Parotid gland anatomy with all information and simple way explanation
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Finding Sources
I now have everything needed to write a comprehensive, well-illustrated answer. Let me compile it.
Parotid Gland Anatomy - Complete Guide
🔶 What Is the Parotid Gland?
The parotid gland is the largest of the three paired major salivary glands (parotid, submandibular, sublingual). It is a pure serous gland - meaning it produces watery, enzyme-rich saliva (specifically salivary amylase) rather than mucus. It contributes about 25% of total daily saliva production.
Think of it simply: it sits in front of your ear, hugs the jaw, and squirts digestive saliva into your mouth when you eat.
📍 Location and Borders
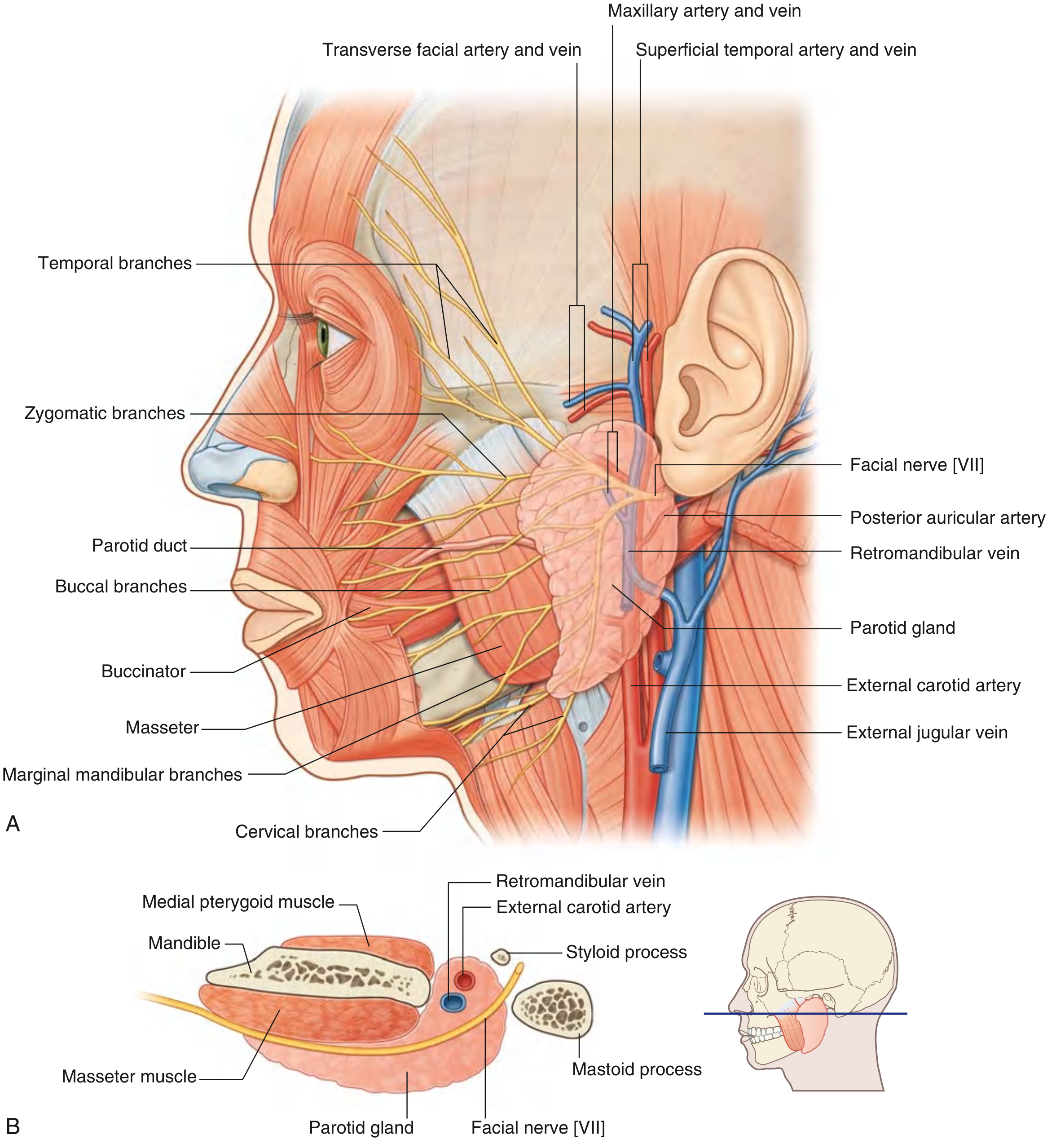
Fig. 8.65 - Parotid Gland: (A) Lateral view showing facial nerve branches and vascular anatomy, (B) Cross-sectional view - Gray's Anatomy for Students
The parotid occupies the parotid space - an irregular wedge-shaped region on the lateral face.
