
20260608_213336.jpg
Explain me 10 common heart disease with ecg changes and ecg images of those diseases
Reading File
Finding Sources
Finding Sources
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings with images
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
Searching the Web
STEMI inferior anterior ECG image site:litfl.com OR site:ecgwaves.com
Reading File
Loading Image
Loading Image
Loading Image
Searching the Web
atrial fibrillation ECG pericarditis Wolff-Parkinson-White ventricular tachycardia complete heart block images site:litfl.com
Loading Image
Searching the Web
atrial fibrillation ECG 12 lead pericarditis ECG saddle shaped ST elevation site:litfl.com
Loading Image
I now have extensive textbook content and ECG images. Let me also quickly note about the attached patient ECG before writing the full response.
Looking at the attached ECG (patient: Goutam Ghosh, dated 05/06/26, from Midnapore Hospital), I can see a 12-lead tracing. Now let me compose the comprehensive answer.
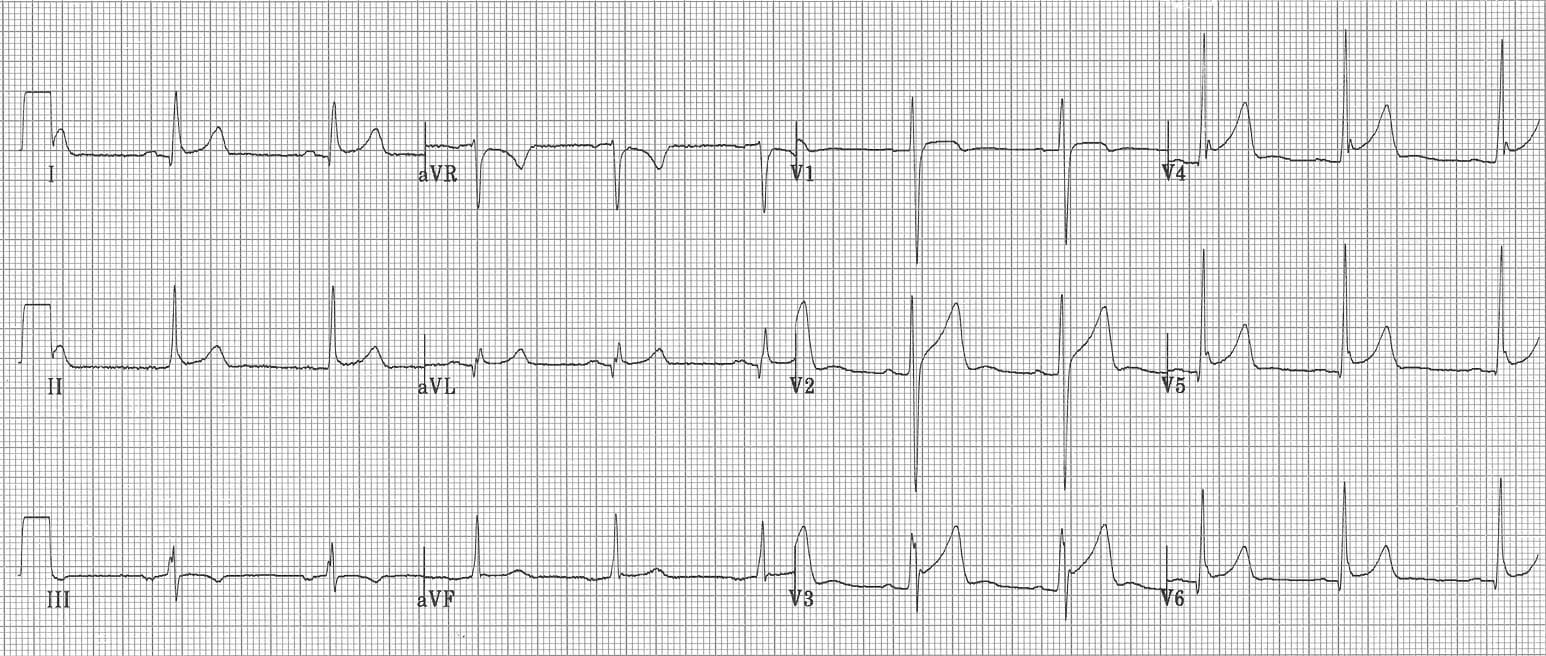
Regarding Your Attached ECG
The ECG belongs to Goutam Ghosh (Midnapore Hospital, 05/06/2026). Looking at the tracing: the rhythm appears regular with visible P waves, narrow QRS complexes, and the overall rate looks to be in the normal range. There appear to be some ST-T changes visible - but for a proper clinical interpretation, this must be evaluated by the treating physician in the clinical context.
