
Interpret ECG
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
Wolff-Parkinson-White syndrome ECG delta wave short PR interval
I have all the information needed. Let me now provide a thorough ECG interpretation.
ECG Interpretation
Clinical Context (from the Russian text)
The note mentions: episodes that begin and end suddenly ("начинаются/заканчиваются внезапно"), regular rhythm, stable blood pressure. This describes paroxysmal palpitations.
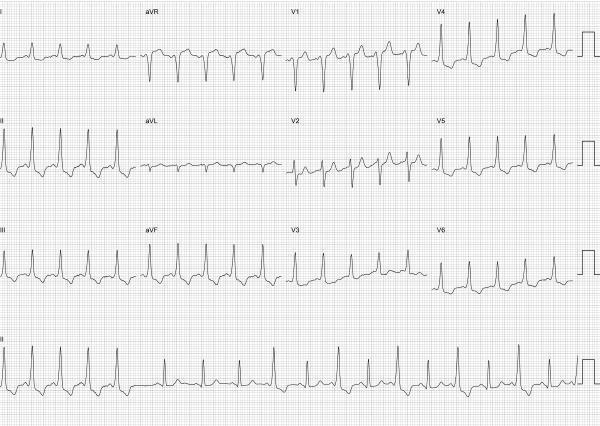
Key ECG Findings (Systematic Analysis)
| Parameter | Finding |
|---|---|
| Rate | ~75–80 bpm (regular) |
| Rhythm | Sinus, regular |
| PR interval | Short (<120 ms) |
| QRS width | Slightly prolonged (~110–120 ms) |
| Initial QRS | Slurred, slow upstroke (delta waves) — best seen in I, aVL, V2–V6 |
| ST/T waves | Discordant changes (opposite to delta/QRS vector) |
| Q waves | Pseudo-Q pattern in inferior leads (II, aVF, III) |
Diagnosis: Wolff-Parkinson-White (WPW) Syndrome
The classic triad is present:
- Short PR interval — impulse bypasses the AV node via an accessory pathway (Bundle of Kent), reaching the ventricle early
- Delta wave — slurred initial QRS deflection from aberrant ventricular activation through the accessory pathway before normal His-Purkinje activation arrives
- Widened/fused QRS — fusion of pre-excitation (delta) and normal His-Purkinje activation
"The PR interval is shortened in sinus rhythm because the impulse moving through the accessory pathway is not subject to the physiologic slowing within the AV node. The ventricle is activated by two separate pathways, resulting in a fused, or slightly widened, QRS complex." — Tintinalli's Emergency Medicine
Accessory Pathway Localization
Using delta wave polarity:
- Lead V1: Positive delta wave → suggests a left-sided accessory pathway
- Inferior leads (II, III, aVF): Negative/isoelectric delta waves → creates pseudo-Q waves, points to left posteroseptal or left posterior location
- Lead I / aVL: Positive delta waves
This pattern (positive delta in V1, negative in inferior leads) is most consistent with a left posteroseptal accessory pathway.
"A positive delta wave in V1 indicates a left-sided accessory pathway" — Braunwald's Heart Disease
Associated Pseudo-infarction Pattern
The negative delta waves in II, III, aVF mimic inferior wall Q waves and must not be mistaken for inferior MI. This is a well-recognized WPW pitfall.
Clinical Implications
The paroxysmal episodes described (sudden onset/offset) represent likely orthodromic AVRT (the most common tachycardia in WPW, ~65%):
- Narrow QRS tachycardia
- Rate 160–220 bpm
- Regular
- No delta wave during tachycardia (ventricles activate via normal AV node/His-Purkinje)
Management considerations:
- Avoid AV node blockers (digoxin, verapamil, diltiazem, adenosine) in antidromic AVRT or pre-excited AF — they can accelerate conduction down the accessory pathway → VF
- Electrophysiology study + radiofrequency catheter ablation is curative (>95% success rate)
- Risk stratification for sudden cardiac death (SCD risk: 0.15–0.39% lifetime)
Reference ECG for Comparison

Classic WPW: short PR, delta waves (slurred QRS upstroke), secondary ST/T changes
Summary: This is a textbook WPW pattern — sinus rhythm with ventricular pre-excitation via a left-sided (likely left posteroseptal) accessory pathway. The clinical presentation of paroxysmal SVT fits orthodromic AVRT. Referral for EP study and ablation is the definitive next step.