| Border | Structure |
|---|---|
| Anterior | Masseter muscle (extends halfway across it) |
| Superior | Zygomatic arch |
| Posterior | Tragal cartilage + sternocleidomastoid muscle |
| Inferior | Tail of parotid (between ramus of mandible and SCM, overlying digastric muscle) |
| Deep | Pretyloid compartment of parapharyngeal space |
The gland is anterior to and below the lower half of the ear, extending from the zygomatic arch above to the lower border of the mandible below. Posteriorly it covers the anterior part of the sternocleidomastoid muscle.
🧱 Fascial Capsule (Covering)
The parotid is enclosed by the parotidomasseteric fascia (a split of the investing layer of deep cervical fascia):
- Attaches to the root of the zygomatic arch
- Thin fascia separates it from the tragal and conchal cartilage (can be separated by blunt dissection)
- Thick fascia attaches to the mastoid process posteriorly
- Thick fascia at the anterior and inferior tip separates the parotid from the submandibular gland
The fascia is tough and inelastic - which is why parotitis (parotid inflammation) is so painful; the swelling has nowhere to expand.
🔲 Lobes: Superficial vs Deep
The facial nerve divides the parotid into two lobes:
| Lobe | Size | Location |
|---|---|---|
| Superficial lobe | ~80% of gland | Lateral to facial nerve |