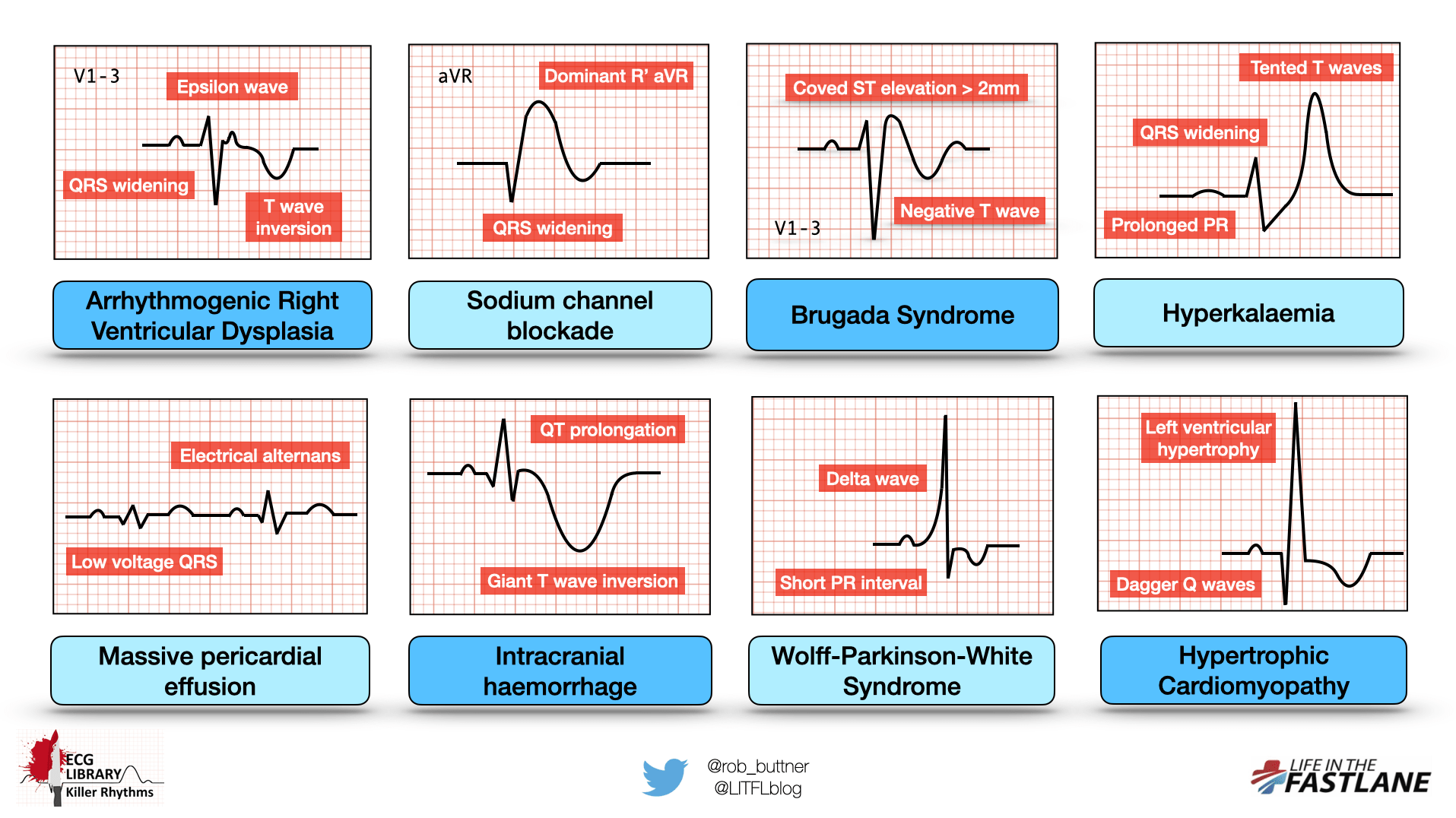
10 Common Heart Diseases with ECG Changes
Here is an overview infographic of killer ECG patterns across multiple conditions:
1. ST-Elevation Myocardial Infarction (STEMI)
What it is: Complete occlusion of a coronary artery causing transmural myocardial necrosis.
