how does the iodine dye is the cause of acute kideny injury
contrast induced nephropathy iodine mechanism acute kidney injury
Contrast-Induced Acute Kidney Injury (CI-AKI) from Iodinated Dye
Terminology (Important Distinction)
| Term | Meaning |
|---|---|
| Post-contrast AKI (PC-AKI) | Any AKI within 48 h of contrast - correlative, not necessarily caused by contrast |
| CIN | A subset of PC-AKI where contrast is the confirmed cause |
Mechanisms of Injury (3 Main Pathways)
1. Renal Vasoconstriction - Medullary Ischemia
- Contrast media triggers release of vasoactive substances including adenosine and endothelin
- These cause afferent arteriolar constriction, reducing glomerular blood flow
- The renal medulla is especially vulnerable because it already operates at near-hypoxic levels (the thick ascending limb has high O2 demand but poor blood supply)
- Result: medullary ischemia and tubular cell death from oxygen deprivation
"Vasoactive substances such as adenosine and endothelin mediate vasoconstriction of the afferent arterioles, thereby reducing kidney blood flow and promoting kidney medullary ischemia." - National Kidney Foundation Primer on Kidney Diseases, 8e
2. High Viscosity - Sluggish Peritubular Blood Flow
- Isosmolar contrast agents (IOCM) are ~twice as viscous as low-osmolar agents (LOCM), even though their osmolality is lower
- Their high viscosity slows blood flow through peritubular capillaries, further worsening oxygenation of tubular epithelium
- This promotes hypoxic injury and epithelial cell necrosis even without direct osmotic damage
3. Direct Tubular Toxicity - Oxidative Stress
- High-osmolality contrast media cause hyperosmolar injury to proximal tubular cells
- This leads to vacuolization of tubular cells (osmotic nephrosis)
- Contrast also generates reactive oxygen species (free radicals), triggering:
- Oxidative stress
- Activation of the polyol-fructokinase pathway in the proximal tubule
- Tubular cell apoptosis and necrosis
- In animal studies, volume depletion further reduces antioxidant enzyme activity, amplifying this injury
"Radiocontrast causes direct renal tubular toxicity through hyperosmolar injury, which results in vacuolization of proximal tubular cells, and oxidative stress from free oxygen radicals with associated tubular cell apoptosis and necrosis." - NKF Primer on Kidney Diseases, 8e
Contrast Agent Properties That Matter
| Property | Impact |
|---|---|
| High osmolality (HOCM) | Greatest risk - causes most direct tubular injury |
| Low osmolality (LOCM) | Reduced risk vs HOCM |
| Isosmolar (IOCM) | Lowest osmolar injury, but high viscosity offsets benefit |
| Volume of contrast | More contrast = greater injury; limit to ≤150 mL in high-risk patients |
Risk Factors
- Preexisting CKD (eGFR <45 mL/min/1.73m² significantly increases risk; eGFR <30 is high risk)
- Diabetes mellitus (especially diabetic nephropathy)
- Volume depletion / dehydration
- Congestive heart failure
- Advanced age (>60-75 years)
- Concurrent nephrotoxic drugs (NSAIDs, diuretics)
- High contrast volume or repeated studies
- Intraaortic balloon pump (marker of poor cardiac output and renal hypoperfusion)
- Multiple myeloma in dehydrated patients
"Volume depletion or renal hypoperfusion are the most significant risk factors." - Comprehensive Clinical Nephrology, 7th Ed.
