I now have everything needed for a thorough MD-exam answer. Here is the complete, structured response:
---
# Dynamic Hyperinflation - Complete Notes for MD Examination (10 Marks)
---
## 1. Definition
**Dynamic hyperinflation (DH)** is a progressive increase in end-expiratory lung volume (EELV) above the static functional residual capacity (FRC), occurring whenever there is insufficient time for complete exhalation before the next breath begins.
- It is synonymous with **intrinsic PEEP (iPEEP / auto-PEEP)**
- Auto-PEEP = alveolar pressure minus airway-opening pressure at end-expiration
- DH = the volume manifestation; auto-PEEP = the pressure manifestation of the same phenomenon
> "Dynamic hyperinflation is an increase in end-expiratory lung volume above the value that would be obtained if there was complete exhalation to the static functional residual capacity." - Goldman-Cecil Medicine
---
## 2. Pathophysiology / Mechanism
### 2a. Core Mechanism
Under normal conditions, expiration is passive and returns EELV to static FRC. DH occurs when:
1. **Expiratory flow limitation (EFL)** is present - expiratory flow does not increase despite increasing alveolar-to-atmospheric pressure gradient (as in COPD/asthma)
2. **Expiratory time is insufficient** - the next inhalation begins before complete exhalation
3. Each successive breath adds a "residual volume increment" - leading to a progressively rising EELV
### 2b. Determinants of Auto-PEEP / DH (4 key factors):
| Factor | Mechanism |
|--------|-----------|
| **High minute ventilation** | Increased respiratory rate shortens expiratory time |
| **Increased expiratory airway resistance** | Slows expiratory flow (COPD, asthma, mucus) |
| **Increased respiratory system compliance** | Lung empties more slowly (emphysema) |
| **Decreased expiratory time (short I:E ratio)** | Less time for passive recoil |
In addition, **tonic inspiratory muscle activity at end-expiration** and **positive-pressure ventilation settings** (high RR, high tidal volume) further exacerbate DH.
### 2c. PEEP₁ (intrinsic PEEP)
- The resulting positive end-expiratory alveolar pressure is called PEEP₁ or auto-PEEP
- It acts as an **inspiratory threshold load** - the patient must first overcome PEEP₁ before generating any inspiratory flow
- The ventilator does not "see" this pressure because the pressure drop is upstream of where airway pressure is measured in the circuit
---
## 3. Causes / Clinical Settings
### 3a. Obstructive Airway Diseases (commonest)
- **COPD** (emphysema + chronic bronchitis) - loss of elastic recoil + airflow obstruction
- **Acute severe asthma** (status asthmaticus) - bronchoconstriction + air-trapping
- **Bronchiectasis** - secretion-related obstruction
### 3b. Mechanical Ventilation Settings
- High respiratory rate (RR > 20/min) - shortened expiratory time
- Large tidal volumes
- Short I:E ratio (insufficient expiratory phase)
- High minute ventilation
### 3c. Other
- Tachypnea from any cause (pain, anxiety, hypoxemia) - even without intrinsic lung disease, a very high respiratory rate can produce DH
- Post-exercise in COPD patients
---
## 4. Consequences / Physiological Effects
### 4a. Respiratory Effects
| Effect | Mechanism |
|--------|-----------|
| **Increased work of breathing** | Raised EELV increases elastic recoil forces; auto-PEEP acts as threshold load |
