explain me about bone histology in detail for midterms and final exams
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have everything needed for a comprehensive, exam-ready bone histology guide. Let me compile this into a detailed, well-organized response.
Bone Histology - Complete Exam Guide
Sources: Histology: A Text and Atlas (Pawlina, 9e) | Miller's Review of Orthopaedics (9e)
1. Overview of Bone as a Tissue
Bone is a specialized connective tissue consisting of cells embedded in a mineralized extracellular matrix. It provides mechanical support, protects organs, serves as a mineral reservoir (calcium and phosphate), and houses hematopoietic marrow.
2. Types of Bone
Microscopic Classification
| Feature | Woven (Immature) Bone | Lamellar (Mature) Bone |
|---|---|---|
| Collagen orientation | Random, disorganized | Organized, stress-oriented |
| Osteocyte density | More per unit volume | Fewer |
| Strength | Weaker, more flexible | Stronger, less flexible |
| Turnover | High | Low |
| Examples | Embryonic skeleton, fracture callus, osteogenic sarcoma, fibrous dysplasia | Normal adult bone |
Exam tip: Woven bone = pathologic or immature. Finding woven bone in an adult = abnormal (except healing fractures). Lamellar bone is secondary bone formed by remodeling of woven bone.
Macroscopic Classification
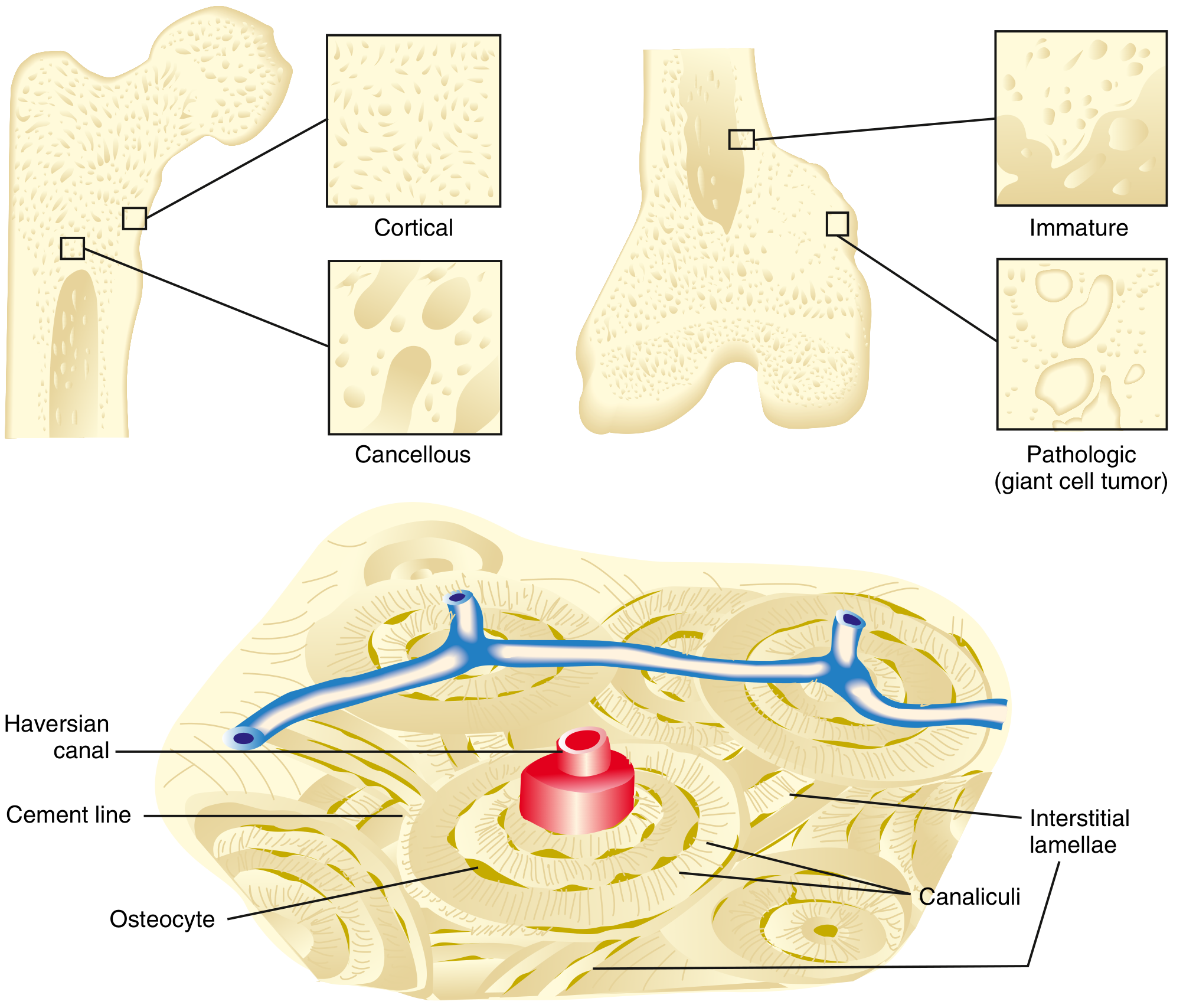
Cortical (Compact) Bone
- Makes up ~80% of the skeleton (e.g., femoral shaft)
- Slow turnover rate; high Young's modulus (stiff)
- Organized into tightly packed osteons (Haversian systems)
- Each osteon = concentric lamellae surrounding a central Haversian canal (contains arterioles, venules, capillaries, nerves)
- Volkmann canals run perpendicular to Haversian canals, connecting them to each other and to the periosteum
- Cement lines define the outer border of each osteon
- Interstitial lamellae are remnants of old osteons between current ones