Urinalysis Finding
- Low FENa (<1%) due to constrictive or tubular obstructive effects
- Muddy brown granular casts on urine sediment (marker of ATN)
- The injury pattern is essentially acute tubular necrosis (ATN)
Prevention Strategies
| Strategy | Evidence |
|---|---|
| IV/oral hydration (isotonic saline) | Most effective - improves renal blood flow, dilutes contrast in tubules, suppresses RAAS and ADH |
| Limit contrast volume | Use minimum necessary; <150 mL in at-risk patients |
| Use LOCM or IOCM | Avoid high-osmolar agents in CKD patients |
| N-acetylcysteine (NAC) | Thiol antioxidant - evidence is inconsistent; a large RCT (PRESERVE trial) showed no benefit over saline |
| Sodium bicarbonate | Mixed evidence; no proven superiority over normal saline |
| Hold nephrotoxins | Stop NSAIDs 24 h before; hold diuretics |
| Alternative imaging | Consider ultrasound, non-contrast CT, or MRI |
Important Caveat from Recent Data
intra renal cuase
Intrarenal (Intrinsic) Causes of Acute Kidney Injury
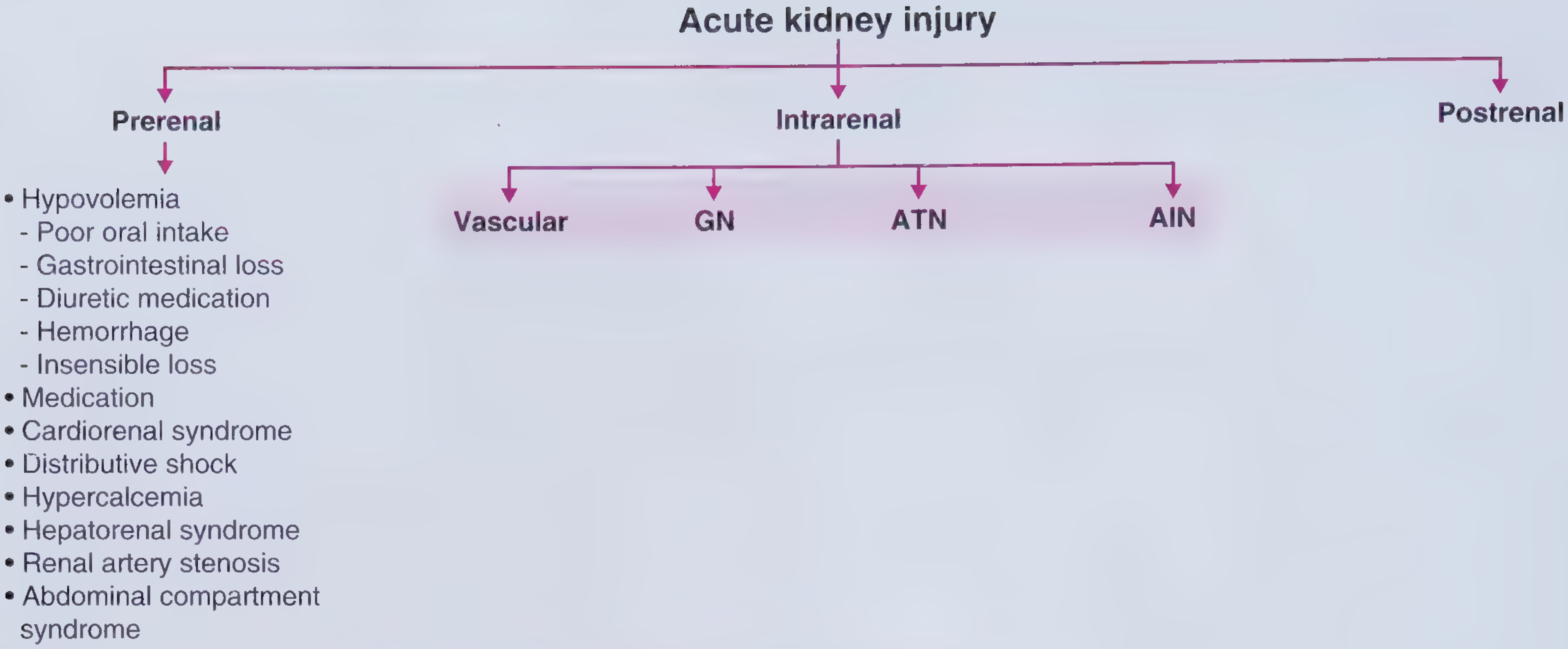
1. Acute Tubular Necrosis (ATN)
A. Ischemic ATN (Prerenal spectrum → ATN)
- Cardiogenic shock, septic shock, hemorrhage
- Post-cardiac surgery (cardiopulmonary bypass)
- Post-major vascular surgery (aortic cross-clamping)
- Severe burns, acute pancreatitis
B. Nephrotoxic ATN
| Category | Specific Agents |
|---|---|
| Antibiotics | Aminoglycosides, vancomycin, polymyxins, amphotericin B |
| Antiviral/antifungal | Foscarnet, tenofovir, pentamidine |
| Chemotherapy | Cisplatin, methotrexate, ifosfamide |
| Contrast dye | Iodinated contrast (CIN) |
| NSAIDs | Reduce prostaglandin-mediated afferent dilation |
