Screening for pda in neonates
Reading File
Finding Sources
Finding Sources
Searching PubMed
"patent ductus arteriosus" AND screening AND neonates
Reading File
Reading File
Reading File
Reading Article
PMID: 37899032
Reading Article
PMID: 41749152
Reading File
Finding Sources
Reading Article
PMID: 40870487
Loading Image
Searching the Web
PDA screening neonates pulse oximetry echocardiography criteria 2024 2025 guidelines
Finding Sources
Reading File
Reading Web Page
https://publications.aap.org/pediatrics/article/155/5/e20250…
I now have all the information needed for a comprehensive answer. Let me compile it.
Screening for PDA in Neonates
Background
Patent ductus arteriosus (PDA) is a failure of postnatal closure of the ductus arteriosus - the fetal vessel connecting the pulmonary artery to the descending aorta. At birth, rising oxygen tension triggers smooth muscle contraction and functional closure within 10-15 hours, followed by anatomic fibrosis (ligamentum arteriosum) over days to weeks.
- Incidence: ~1 in 2,000 term births; rises dramatically with prematurity
- 40-60% of VLBW infants have a PDA; reaches 60-75% in neonates <28-30 weeks gestation
- Female predominance (2:1 ratio)
- Untreated isolated PDA carries ~30% mortality, primarily from CHF
- Harriet Lane Handbook, 23rd ed., p. 243; Schwartz's Principles of Surgery, 11th ed., p. 787
Why Screening Matters
A clinically silent or small PDA may still carry risks (infectious endarteritis ~0.45%/year after the second decade). A hemodynamically significant PDA (hs-PDA) in preterm infants causes:
- Left-to-right shunting → left ventricular volume overload
- Pulmonary over-circulation → respiratory distress, BPD risk
- Diastolic "steal" → mesenteric/renal underperfusion, NEC risk
- Intraventricular hemorrhage risk in extreme preterms
Screening Methods
1. Clinical Assessment
Signs suggestive of PDA:
| Feature | Finding |
|---|---|
| Murmur | Continuous "machinery" murmur, grade 1-4/6, loudest at LUSB (left upper sternal border) / left infraclavicular area |
| Pulse | Wide pulse pressure; bounding/waterhammer pulses |
| Precordium | Hyperactive; left ventricular heave |
| Tachycardia/tachypnea | From increased sympathetic discharge |
| Cyanosis | Absent in uncomplicated left-to-right PDA; differential cyanosis (lower limbs more cyanosed than upper) if Eisenmenger reversal occurs |
In neonates, the murmur is often only systolic on the first day of life (audible at upper left sternal border / left infraclavicular area) and becomes continuous as pulmonary vascular resistance falls. In very premature infants, the classic murmur may be absent even with large shunts - clinical signs alone are unreliable.
- Goldman-Cecil Medicine, p. 1064; Schwartz's, p. 788
2. Pulse Oximetry (CCHD Screening)
The AAP 2025 updated algorithm uses pre- and post-ductal SpO₂ to screen for critical congenital heart disease (CCHD):
Timing: At 24-48 hours of age (or just before discharge if <24 hours)
Sites:
- Pre-ductal: Right hand (reflects aortic arch blood, before ductus joins)
- Post-ductal: Either foot
Interpretation:
| Result | Criteria |
|---|---|
| Pass | SpO₂ ≥95% in both sites AND difference ≤3% |
| Rescreen in 1 hr | SpO₂ 90-94% in either site, OR >3% difference |
| Fail (immediate echo) | SpO₂ <90% in either site, OR fails 3 consecutive screens |
A passing pulse oximetry screen does NOT exclude PDA. Isolated left-to-right PDA (without right-to-left shunt) typically passes oximetry. The test is most useful for detecting ductal-dependent cyanotic lesions.
- AAP 2025 CCHD Screening Protocol; CDC CCHD screening page
3. Echocardiography - The Gold Standard
Echocardiography (2D + colour Doppler) is the definitive tool for PDA diagnosis and characterisation.
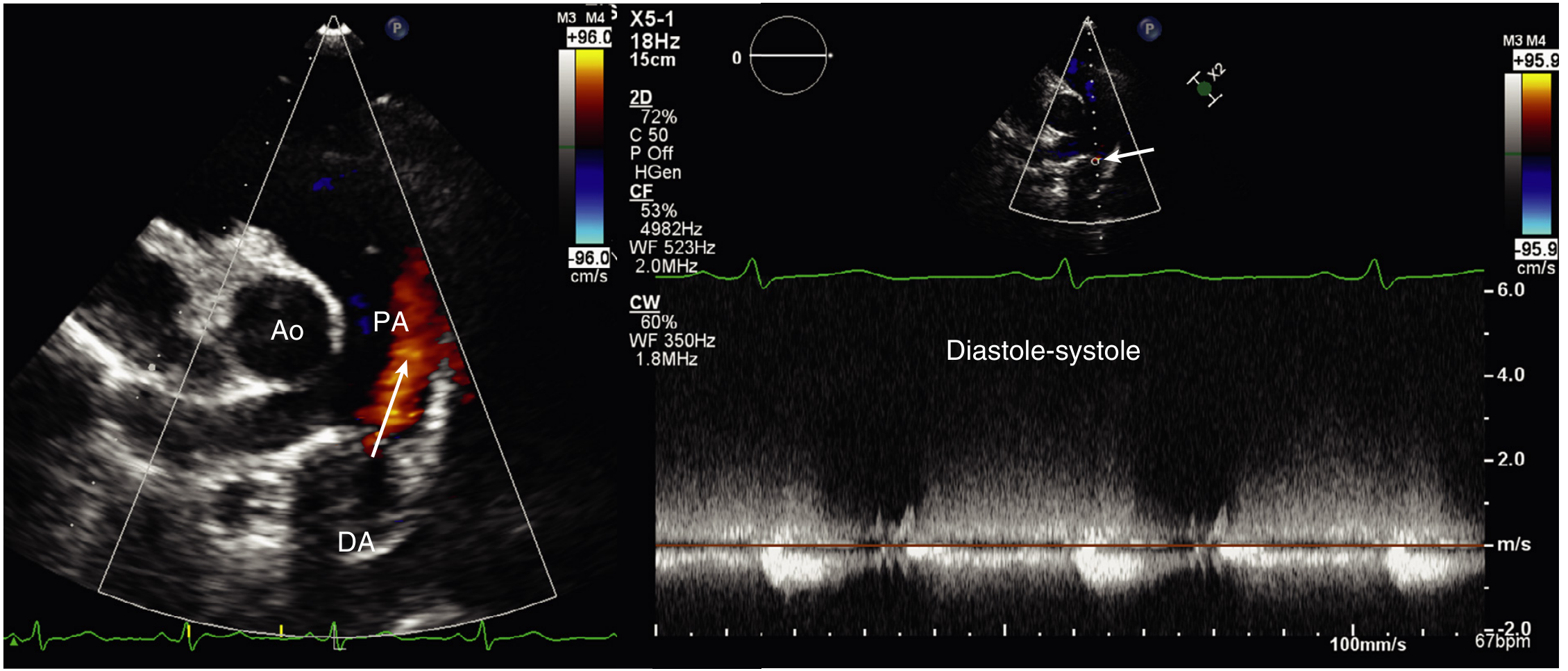