- Canaliculi carry osteocyte cell processes and provide nutrition between lacunae and canals
Cancellous (Spongy / Trabecular) Bone
- Makes up ~20% of the skeleton (e.g., distal femoral metaphysis)
- High turnover rate; lower Young's modulus (more elastic)
- Meshwork of trabeculae surrounding marrow spaces
- No true osteons (too thin for a Haversian system); osteocytes are nourished by diffusion from marrow
3. Bone Matrix
Organic component (~35%):
- Type I collagen (90% of organic matrix) - provides tensile strength
- Non-collagenous proteins: osteopontin, osteonectin, osteocalcin, bone sialoprotein, proteoglycans
- Osteoid = unmineralized organic matrix (the precursor layer laid down by osteoblasts before mineralization)
Inorganic component (~65%):
- Hydroxyapatite crystals: Ca₁₀(PO₄)₆(OH)₂
- Provides compressive strength and rigidity
- Also contains carbonate, magnesium, fluoride, sodium
Exam tip: Remove mineral from bone = flexible (like cartilage). Remove organic = brittle/chalk-like. This shows each component's role.
4. Bone Cells (The Four Cell Types)
4a. Osteoprogenitor Cells (Osteogenic Cells)
- Resting stem cells derived from mesenchymal stem cells (MSCs)
- Found in periosteum (inner cambium layer), endosteum, and lining Haversian canals
- Flat, spindle-shaped, pale-staining on H&E
- Activated by growth factors (BMPs, FGFs) to differentiate into osteoblasts
4b. Osteoblasts
- Bone-forming cells derived from osteoprogenitor cells (mesenchymal lineage)
- Morphology: cuboidal to columnar, basophilic cytoplasm (rich in RER and Golgi), single nucleus
- Arranged in a single layer along bone surfaces being formed
- Function: synthesize and secrete osteoid (type I collagen + non-collagenous proteins), then orchestrate its mineralization
- Also produce alkaline phosphatase (ALP) - a clinical marker of bone formation
- Produce osteoprotegerin (OPG) - a decoy receptor that inhibits osteoclast formation