| Pigment nephropathy | Myoglobin (rhabdomyolysis), hemoglobin (hemolysis) |
| Protein injury | Light chains (multiple myeloma - cast nephropathy) |
"ATN is the most common cause of AKI in the hospital (just under one-half of all cases), and is particularly prevalent in the ICU (more than one-half of all cases)." - Frameworks for Internal Medicine
- FENa >1-2% (tubules cannot reabsorb sodium)
- Muddy brown granular casts on microscopy (≥6 casts = likelihood ratio 10 for ATN)
- Exception: FENa can be <1% in contrast-induced and pigment nephropathy due to afferent arteriolar constriction on top of tubular injury
2. Acute Interstitial Nephritis (AIN)
Causes:
| Cause | Details |
|---|---|
| Drugs (>75% of cases) | Antibiotics (penicillins, cephalosporins, sulfonamides), NSAIDs, PPIs, diuretics, immune checkpoint inhibitors |
| Infection (~15%) | Streptococcal, leptospirosis, CMV, EBV, hantavirus |
| Autoimmune/systemic | Sarcoidosis, SLE, Sjogren's syndrome |
| TINU syndrome | Tubulointerstitial nephritis + uveitis |
Classic Triad (present in only ~10-15% overall):
- Fever
- Maculopapular rash
- Peripheral eosinophilia
- Leukocyturia and white blood cell casts (most cases)
- Urine eosinophils (less reliable)
3. Glomerulonephritis (GN)
Causes:
- Anti-GBM disease (Goodpasture syndrome) - linear IgG deposits
- Pauci-immune GN / ANCA vasculitis:
- GPA (Granulomatosis with Polyangiitis / Wegener's) - sinus disease, hemoptysis, AKI
- EGPA (Eosinophilic GPA / Churg-Strauss)
- Microscopic polyangiitis
- Immune complex GN: post-streptococcal GN, IgA nephropathy (Henoch-Schönlein purpura), lupus nephritis, MPGN