| **Dyspnea / air hunger** | Combination of increased WOB + respiratory muscle inefficiency |
| **Respiratory muscle fatigue** | Diaphragm operates at shorter-than-optimal length (flattened); zone of apposition reduced |
| **Alveolar overdistension** | Risk of barotrauma, pneumothorax |
| **Decreased compliance (apparent)** | Respiratory system compliance appears falsely low if auto-PEEP is not corrected |
| **Increased dead space ventilation** | Overdistended alveoli compromise perfusion |
| **Hypercapnia / respiratory failure** | Progressive CO₂ retention from WOB + dead space |
### 4b. Cardiovascular Effects
- **Elevated intrathoracic pressure** raises right atrial pressure
- **Decreased venous return** - reduced driving pressure for systemic venous return
- **Right ventricular strain** - increased RV afterload
- **Hypotension** - especially immediately after intubation/sedation when compensatory mechanisms are blunted
### 4c. Ventilator-Specific Effects
- **Ineffective triggering** - patient must generate effort to overcome auto-PEEP before the ventilator detects the inspiratory effort; "failed efforts" occur in >10% of breathing attempts in ~25% of patients on pressure support
- **Underestimation of respiratory rate** - the ventilator's counted rate is lower than the patient's actual rate
- **Falsely low compliance measurements** - if auto-PEEP is not factored in
---
## 5. Measurement / Detection
### 5a. Clinical Signs
- Flow at end-expiration remains detectable on the flow-time waveform (flow does not return to zero)
- **End-expiratory flow velocity > 0** on the ventilator screen
- Patient making inspiratory efforts that fail to trigger the ventilator (ineffective efforts)
- Tachypnea with pursed-lip breathing
### 5b. Bedside Measurement (Mechanically Ventilated Patient)
**End-expiratory occlusion technique:**
- In a patient with no spontaneous breathing effort, occlude the expiratory port at end-expiration
- Alveolar, central airway, and ventilator circuit pressures equilibrate
- Auto-PEEP = measured pressure - set PEEP (read on the ventilator manometer)
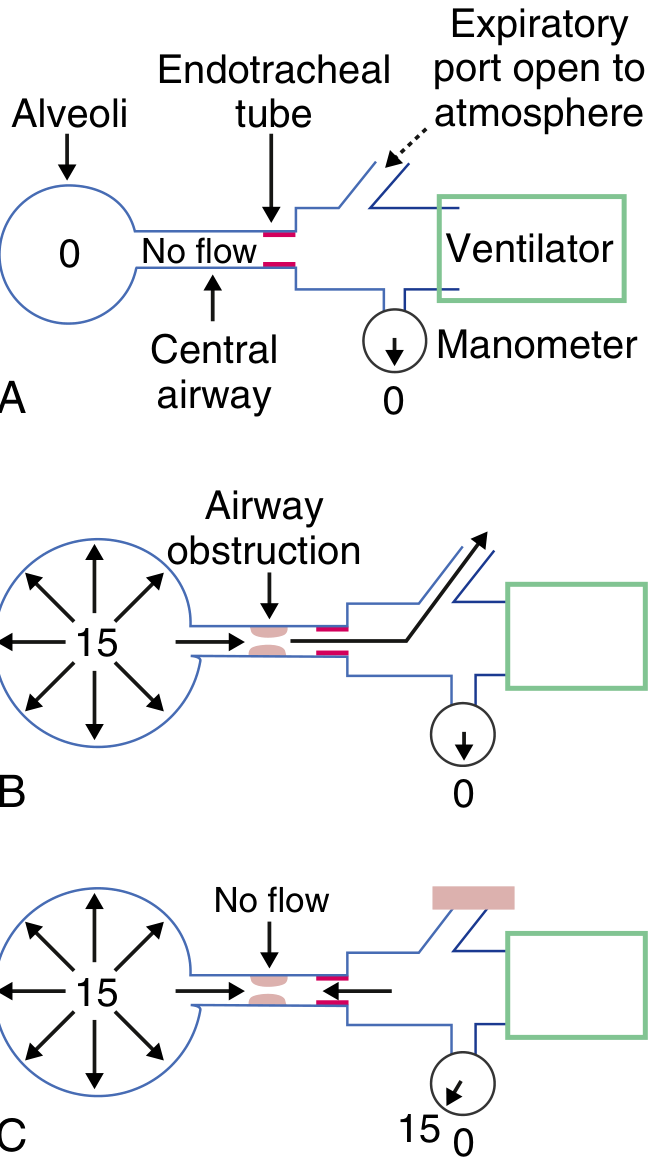
*Goldman-Cecil Medicine - E-Fig 91-1: Auto-PEEP measurement. Panel A = normal; Panel B = dynamic obstruction, port open; Panel C = port occluded, auto-PEEP reads 15 cmH₂O*
**Prolonged expiration technique:**
- Perform a prolonged expiration (20-30 seconds) to atmosphere
- Volume of gas released = volume of dynamic hyperinflation
### 5c. Spirometric/Exercise Surrogate
- **Inspiratory capacity (IC)** progressively falls as EELV rises during exercise
- IC is the most practical marker of dynamic hyperinflation during exercise testing
- IC = TLC - EELV (if TLC is constant, ↓IC = ↑EELV)
---
## 6. Clinical Implications in COPD
- Progressive exercise limitation in COPD is driven largely by DH
- DH raises WOB and exacerbates dyspnea during exertion
- **Anxiety episodes** can cause tachypnea → DH → more dyspnea → a vicious cycle
- Interventions reducing DH improve exercise capacity:
- Inhaled bronchodilators (LABA/LAMA) - reduce airway resistance
- Oxygen supplementation - reduces minute ventilation demand
- Pursed-lip breathing - slows respiratory rate, prolongs expiratory phase
- Lung volume reduction surgery (LVRS) - improves elastic recoil and reduces DH
- Pulmonary rehabilitation
---