ECG Changes:
- Hyperacute T waves - the earliest finding (tall, broad, asymmetric T waves)
- ST elevation ≥1 mm in ≥2 contiguous limb leads or ≥2 mm in precordial leads
- Pathological Q waves - develops within hours to days (>40 ms wide, >25% of R wave depth)
- T wave inversion follows as repolarization changes evolve
- Reciprocal ST depression in mirror leads
Localization:
| Territory | Leads with ST elevation | Culprit Artery |
|---|---|---|
| Anterior | V1-V4 | LAD |
| Inferior | II, III, aVF | RCA (usually) |
| Lateral | I, aVL, V5-V6 | LCx |
| Posterior | ST depression V1-V3 (reciprocal) | RCA/LCx |
From Harrison's Principles: "Acute transmural anterior wall ischemia is reflected by ST elevations or increased T-wave positivity in one or more of the precordial leads (V1-V6) and leads I and aVL. Inferior wall ischemia produces changes in leads II, III, and aVF."
ECG - Anterior STEMI (Wellens T-wave sign - pre-infarction LAD stenosis):
 Deep symmetric T-wave inversions V1-V6 indicating critical LAD stenosis (Wellens pattern) - Harrison's 22E
Deep symmetric T-wave inversions V1-V6 indicating critical LAD stenosis (Wellens pattern) - Harrison's 22E
ECG - Inferior STEMI with Complete Heart Block:
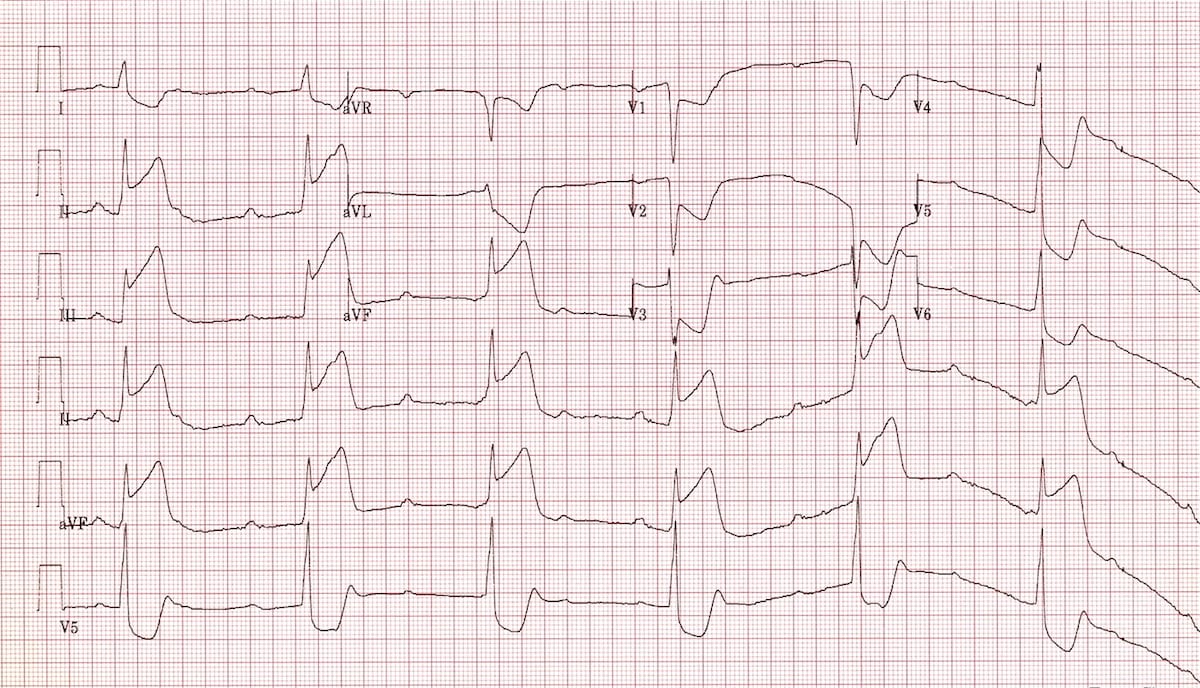 ST elevation in II, III, aVF with reciprocal depression in I, aVL. Note complete heart block (a complication of inferior MI due to RCA occlusion).