- Dysmorphic red blood cells (acanthocytes)
- Red blood cell (RBC) casts - pathognomonic
4. Vascular Causes (Intrarenal)
| Condition | Key Feature |
|---|---|
| Renal artery embolism | Sudden flank pain; AF, endocarditis, cardiomyopathy as source |
| Renal artery thrombosis | Severe flank pain, sudden onset; on background of atherosclerotic RAS |
| Atheroembolic renal disease | After arterial instrumentation; cholesterol crystal emboli; eosinophilia + hypocomplementemia; stuttering AKI over weeks |
| Thrombotic Microangiopathy (TMA) | Triad: microangiopathic hemolytic anemia + thrombocytopenia + AKI; causes = TTP, HUS, malignant HTN, HELLP, DIC, scleroderma renal crisis, drugs (cocaine, chemotherapy) |
| Large/medium vessel vasculitis | Giant cell arteritis, Takayasu (large), polyarteritis nodosa (medium) |
| Small vessel vasculitis | GPA, EGPA, microscopic polyangiitis, HSP - often cause GN |
| Malignant hypertension | Onion-skin arteriolar changes + TMA pattern |
| Scleroderma renal crisis | TMA + severe hypertension |
Summary Table
| Category | Compartment | Key Urine Finding | Example |
|---|---|---|---|
| ATN | Tubules | Muddy brown granular casts, FENa >1% | Ischemia, aminoglycosides, contrast |
| AIN | Interstitium | WBC casts, leukocyturia | NSAIDs, PPIs, antibiotics |
| GN | Glomerulus | RBC casts, dysmorphic RBCs, proteinuria | ANCA vasculitis, anti-GBM, lupus |
| Vascular | Vessels | Variable; eosinophilia (atheroemboli) | TMA, TTP-HUS, renal artery emboli |
give me some sah ct scan image with it s labelles for begginers
SAH on CT Scan - A Beginner's Guide
What to look for on a non-contrast CT head