— Tintinalli's Emergency Medicine, p. 2142–2144 | Braunwald's Heart Disease | Fuster & Hurst's The Heart, 15th Ed., p. 1135

Interpret ECG
Finding Sources
Searching Images
WPW Wolff-Parkinson-White ECG intermittent pre-excitation alternating delta wave
This is a highly instructive ECG. Let me provide a detailed, systematic interpretation.
ECG Interpretation
Immediate Observation — A Tale of Two Patterns
This tracing shows two distinct QRS morphologies alternating across the strip. This is the key finding that makes this ECG different from a simple WPW tracing.
Systematic Analysis
| Parameter | Pre-excited beats | Non-pre-excited beats |
|---|---|---|
| PR interval | Short (<120 ms) | Normal (~160 ms) |
| QRS width | Widened (~120 ms) | Narrow (~80 ms) |
| Delta wave | Present (slurred upstroke) | Absent |
| QRS morphology | Fused (delta + His-Purkinje) | Normal |
| ST/T | Discordant secondary changes | Normal |
Diagnosis: Intermittent (Transient) Ventricular Pre-excitation — Intermittent WPW
The tracing shows alternating beats — some with the classic WPW triad (short PR + delta wave + wide QRS) and others with completely normal conduction. This is intermittent pre-excitation, where the accessory pathway conducts only on some beats depending on:
- The heart rate and timing of the impulse
- The refractory period of the accessory pathway at that moment
- Autonomic tone modulating pathway conduction
"The ECG hallmark of an antegradely conducting AP is an unusually short PR interval and a slurred upstroke to the QRS complex (delta wave). Conversely, the presence of retrograde conduction only in an AP will not be apparent on a surface ECG during sinus rhythm." — Fuster & Hurst's The Heart, 15th Ed.
Accessory Pathway Localization (from pre-excited beats)
Analyzing delta wave polarity in pre-excited beats:
- Lead V1: Negative/isoelectric delta (rS pattern) → right-sided pathway
- Lead II / aVF: Upright/positive delta → rules out posteroseptal
- Lead I / aVL: Positive delta
- Precordial transition: Early in V2–V3
This pattern is consistent with a right anteroseptal or right free-wall accessory pathway.
Critical Clinical Significance of Intermittent Pre-excitation
Paradoxically, intermittent pre-excitation carries important prognostic information:
- When the accessory pathway disappears abruptly during sinus rhythm or with exercise, it suggests the pathway has a long refractory period — meaning it cannot sustain rapid conduction during AF, which lowers (but does not eliminate) the risk of ventricular fibrillation
- However, it can still support AVRT with paroxysmal palpitations
- The Russian text confirms: "episodes begin and end suddenly" ("начинаются/заканчиваются внезапно") — consistent with paroxysmal AVRT
"Electrophysiologic studies can identify patients with multiple accessory tracts and short refractory periods in those tracts and, thus, who are at increased risk for ventricular fibrillation and cardiac arrest." — Tintinalli's Emergency Medicine
Comparison ECG — Intermittent Pre-excitation with delta waves
Summary
Diagnosis: Intermittent WPW syndrome — sinus rhythm with beat-to-beat alternation between pre-excited (delta wave, short PR, wide QRS) and normally-conducted (no delta wave, normal PR, narrow QRS) complexes. The accessory pathway localizes to the right side based on delta wave polarity. The clinical history of paroxysmal episodic palpitations fits orthodromic AVRT as the likely tachycardia mechanism.
Next steps:
- EP study to assess accessory pathway refractory period
- Radiofrequency catheter ablation — curative with >95% success for right-sided pathways
- Avoid empiric AV nodal blockers (digoxin, verapamil) without EP characterization
— Tintinalli's Emergency Medicine | Braunwald's Heart Disease | Fuster & Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.