What is idiosyncrasy and immunity
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive information from multiple authoritative textbooks. Here is a thorough answer:
Idiosyncrasy and Immunity
1. Idiosyncrasy
Definition
Idiosyncrasy is an abnormal, unpredictable, and qualitatively aberrant response to a drug or substance that occurs in a small subset of individuals, even at doses that are otherwise safe and well-tolerated in the general population.
"Idiosyncrasy is an allergic or anaphylactic response to a substance in which even a drug that is otherwise safe produces a toxic effect."
- P C Dikshit Textbook of Forensic Medicine and Toxicology
"Drug idiosyncrasy: The administration of drugs in amounts which are known to be harmless to a normal person may cause death due to drug idiosyncrasy, e.g., many persons are hypersensitive to cocaine."
- The Essentials of Forensic Medicine and Toxicology (2026 ed.)
Key Features of Idiosyncrasy
| Feature | Description |
|---|---|
| Dose | Occurs at normal or even sub-therapeutic doses |
| Mechanism | Genetic or acquired differences in drug metabolism |
| Predictability | Unpredictable - does not occur in most people |
| Relation to allergy | May overlap with allergic/anaphylactic mechanisms |
| Examples | Hypersensitivity to cocaine; barbiturate-induced paradoxical excitement in elderly |
Types / Mechanisms
-
Metabolic Idiosyncrasy - Due to genetic or acquired defects in drug metabolism (e.g., enzyme deficiencies). The liver may produce toxic metabolites at standard doses. Isoniazid and nitrofurantoin are classic examples.
-
Immunoallergic Idiosyncrasy - The drug triggers an immune/allergic response. Features of drug allergy (rash, eosinophilia, fever) may be present.
-
Pharmacogenetic Idiosyncrasy - Due to hereditary enzyme deficiencies (e.g., G6PD deficiency causing hemolysis with primaquine).
In Fitzpatrick's Dermatology, idiosyncrasy is classified under nonimmunologic drug reactions and defined as "reactions resulting from hereditary enzyme deficiencies."
Idiosyncrasy vs. Drug Allergy vs. Tolerance
| Idiosyncrasy | Allergy | Tolerance | |
|---|---|---|---|
| Dose relationship | No | No | Yes (higher dose needed) |
| Immune mechanism | Sometimes | Yes | No |
| Genetic basis | Often | Sometimes | Acquired |
| Prior exposure needed | No | Usually yes | Yes |
Clinical Importance (Forensic/Toxicological)
Idiosyncrasy is recognized as a cause of obscure death at autopsy - when a drug given in a standard dose causes fatal toxicity, the diagnosis relies primarily on clinical history. It must be differentiated from overdose, allergy, and anaphylaxis.
2. Immunity
Definition
Immunity is the state of protection against infection and disease, mediated by the body's defense mechanisms. It involves a network of cells, tissues, and molecules that recognize and eliminate foreign pathogens and abnormal host cells.
Two Major Arms of Immunity
Defense is mediated by sequential and coordinated responses:
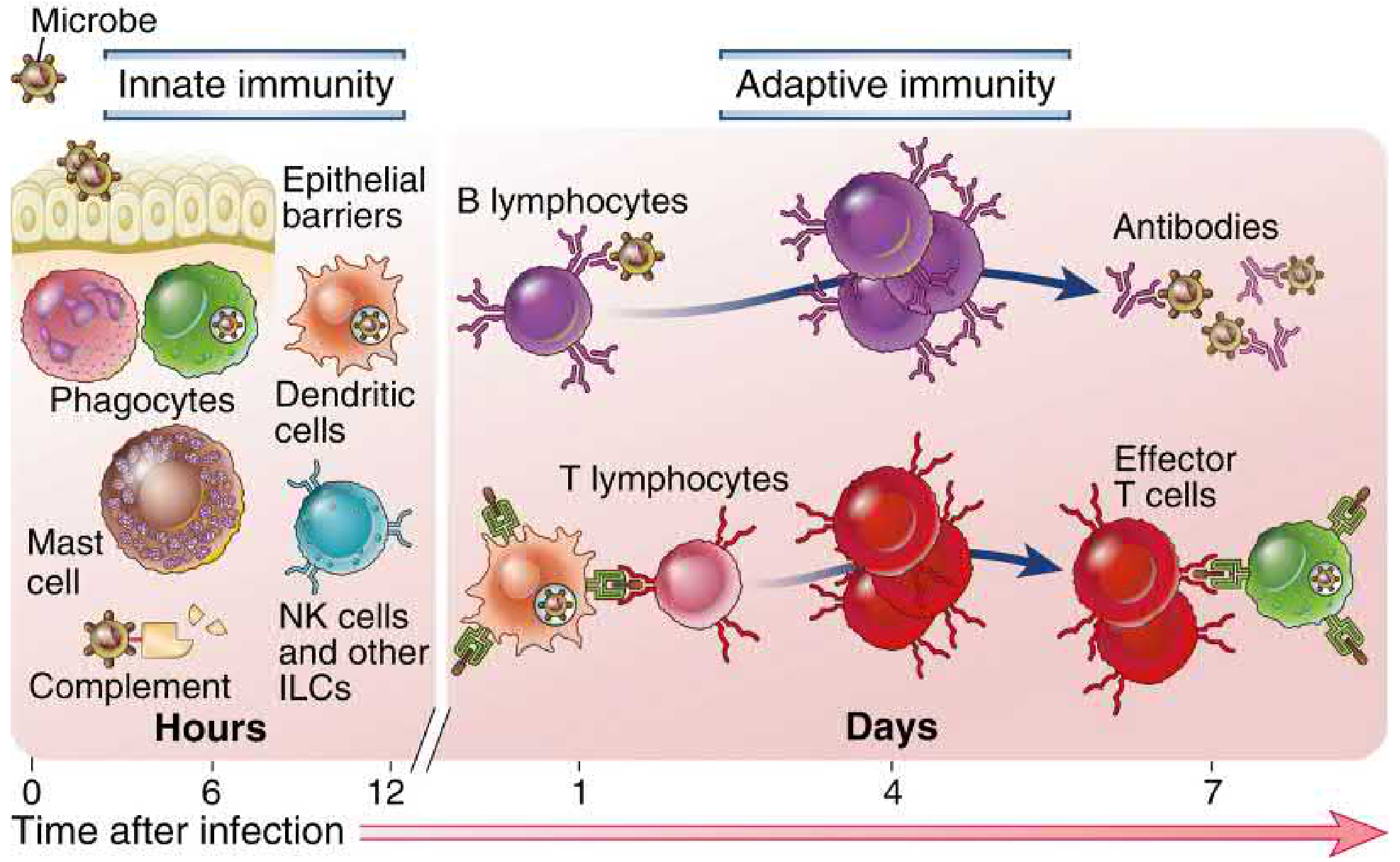
A. Innate Immunity (Natural / Native Immunity)
- First line of defense - active within hours of infection
- Mechanisms are pre-existing (in place before any infection)
- Recognizes molecular patterns shared by groups of microbes (pathogen-associated molecular patterns, PAMPs)
- No memory - same response on re-exposure