Image 1 - SAH from a Ruptured Basilar Artery Aneurysm
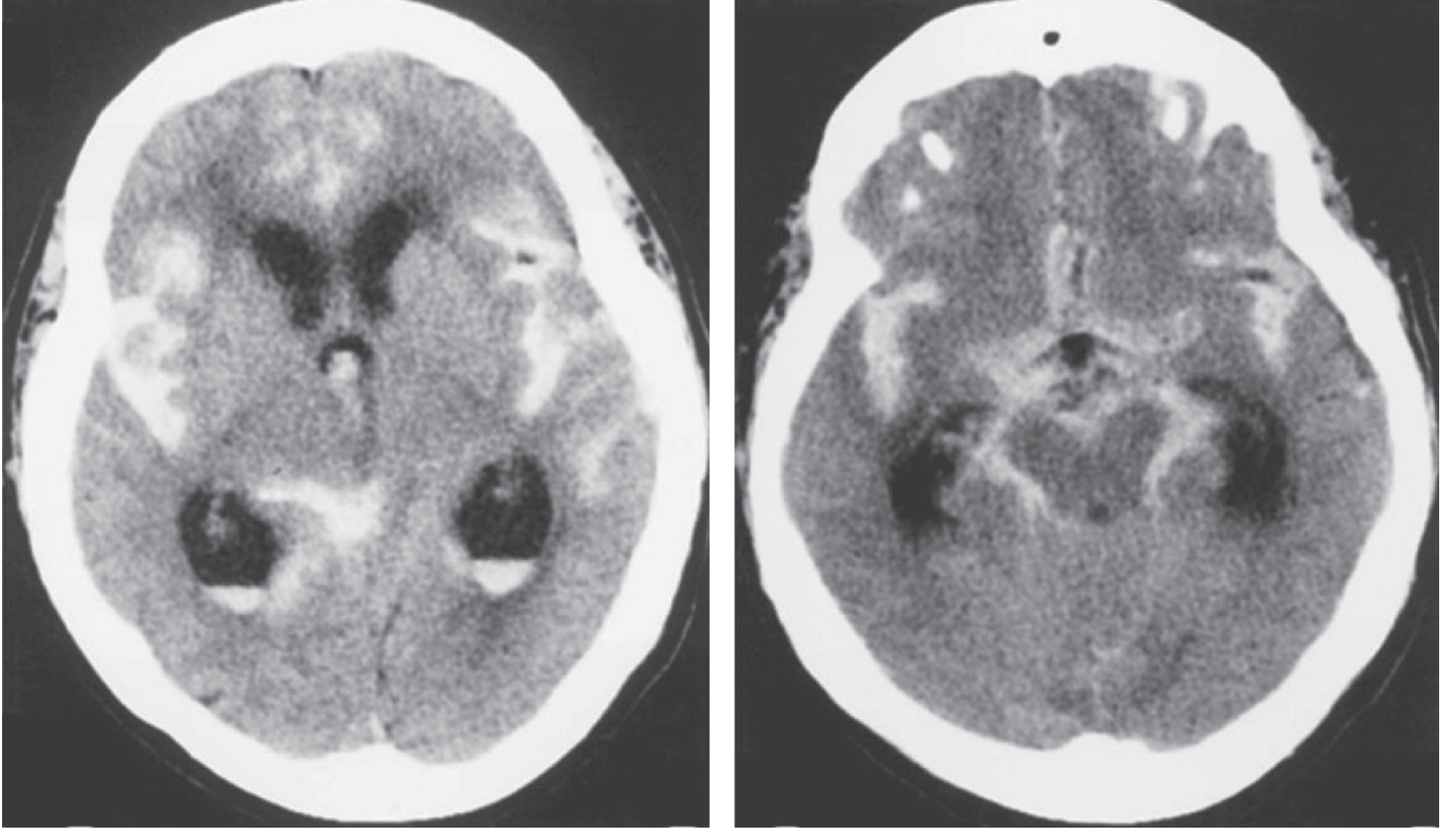
| What you see | What it means |
|---|---|
| Bright white areas spread through the middle of the brain | Blood flooding the subarachnoid spaces around the basal cisterns |
| Bright white layering inside the dark ventricles | Intraventricular hemorrhage (IVH) - blood has entered the ventricle cavities |
| Blood-CSF level in the posterior horns | Typical of recent, acute bleeding |
| Enlarged ventricles | Acute hydrocephalus - blood blocking CSF drainage |
| What you see | What it means |
|---|---|
| Bright white surrounding the brainstem | Blood in the perimesencephalic cistern (around the midbrain) |
| Bright white in the Sylvian fissures (sides) | Blood tracking into the Sylvian fissures |
| Bright white at the front between the hemispheres | Blood in the anterior interhemispheric fissure |
Image 2 - Hunt & Hess Grade III SAH with Identified Aneurysm
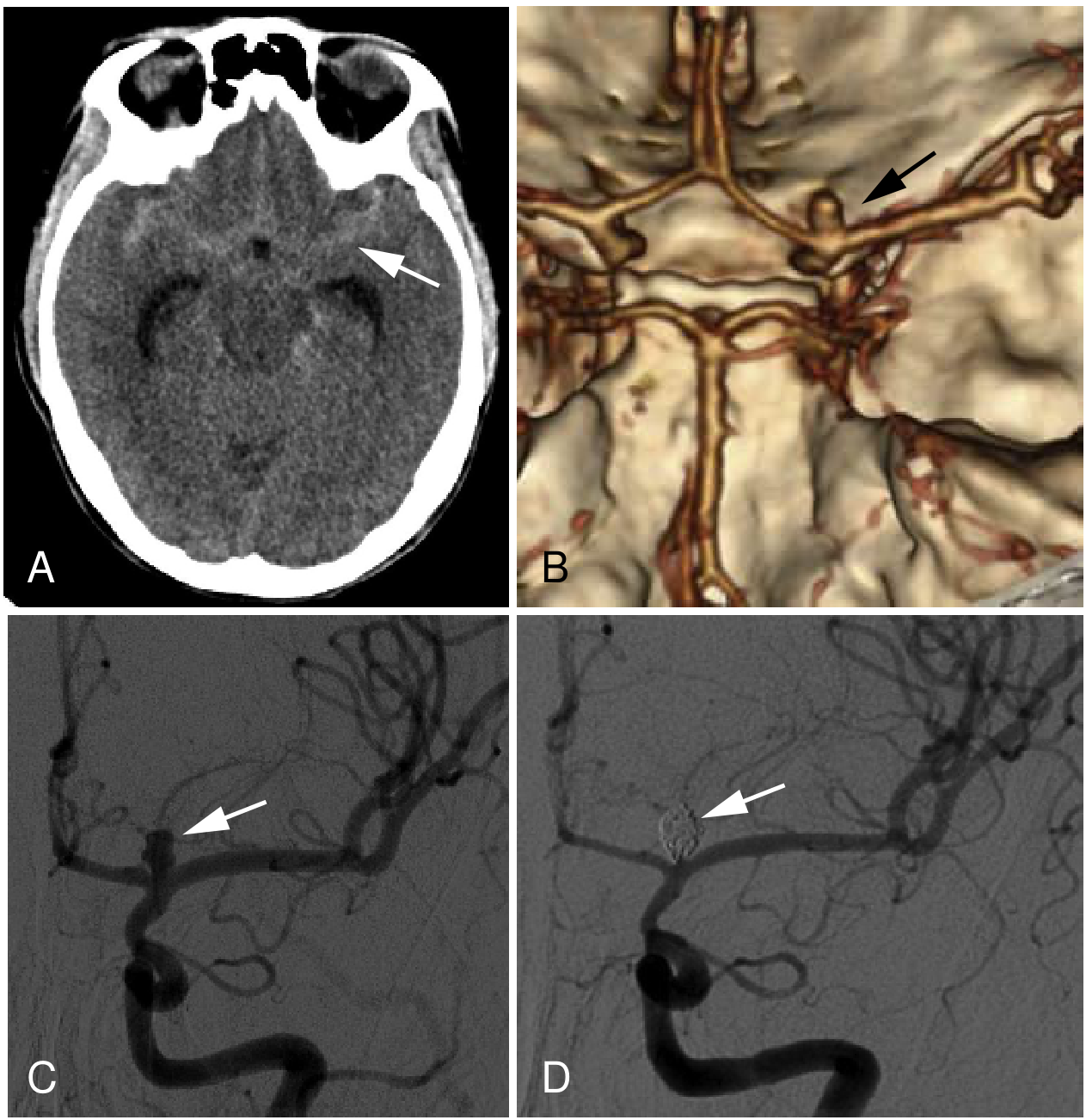
| Panel | What it shows |
|---|---|
| A - Non-contrast CT | White arrow points to extensive hyperdense (bright white) subarachnoid blood - this is Fisher Grade 3 (thick clot) |
| B - 3D CT Angiography (CTA) | Black arrow identifies the saccular (berry) aneurysm at the left internal carotid artery terminus - the source of the bleed |
| C - DSA before treatment | White arrow shows the aneurysm on digital subtraction angiography - confirms the anatomy |
| D - DSA after coiling | White arrow shows the aneurysm obliterated with platinum coils - no more flow into the sac |
Key Anatomy - Where Does Blood Go in SAH?