ST elevation in II, III, aVF with reciprocal depression in I, aVL. Note complete heart block (a complication of inferior MI due to RCA occlusion).
2. Non-ST Elevation MI (NSTEMI) / Unstable Angina
What it is: Partial coronary occlusion or severe subendocardial ischemia without full-thickness necrosis.
ECG Changes:
- ST depression (horizontal or downsloping) - most significant finding
- T wave inversions in multiple leads
- No pathological Q waves (by definition)
- aVR ST elevation often accompanies widespread ST depression (suggests left main or proximal LAD disease)
- ECG may be completely normal in up to 6% of cases
Key point from Tintinalli's: "The diagnosis of NSTEMI depends on abnormal elevation of cardiac biomarkers but may include ECG changes not meeting criteria for STEMI."
3. Atrial Fibrillation (AF)
What it is: Chaotic, disorganized atrial electrical activity causing irregular ventricular response. Most common sustained arrhythmia.
ECG Changes:
- No discernible P waves - replaced by fibrillatory baseline (f waves), most visible in V1
- Irregularly irregular R-R intervals - the hallmark
- Narrow QRS (unless aberrant conduction or bundle branch block)
- Ventricular rate typically 100-180 bpm if uncontrolled
- Coarse AF - large fibrillatory waves (often seen with mitral stenosis)
- Fine AF - small fibrillatory waves (seen with long-standing AF)
ECG - AF with WPW (extremely irregular, wide, bizarre QRS complexes):
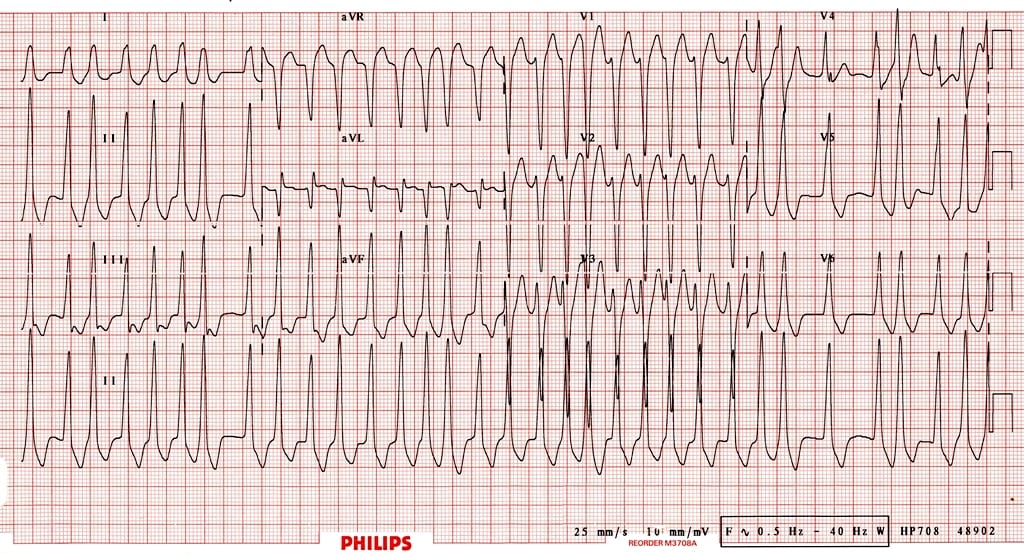 Irregular irregular rhythm with varying QRS morphology - AF conducted via accessory pathway in WPW. This is life-threatening.