- Produce RANKL - stimulates osteoclast differentiation
- When an osteoblast becomes completely surrounded by matrix it secreted, it becomes an osteocyte
4c. Osteocytes
- The most abundant bone cell (~90-95% of all bone cells)
- Former osteoblasts now embedded in lacunae within calcified matrix
- Transformation from osteoblast to osteocyte takes ~3 days; cell volume reduces ~70%, organelles decrease, ~50 long cell processes develop
- Cell processes radiate into canaliculi and communicate with neighboring osteocytes and surface cells via gap junctions (connexins)
- In H&E sections: nucleus is the main visible feature (cell body is shrunken by decalcification artifact); canaliculi are visible in ground sections
- Functions:
- Mechanosensors - detect mechanical strain (piezoelectric signals)
- Regulate bone remodeling via sclerostin (inhibits Wnt signaling = inhibits osteoblast activity)
- Produce FGF-23 - regulates phosphate reabsorption in kidneys
- Produce PGE2 (under stress) - stimulates RANKL production, activating osteoclasts
4d. Osteoclasts
- Bone-resorbing cells
- Derived from hematopoietic precursors (granulocyte/monocyte progenitor cells - GMP, CFU-GM) via fusion - NOT from osteoblast lineage
- Morphology: large, multinucleated (up to 50 nuclei), acidophilic (eosinophilic) cytoplasm
- Located in Howship lacunae (resorption pits on bone surface)
- Have a characteristic ruffled border (infolded plasma membrane) adjacent to bone - greatly increases surface area for resorption
- Have a clear zone (sealing zone) that isolates the resorption compartment
Mechanism of bone resorption:
- Osteoclast attaches to bone via integrin receptors (αvβ3)
- Sealed compartment formed at ruffled border
- Secretes H⁺ (via carbonic anhydrase II + vacuolar H⁺-ATPase) to acidify the compartment → dissolves hydroxyapatite
- Secretes cathepsin K (lysosomal protease) and MMPs → degrades organic matrix (collagen)