## 7. Management
### 7a. Non-Ventilated Patient (COPD/Asthma)
- **Bronchodilators** (SABA + SAMA nebulization) - reduce airway resistance and time constant
- **Systemic corticosteroids** - reduce airway inflammation and secretions
- **Heliox** - low-density gas mixture, reduces turbulent flow, improves expiratory flow
- **Pursed-lip breathing** - self-PEEP stenting of airways, slows RR, prolongs expiration
- **NIV/BiPAP** - external PEEP offsets auto-PEEP, reduces inspiratory threshold load
- **Positioning** - upright reduces abdominal load on diaphragm
### 7b. Mechanically Ventilated Patient
**Core principle: minimize minute ventilation + maximize expiratory time**
| Strategy | Rationale |
|----------|-----------|
| **Low respiratory rate** (10-14/min) | Most effective measure to reduce DH; rates <10 not recommended (causes unacceptable hypercapnia) |
| **Low tidal volume** (≤ 8 mL/kg predicted body weight) | Reduces minute ventilation |
| **Prolonged expiratory time** (high I:E ratio, e.g., 1:3 or 1:4) | Allows more complete lung emptying |
| **Permissive hypercapnia** | Accept elevated PaCO₂; target pH >7.2 rather than normalizing CO₂ |
| **Bronchodilators + suctioning** | Reduce expiratory resistance |
| **Applied external PEEP (extrinsic PEEP)** | Set at ~75-85% of measured auto-PEEP to "stent" the airway; reduces inspiratory threshold load without worsening DH |
| **Sedation and paralysis** (initial phase) | Eliminates tonic respiratory muscle activity; allows controlled low-RR ventilation |
**Permissive hypercapnia target:** Accept PaCO₂ elevation so long as pH > 7.2
**Ventilator settings in acute COPD (Rosen's Emergency Medicine):**
- Mode: Volume assist-control
- RR: 10-14/min
- TV: ≤ 8 mL/kg predicted BW
- Inspiratory time: 0.8-1.0 seconds
- PEEP: 5 cmH₂O
- SpO₂ target: 88-92%
---
## 8. Auto-PEEP and Triggering Failure (High-Yield for Exams)
- If auto-PEEP = 10 cmH₂O and trigger sensitivity is set at -2 cmH₂O, the patient must generate -12 cmH₂O effort to trigger the ventilator
- Failed triggers = patient effort does not produce a breath; seen on flow-time waveform as small deflections without delivered breaths
- Solution: apply external PEEP ≈ 75-85% of auto-PEEP to reduce the threshold the patient must overcome
---
## 9. Summary - High-Yield Points for Exam
| Point | Key Fact |
|-------|---------|
| Definition | ↑ EELV above static FRC due to incomplete expiration |
| Pressure correlate | Auto-PEEP (intrinsic PEEP) |
| Main cause | COPD, acute severe asthma, MV with high RR |
| Best bedside measure (MV) | End-expiratory occlusion pressure |
| Surrogate during exercise | ↓ Inspiratory capacity (IC) |
| Cardiovascular danger | ↓ Venous return → hypotension (esp. post-intubation) |
| Ventilator management | ↓ RR (10-14/min), ↓ TV, ↑ E time, permissive hypercapnia |
| Triggering failure cause | Patient must overcome auto-PEEP before triggering |
| Treatment (pharmacologic) | Bronchodilators, steroids, heliox |
| Non-pharmacologic | Pursed-lip breathing, NIV, LVRS |
---
**Sources:**
- Goldman-Cecil Medicine International Edition (2 vol.), p. 1064-1065
- Murray & Nadel's Textbook of Respiratory Medicine (2 vol.) - Expiratory Flow Limitation chapter, p. 716
- Fishman's Pulmonary Diseases and Disorders (2 vol.) - Natural History of COPD chapter
- Murray & Nadel's - Oxygen Cost of Breathing chapter
- Rosen's Emergency Medicine - Respiratory Failure & Invasive Ventilation chapter, p. 948
