequence until obstruction is relieved.
— Roberts and Hedges' Clinical Procedures in Emergency Medicine
Key point: After 30 chest compressions in an unconscious patient, open the airway, look for the foreign body, remove it only if directly visualized, attempt 2 rescue breaths, then continue CPR. Never perform blind finger sweeps.
Potential Complications
- Rupture or injury of abdominal/thoracic viscera
- Stomach rupture
- Esophageal perforation
- Mesenteric laceration
- Regurgitation of gastric contents
These risks must be weighed against the immediate life threat — a complete airway obstruction is rapidly fatal without intervention.
Sources: Tintinalli's Emergency Medicine, p. 189 | Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 85–86
This is a shared conversation. Sign in to Orris to start your own chat.