- Degradation products are transcytosed and released into blood
RANK/RANKL/OPG Axis (critical exam topic):
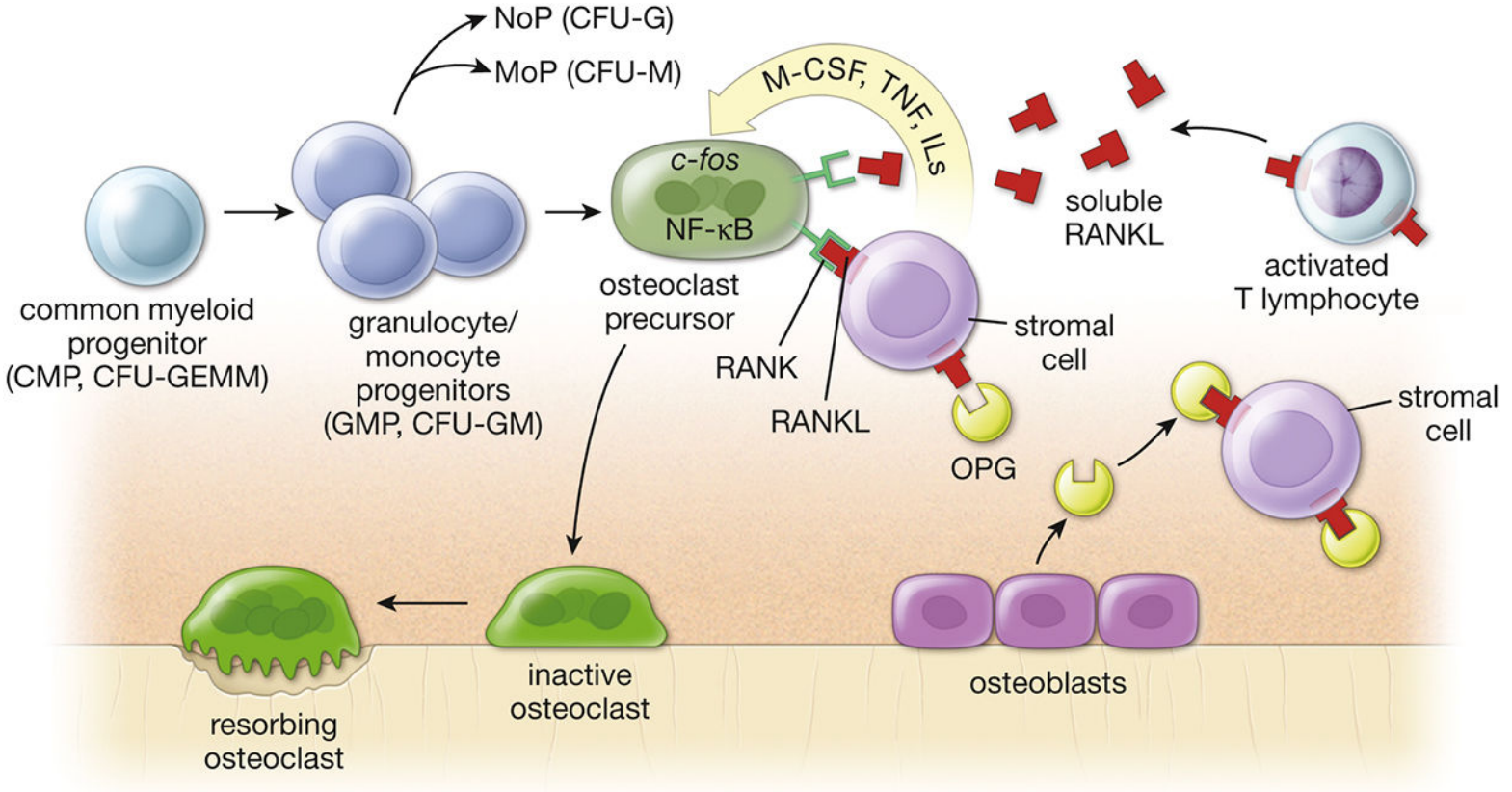
- RANKL (expressed on osteoblasts/stromal cells/T lymphocytes) binds RANK (on osteoclast precursors) → stimulates osteoclast differentiation and activation
- OPG (produced by osteoblasts) = decoy receptor, binds RANKL and blocks RANK-RANKL interaction → inhibits osteoclast formation
- During inflammation, activated T lymphocytes produce RANKL → increased bone resorption (e.g., rheumatoid arthritis, periodontitis)
- All substances promoting remodeling act through the OPG/RANKL system
- Osteoclast differentiation requires transcription factors c-fos and NF-κB, and cytokines M-CSF, TNF, and interleukins
| Cell | Origin | Location | Key Feature |
|---|---|---|---|
| Osteoprogenitor | Mesenchymal stem cell | Periosteum, endosteum, Haversian canals | Flat, spindle-shaped |
| Osteoblast | Osteoprogenitor | Bone surfaces | Cuboidal, basophilic, ALP+ |
| Osteocyte | Osteoblast | Lacunae in matrix | Most abundant, mechanosensor |
| Osteoclast | Hematopoietic (GMP) | Howship lacunae | Multinucleated, ruffled border |
5. Bone Formation (Ossification)
5a. Intramembranous Ossification
- Bone forms directly from mesenchyme - no cartilage intermediate
- Produces flat bones of the skull, mandible, clavicle, and some facial bones
- Also produces the periosteal collar in long bones
Process:
- Mesenchymal cells condense and differentiate directly into osteoblasts within a highly vascularized connective tissue membrane
- Osteoblasts secrete osteoid → mineralizes to form bony spicules
- Spicules enlarge and fuse → woven bone trabeculae
- Woven bone is later remodeled into lamellar bone
- Periosteum and endosteum form from surrounding mesenchyme
5b. Endochondral Ossification
- Bone forms on a hyaline cartilage template