Subarachnoid Space
|
_____|_______________________________________________
| | | | |
Basal Sylvian Interhemis- Cortical Ventricles
Cisterns Fissures pheric Sulci (if severe)
(around (sides of Fissure (surface → IVH
brainstem) brain) (midline) sulci) → Hydrocephalus
What CT Can Tell You
| Finding | Clinical Meaning |
|---|---|
| Hyperdense blood in basal cisterns | Classic SAH - look at the star-shaped cistern around the brainstem |
| Location of most blood | Hints at aneurysm location (blood clusters near the rupture site) |
| Thick blood clot (Fisher Grade 3) | High risk of vasospasm in 4-14 days |
| Enlarged ventricles | Acute hydrocephalus - may need emergency EVD |
| Intraparenchymal hematoma | Aneurysm ruptured directly into brain tissue |
Key Facts for Beginners
- CT sensitivity: >90% in first 12 hours; drops to ~50% at 5-7 days as blood breaks down (becomes isodense)
- If CT is negative but SAH suspected: Do a lumbar puncture → look for xanthochromia (yellow CSF) = definitive diagnosis
- Next step after CT shows SAH: CT Angiography (CTA) to find the aneurysm
- Hyperdensity disappears in 5-7 days as blood is reabsorbed - an early scan is essential
"CT will detect blood locally or diffusely in the subarachnoid spaces in more than 90% of cases... A large localized collection of subarachnoid blood indicates the adjacent location of the aneurysm." - Adams and Victor's Principles of Neurology, 12e
give me a image of the layout of the software of the ct scan having brain scanning
CT scan workstation software interface showing brain CT scan, DICOM viewer layout for beginners. The screen shows: a large central axial brain CT image (showing gray brain tissue with skull), smaller coronal and sagittal brain views in corners, a toolbar at top with tools like zoom, window/level, measure, annotate, scroll. Left sidebar showing patient info panel (name, DOB, study date, scan protocol "HEAD CT WITHOUT CONTRAST"). Bottom showing slice number indicator "Slice 15/32" and slice thickness "5mm". Right panel showing window/level presets labeled "Brain Window W:80 L:40", "Bone Window W:2000 L:400", "Subdural Window". HU (Hounsfield Unit) value display showing "-10 HU" at cursor. Anatomy labels overlaid on the brain CT: frontal lobe, parietal lobe, thalamus, ventricles, cerebellum. Clean professional dark-themed radiology workstation UI, educational diagram style with clear labels for each UI element.