| Deep lobe | ~20% of gland | Medial to facial nerve |
Simple memory: "The facial nerve is the dividing line." If you remove the gland surgically, you must track the nerve to avoid splitting the gland dangerously.
🟡 The Most Important Structure: Facial Nerve (CN VII)
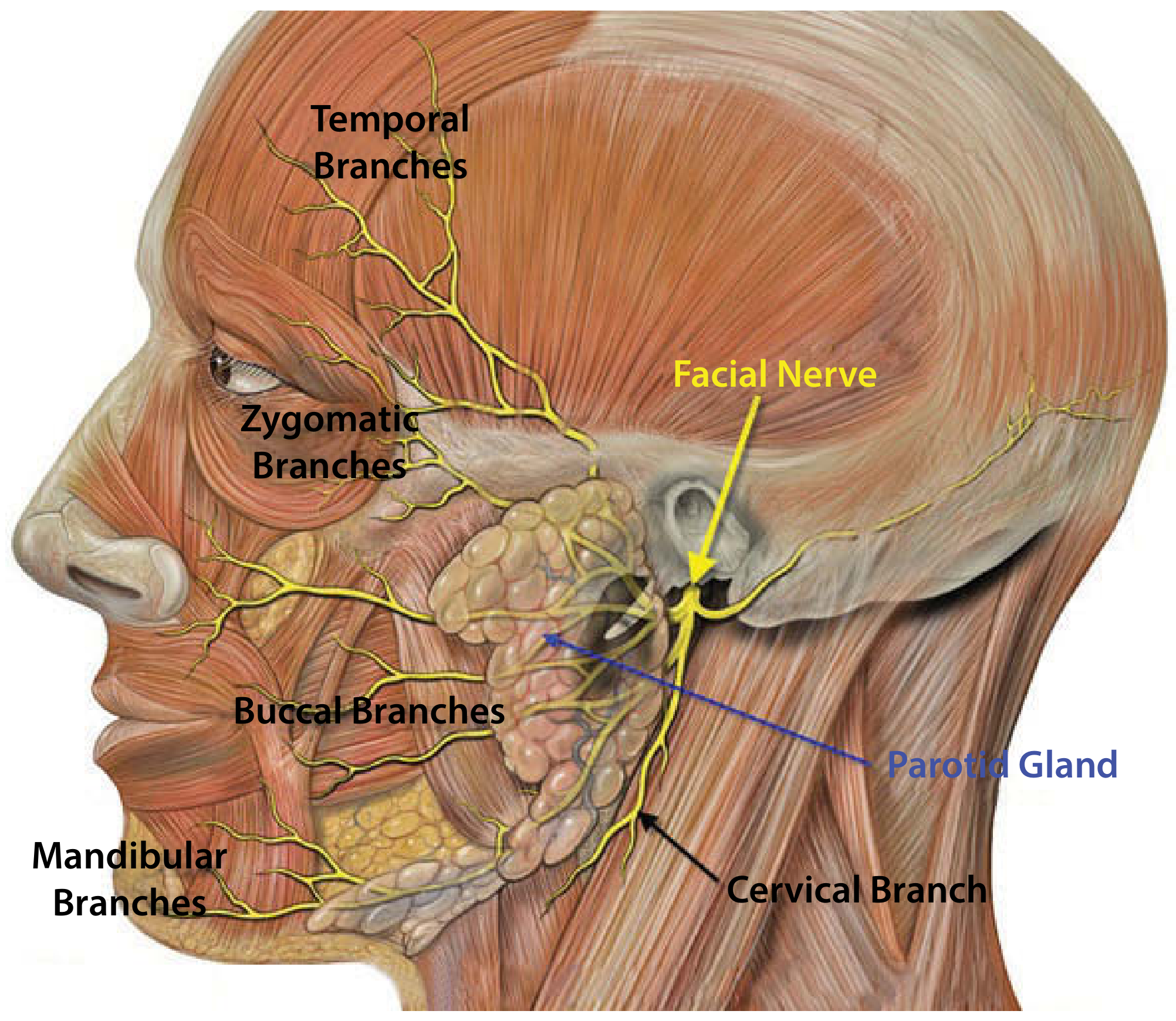
Fig. 43.2 - Anatomy of the parotid gland with facial nerve branches - Scott-Brown's Otorhinolaryngology
The facial nerve is THE critical structure in parotid surgery. Here's the pathway:
- Exits skull through the stylomastoid foramen (posterolateral to styloid process, anteromedial to mastoid process)
- Enters the parotid and divides at the pes anserinus ("goose's foot")
- Splits into upper (temporofacial) and lower (cervicofacial) divisions
- Gives off 5 terminal branch groups that exit the gland borders:
| Branch | Exits From | Function |
|---|---|---|
| Temporal | Upper border | Raises eyebrow, closes eye |
| Zygomatic | Upper/anterior border | Closes eyelid |
| Buccal | Anterior border | Smile, nose movement |
| Marginal mandibular | Lower border | Lip depression |
| Cervical | Lower border | Neck (platysma) |
Clinical note: The facial nerve trunk is more superficial in children under 2 years - a key surgical risk. Damage to upper branches prevents eye closure (risk of corneal injury). Lower branch damage causes facial asymmetry.