- Components: Epithelial barriers (skin, mucosa), phagocytes (macrophages, neutrophils), dendritic cells, NK cells, mast cells, complement system, innate lymphoid cells (ILCs)
B. Adaptive Immunity (Specific / Acquired Immunity)
- Second line of defense - develops over days after exposure
- Specific for individual antigens
- Immunologic memory - stronger response on re-exposure
- Components: B lymphocytes (humoral immunity) and T lymphocytes (cell-mediated immunity)
- Lymphocytes are the only cells capable of specifically recognizing antigens
Key Properties of Adaptive Immunity
| Property | Description |
|---|---|
| Specificity | Recognizes distinct antigens on different microbes |
| Diversity | Large repertoire via somatic recombination of gene segments |
| Memory | Enhanced response upon re-exposure (basis of vaccines) |
| Self-nonself discrimination | Does not attack host's own tissues (self-tolerance) |
Types of Adaptive Immunity
1. Humoral Immunity
- Mediated by B lymphocytes and antibodies (secreted by plasma cells)
- Defense against extracellular microbes
- Antibodies neutralize microbes, activate complement, and facilitate phagocytosis
2. Cell-Mediated Immunity
- Mediated by T lymphocytes and cytokines
- Defense against intracellular microbes
- CD4+ helper T cells assist macrophages and B cells
- CD8+ cytotoxic T cells kill infected cells
Active vs. Passive Immunity
| Active Immunity | Passive Immunity | |
|---|---|---|
| Source | Body's own immune response (to infection or vaccine) | Transfer of preformed antibodies or cells from another individual |
| Onset | Slow (days to weeks) | Immediate |
| Duration | Long-lasting | Temporary (weeks to months) |
| Memory | Yes | No |
| Examples | Natural infection; vaccination | Maternal antibodies to newborn; antiserum; immunoglobulin therapy |
"Immunity may be acquired by a response to antigens (active immunity) or conferred by transfer of antibodies or effector cells (passive immunity)."
- Cellular and Molecular Immunology (Abbas, Lichtman, Pillai)
Innate vs. Adaptive: Quick Comparison
| Feature | Innate | Adaptive |
|---|---|---|
| Speed | Hours | Days |
| Specificity | Low (molecular patterns) | High (individual antigens) |
| Memory | Limited | Yes |
| Diversity | Low (germline encoded) | Very high (somatic recombination) |
| Key cells | Phagocytes, NK cells, dendritic cells | B cells, T cells |
| Key molecules | Complement, lectins | Antibodies |
Connection Between Idiosyncrasy and Immunity
Idiosyncrasy and immunity intersect in drug-induced liver injury (DILI) and other adverse drug reactions. Some idiosyncratic reactions are immunoallergic in nature (the drug acts as a hapten triggering T-cell or antibody responses), while others are purely metabolic. In idiosyncratic DILI, aberrant host immunity to the drug is often implicated, but most patients lack classic hypersensitivity features (rash, eosinophilia), making the distinction between immune-mediated and metabolic idiosyncrasy important for diagnosis and management.
Sources: Cellular and Molecular Immunology (Abbas et al.) | P C Dikshit Textbook of Forensic Medicine and Toxicology | The Essentials of Forensic Medicine and Toxicology (2026) | Fitzpatrick's Dermatology | Goodman & Gilman's Pharmacological Basis of Therapeutics | Sleisenger & Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.