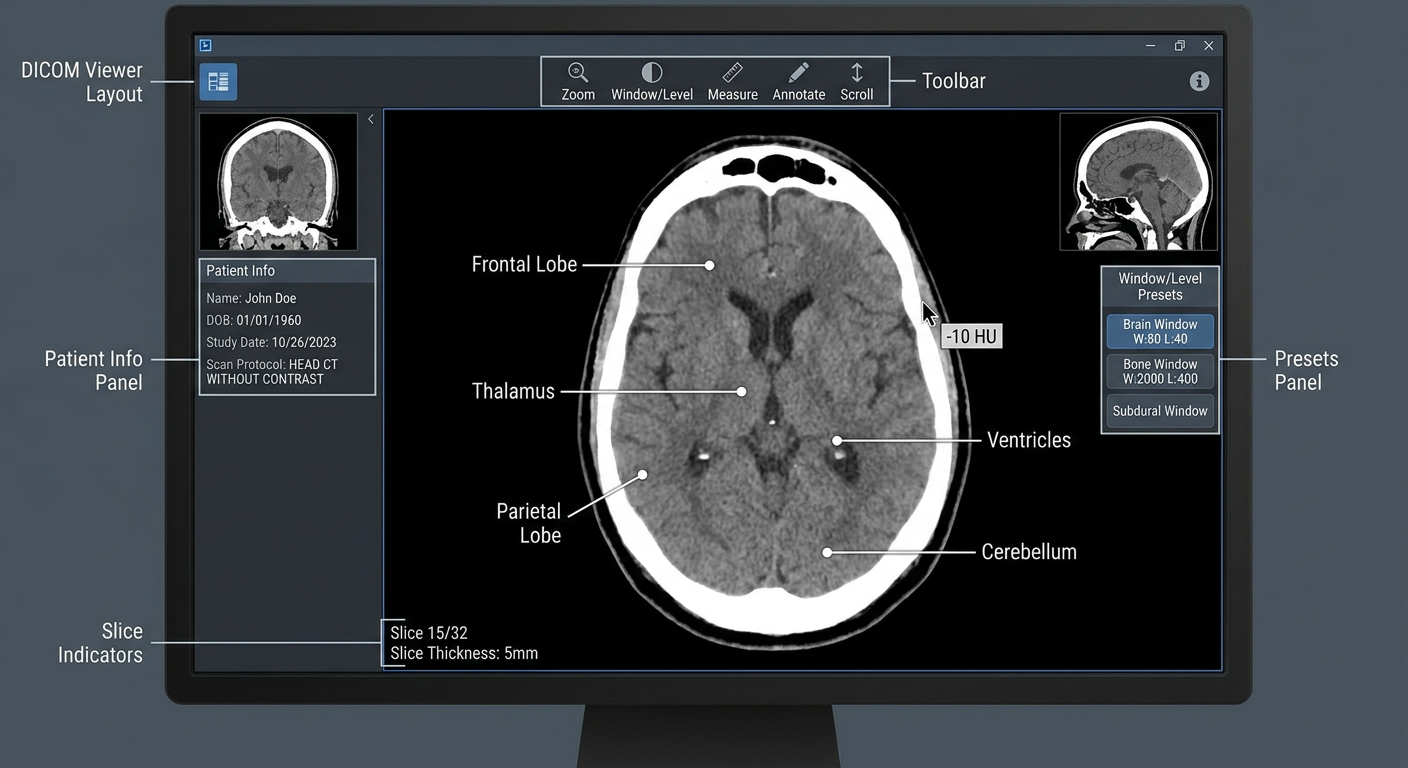
Key Areas of the CT Workstation Interface
| Area | What it does |
|---|---|
| Top Toolbar | Tools for zoom, pan, measure distances, draw annotations, and scroll through slices |
| Central Axial View | The main "top-down" cross-section of the brain - this is what you read most |
| Coronal View | Front-to-back slice (like looking at a face straight on) |
| Sagittal View | Side-to-side slice (like a profile view) |
| Patient Info Panel | Name, DOB, scan date, protocol (e.g. "Head CT without contrast") |
| Slice Indicator | Shows which slice you are on (e.g. "Slice 15/32") and thickness (e.g. 5 mm) |
| Window/Level Presets | Critical settings that control brightness/contrast of the image |
| HU Value Display | Hounsfield Units - the exact density value under your cursor |
Window Presets - Why They Matter
| Window | W / L Setting | Best for seeing |
|---|---|---|
| Brain window | W: 80 / L: 40 | Gray matter, white matter, blood (SAH, ICH) |
| Bone window | W: 2000 / L: 400 | Skull fractures, calcifications |
| Subdural window | W: 200 / L: 80 | Thin subdural hematomas |
| Soft tissue window | W: 400 / L: 40 | Scalp, soft tissue swelling |
Tip for beginners: Always look at a head CT in at least 2 windows - brain window AND bone window - so you don't miss a skull fracture hiding behind a normal-looking brain window.
Hounsfield Units (HU) - Quick Reference
| Tissue | HU Value | Appears on CT as |
|---|---|---|
| Air | -1000 | Black |
| Fat | -100 to -50 | Dark grey |
| Water/CSF | 0 | Dark grey |
| Brain (grey matter) | 37-45 | Medium grey |
| Acute blood | 50-80 | Bright white |
| Bone | 400-1000 | Very bright white |