- Produces long bones, short bones, vertebrae, and pelvis
- Begins in the second trimester and continues into early adulthood at the growth plate
Process (Early - Fetal):
- Mesenchyme → hyaline cartilage model (chondrocytes)
- Chondrocytes at center hypertrophy → matrix calcifies
- Perichondrial cells → osteoblasts → periosteal bone collar forms (intramembranous component)
- Blood vessels invade → vascular endothelial growth factor (VEGF) is critical here
- Osteoblasts arrive → deposit bone on calcified cartilage spicules (primary ossification center)
- Two secondary ossification centers form at epiphyses
- Growth plate (epiphyseal plate) remains as the only remaining cartilage for continued longitudinal growth
Epiphyseal Growth Plate Zones (memorize these!):
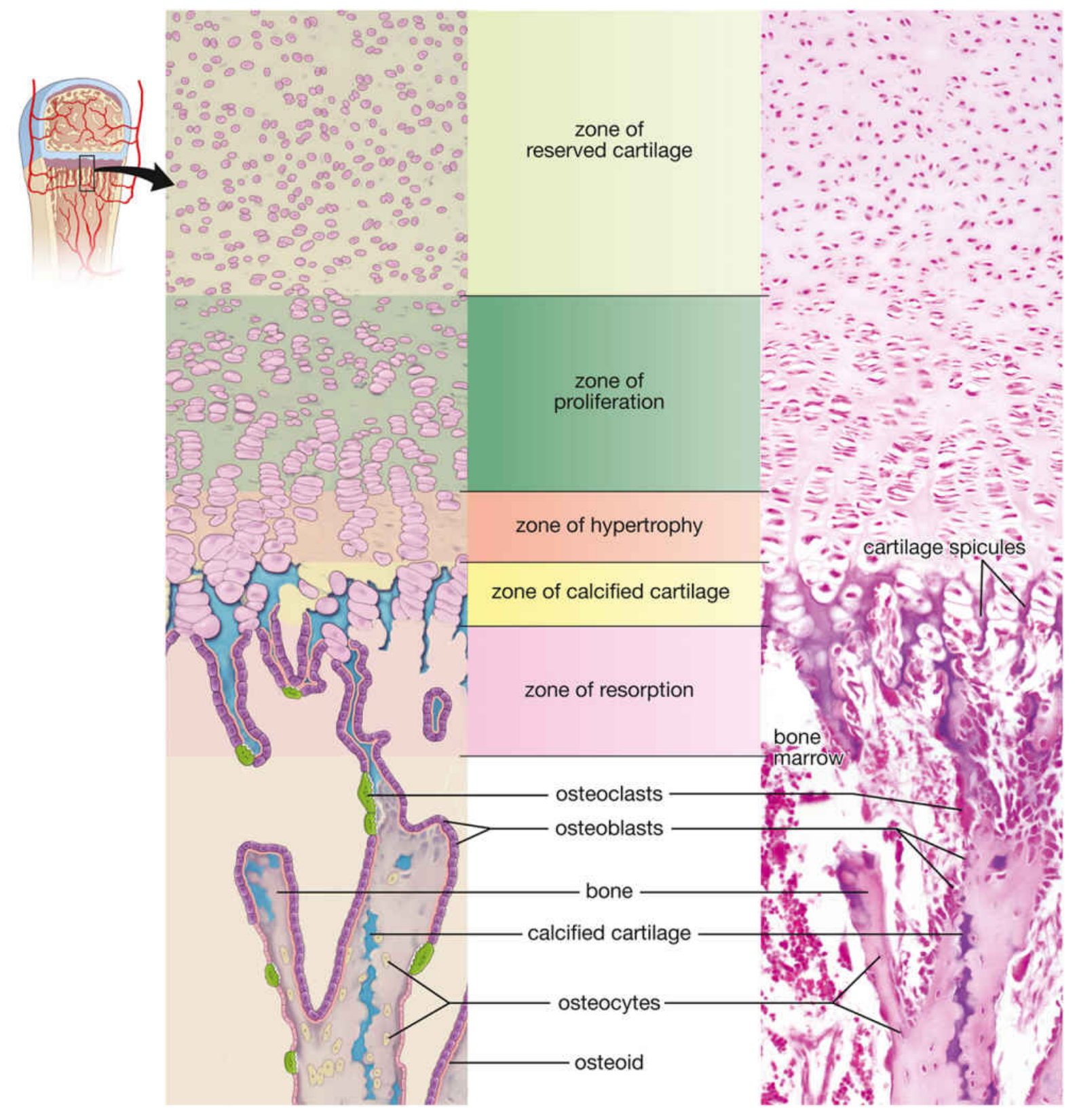
From epiphysis → diaphysis:
| Zone | What Happens | Key Features |
|---|---|---|
| Zone of Reserve Cartilage | Stores cartilage | No proliferation; scattered chondrocytes; small cells |
| Zone of Proliferation | Cell division | Chondrocytes form columns (stacked coins); produce type II and XI collagen; most mitotic activity |
| Zone of Hypertrophy | Cells enlarge | Chondrocytes swell 5-10x; produce type X collagen; alkaline phosphatase increases |
| Zone of Calcified Cartilage | Matrix mineralization | Calcium deposits; chondrocytes die by apoptosis; tide mark separates hypertrophic from calcified |
| Zone of Resorption (Ossification) | Bone deposition | Blood vessels invade; osteoclasts resorb calcified cartilage; osteoblasts deposit bone on calcified cartilage scaffolding |
Mnemonic for growth plate zones: "Resting Preschoolers Have Cleaned Rooms" → Reserve, Proliferation, Hypertrophy, Calcified, Resorption
Clinical link: Rickets disrupts the zone of hypertrophy and calcification (deficient mineralization). Achondroplasia is due to FGFR3 mutation that inhibits chondrocyte proliferation in the zone of proliferation.