Landmarks to Find the Facial Nerve Surgically
- Tympanomastoid suture line
- Posterior belly of digastric muscle (marks nerve depth)
- Tragal pointer (most commonly used - nerve lies ~1 cm deep and inferior to the tragal tip)
- Retrograde identification by tracing a peripheral branch back to the trunk
🩸 Blood Supply
Arterial supply comes from arteries passing through the gland substance (not a single dedicated artery):
- External carotid artery courses medial to the gland, dividing into:
- Maxillary artery - passes horizontally deep to mandible
- Superficial temporal artery - gives off the transverse facial artery before exiting the upper border
Venous drainage:
- Superficial temporal vein + Maxillary vein join inside the gland to form the retromandibular vein
- Retromandibular vein divides into:
- Anterior division - joins with facial vein → internal jugular vein
- Posterior division - joins posterior auricular vein → external jugular vein
🔵 Parotid Duct (Stensen's Duct)
The duct is the drainage pipe of the parotid:
- Exits the anterior edge of the gland midway between the zygomatic arch and the corner of the mouth
- Travels across the face horizontally, crossing the masseter muscle
- At the anterior border of the masseter, it turns 90° and dives deep through the buccal fat pad
- Pierces the buccinator muscle
- Opens into the oral cavity opposite the upper second molar tooth (2nd maxillary premolar region)
Simple rule: The duct runs along a line from the tragus to the midpoint between the nose and upper lip. It opens near your upper 2nd molar - you can see it as a small papilla.
🧠 Nerve Supply (Innervation)
| Type | Nerve | Pathway |
|---|---|---|
| Secretomotor (parasympathetic) | Glossopharyngeal nerve (CN IX) | CN IX → Tympanic nerve → Lesser petrosal nerve → Otic ganglion → Auriculotemporal nerve → Parotid gland |
| Sensory | Auriculotemporal nerve (branch of V3, mandibular division of trigeminal) | Carries sensation from the gland |
| Sympathetic | Superior cervical ganglion | Controls vasoconstriction in gland vessels |
Simple way: Eating activates CN IX → otic ganglion → auriculotemporal nerve → parotid secretes saliva. This same pathway causes Frey's Syndrome (sweating instead of salivating after parotid surgery, when regenerating secretomotor fibers accidentally innervate sweat glands of the facial skin).
Great auricular nerve (C2, C3) provides cutaneous sensation to the overlying skin - often divided during parotidectomy, causing numbness over the angle of the mandible and lower ear.
🔗 Lymphatics
The parotid is unique among salivary glands: it has ~20 intraglandular lymph nodes (inside the gland itself) as well as periglandular nodes. This is clinically important:
- Skin cancers of the scalp and face drain to these nodes
- Malignant tumors arising from these intraglandular nodes can mimic primary parotid tumors
- The submandibular gland, by contrast, only has periglandular nodes
🏥 Key Clinical Points
| Condition | Anatomical Basis |
|---|---|
| Parotitis (mumps) | Pain is severe because tight fascia cannot expand |
| Parotid stones | Form in the main duct or duct confluences; anterior stones - duct incision; posterior stones - total gland removal |
| Parotid tumors | 80-90% arise in superficial lobe (because 80% of tissue is superficial); 80% are benign; pleomorphic adenoma is most common |
| Frey's syndrome | Post-parotidectomy gustatory sweating - misdirected secretomotor fibers |
| Facial palsy risk | Any parotid surgery - nerve runs through gland; 1-2% risk of permanent palsy |
| Deep lobe tumors | Present as palate/oropharynx swelling ("dumbbell tumor" through stylomandibular tunnel) |
🗺️ Quick Summary Diagram (Text-based)
ZYGOMATIC ARCH (superior border)
↑
[EAR] → PAROTID GLAND ← [MASSETER muscle anterior]
↓ ↓
SCM posterior PAROTID DUCT → crosses masseter
→ pierces buccinator
→ opens near upper 2nd molar
INSIDE the gland:
External carotid artery → Maxillary + Superficial temporal arteries
Retromandibular vein (formed here)
Facial nerve VII → divides → 5 branch groups exit at borders
~20 lymph nodes (unique to parotid!)
Sources:
- Gray's Anatomy for Students, Chapter 8 (parotid gland, pp. 1051-1052)
- K.J. Lee's Essential Otolaryngology, Chapter on salivary glands (pp. 642-643)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Chapter 43 (parotid anatomy)
- Bailey and Love's Short Practice of Surgery 28th Edition, Chapter 54 (salivary glands)
This is a shared conversation. Sign in to Orris to start your own chat.