Fig. Parasternal short-axis view (left): colour Doppler jet (arrow) in the PA arising from the descending aorta (DA) in diastole. CW Doppler (right): characteristic continuous high-velocity flow from diastole through systole. (Textbook of Clinical Echocardiography)
Key echocardiographic criteria for hs-PDA:
- Ductal diameter >1.5 mm (or >1.4-1.5 mm/kg in VLBW)
- Left atrium:aortic root (LA:Ao) ratio >1.4-1.5 (indicates volume overload)
- Antegrade diastolic flow reversal in descending aorta
- Left-to-right or bidirectional ductal flow on colour Doppler
- Diastolic ductal flow in the PA has sensitivity 96%, specificity 100% for PDA diagnosis
- LV dilatation / reduced LV function
- Textbook of Clinical Echocardiography, p. 548
Targeted Neonatal Echocardiography (TnECHO)
A 2025 systematic review (PMID 40870487) of 11 studies (PRISMA, Feb 2025) found:
- TnECHO implementation associated with a 49% reduction in PDA ligation rates
- Improved diagnostic precision for shunt significance and myocardial function
- Enables physiology-guided decisions, reducing unnecessary interventions
- The 2024 ASE guidelines from the American Society of Echocardiography updated indications and training requirements for TnECHO/cPOCUS in the NICU
4. Biomarkers
BNP / NT-proBNP (serum or urinary):
- Elevated in hs-PDA due to ventricular volume/pressure overload
- A 2024 systematic review (PMID 37899032) found urinary NT-proBNP has modest sensitivity and specificity for hs-PDA; requires local validation before routine use
- NT-proBNP levels >1800 pg/mL in preterm infants are often used as a threshold, though cutoffs vary by gestational age and postnatal age
5. Near-Infrared Spectroscopy (NIRS) - Emerging
A 2026 meta-analysis (PMID 41749152) of 9 studies found:
- Cerebral rSO₂ (regional oxygen saturation) is significantly lower in PDA infants vs. controls (SMD -0.42, 95% CI -0.74 to -0.10)
- Renal rSO₂ and peripheral SpO₂ did not show significant differences
- Suggests cerebral NIRS may serve as a non-invasive bedside indicator for PDA, but AUC studies are still needed
6. Other Investigations
| Test | Finding in PDA |
|---|---|
| Chest X-ray | Cardiomegaly, increased pulmonary vascular markings, pulmonary oedema in large shunts |
| ECG | Small-moderate PDA: normal or LVH; large PDA: BVH |
| Cardiac catheterization | Reserved only when pulmonary hypertension is suspected |
Screening Strategy by Population
Term Neonates
- Routine newborn examination (auscultation at 6-24 hours and again at discharge)
- Pulse oximetry CCHD screen at 24-48 hours
- Echo only if murmur persists, abnormal oximetry, or clinical concern
Preterm Neonates (<32 weeks or VLBW)
- Routine clinical reassessment daily in NICU (murmur, bounding pulses, hyperdynamic precordium)
- Echocardiography is the standard - many units perform a screening echo at 3-7 days of life in all infants <28 weeks gestation
- Repeat echo if clinical deterioration, increasing FiO₂ requirement, or feeding intolerance
- Consider urinary NT-proBNP or cerebral NIRS as adjuncts where echo is unavailable
Key Points Summary
- Clinical signs are insensitive in very preterm infants - a large PDA can be silent on auscultation.
- Pulse oximetry screens for CCHD broadly, not PDA specifically; a left-to-right PDA will usually pass.
- Echocardiography with colour Doppler is the gold standard; diastolic PA jet has 96% sensitivity, 100% specificity.
- TnECHO by trained neonatologists is now supported by ASE 2024 guidelines and reduces overtreatment.
- Biomarkers (NT-proBNP) and cerebral NIRS are adjuncts, not replacements for echo.
- Management after diagnosis: watchful waiting in asymptomatic, COX inhibitors (indomethacin/ibuprofen/acetaminophen) for hs-PDA in preterms, catheter-based or surgical closure in term infants or those refractory to medical therapy.
This is a shared conversation. Sign in to Orris to start your own chat.