6. Bone Remodeling
Remodeling is the ongoing process of bone resorption and formation that:
- Maintains calcium homeostasis
- Repairs microfractures
- Adapts bone architecture to mechanical load (Wolff's Law)
Basic Multicellular Unit (BMU) = Cutting Cone:
- Osteoclasts at the front cut a tunnel through cortical bone
- Osteoblasts follow and fill the tunnel with new concentric lamellae
- Creates a new osteon
Remodeling sequence: Activation → Resorption → Reversal → Formation → Quiescence
Regulators:
| Factor | Effect on Bone |
|---|---|
| PTH (chronic high levels) | Stimulates resorption (via RANKL ↑, OPG ↓) |
| PTH (intermittent low-dose) | Anabolic - stimulates formation |
| Calcitonin | Inhibits osteoclasts |
| Estrogen | Inhibits RANKL; promotes OPG; anti-resorptive |
| Vitamin D (1,25-OH) | Increases calcium absorption; regulates mineralization |
| Sclerostin (from osteocytes) | Inhibits Wnt → inhibits osteoblasts |
| BMPs | Activate SMADs → osteoblastic differentiation |
7. Periosteum and Endosteum
Periosteum:
- Covers outer bone surface (except articular cartilage)
- Two layers:
- Outer fibrous layer: dense irregular CT, blood vessels, nerves
- Inner cambium (osteogenic) layer: osteoprogenitor cells and osteoblasts
- Essential for appositional growth and fracture repair
- Attached to bone via Sharpey's fibers (perforating fibers of collagen)
Endosteum:
- Lines all internal bone surfaces (Haversian canals, Volkmann canals, trabeculae, medullary cavity)
- Single layer of flattened osteoprogenitor cells and bone-lining cells
- More active than periosteum in normal adult bone remodeling
8. Special Stains and Identification (High-Yield for Practical Exams)
| Feature | Stain | Appearance |
|---|---|---|
| Osteoid | H&E | Pink, homogeneous, unmineralized |
| Mineralized bone | H&E after decalcification | Pale pink, structureless matrix with lacunae |
| Canaliculi | Ground sections (not decalcified) | Fine dark lines radiating from lacunae |
| Osteoclast ruffled border | EM | Infolded plasma membrane at Howship lacuna |
| Collagen (type I) | Masson's trichrome | Blue-green |
| Calcified cartilage vs bone | Mallory-Azan | Light blue (calcified cartilage) vs. dark blue (bone) |
9. High-Yield Exam Facts Summary
- Most abundant bone cell: Osteocyte
- Most important bone-forming cell: Osteoblast
- Marker of bone formation: Alkaline phosphatase (ALP), osteocalcin
- Marker of bone resorption: Tartrate-resistant acid phosphatase (TRAP) in osteoclasts; urinary collagen crosslinks (NTX, CTX)
- Osteoclast lineage: Hematopoietic (myeloid), NOT mesenchymal
- Osteoblast lineage: Mesenchymal stem cells
- Only cartilage remaining after endochondral ossification in adults: Articular cartilage (growth plate fuses at end of puberty)
- Cement line composition: Mineralized matrix rich in osteopontin; lacks collagen fibrils
- Wolff's Law: Bone adapts its structure to mechanical loads (piezoelectric mechanism)
- Woven bone is ALWAYS pathologic in adults (except healing fractures and certain physiologic states)
- Collagen type in bone: Type I (bone/tendon); Type II (cartilage); Type X (hypertrophic zone of growth plate only)
Sources: Histology: A Text and Atlas with Correlated Cell and Molecular Biology (Pawlina/Ross, 9e) | Miller's Review of Orthopaedics, 9e
This is a shared conversation. Sign in to Orris to start your own chat.