Irregular irregular rhythm with varying QRS morphology - AF conducted via accessory pathway in WPW. This is life-threatening.
4. Acute Pericarditis
What it is: Inflammation of the pericardium, most commonly viral. Causes pleuritic chest pain.
ECG Changes (evolve through 4 stages):
- Stage 1 (days 1-2): Diffuse concave ("saddle-shaped") ST elevation in almost ALL leads (I, II, III, aVF, V2-V6) + PR depression (most specific finding) + PR elevation in aVR
- Stage 2 (days 3-7): ST normalizes, T waves flatten
- Stage 3 (1-3 weeks): T wave inversions (may look like ischemia)
- Stage 4 (months): ECG returns to normal
Key differentiator from STEMI:
- ST elevation is CONCAVE (smiley face), not convex
- Affects ALL leads (no territorial pattern)
- PR depression present
- No reciprocal ST depression (except aVR)
- No Q waves
ECG - Pericarditis:
 Concave ST elevation across multiple leads with PR depression - classic pericarditis pattern.
Concave ST elevation across multiple leads with PR depression - classic pericarditis pattern.
5. Left Bundle Branch Block (LBBB)
What it is: Conduction failure through the left bundle branch, causing delayed and abnormal left ventricular activation. A new LBBB with chest pain is treated as STEMI-equivalent.
ECG Changes:
- QRS duration ≥120 ms (broad QRS)
- Broad, notched ("M-shaped") R wave in lateral leads (I, aVL, V5, V6)
- Deep S wave in V1 (rS or QS pattern)
- No septal Q waves in lateral leads
- ST and T wave changes are DISCORDANT (opposite to QRS direction) - this is normal in LBBB, making ischemia diagnosis difficult
- Left axis deviation often present
Sgarbossa criteria are used to detect MI in the presence of LBBB:
- Concordant ST elevation ≥1 mm in any lead
- Concordant ST depression ≥1 mm in V1-V3
- Discordant ST elevation ≥5 mm (or ST/S ratio ≥0.25 in Smith-modified criteria)
6. Complete Heart Block (Third-Degree AV Block)
What it is: Complete failure of conduction between atria and ventricles. Atria and ventricles beat independently.
ECG Changes:
- P waves present at a regular, faster rate (atrial rate ~60-100)
- QRS complexes present at a regular, SLOWER rate (ventricular rate ~20-40 if junctional escape) - completely independent
- No relationship between P waves and QRS - "AV dissociation"
- Narrow QRS if junctional escape pacemaker (above His bundle)
- Wide QRS (≥120 ms) if ventricular escape pacemaker (below His bundle) - more dangerous
- Regular R-R intervals (unlike AF)
Common causes: Inferior MI (RCA occlusion affecting AV node), Lyme disease, digoxin toxicity, congenital.
7. Wolff-Parkinson-White (WPW) Syndrome
What it is: Pre-excitation syndrome caused by an accessory pathway (Bundle of Kent) bypassing the AV node, allowing early ventricular activation.
ECG Changes (the classic delta wave triad):
- Short PR interval (<120 ms) - because impulse bypasses AV node delay
- Delta wave - slurred upstroke at the beginning of QRS (pre-excitation of ventricles)
- Wide QRS (≥120 ms) - due to abnormal ventricular conduction
- ST-T changes discordant to QRS (secondary changes)
- Pseudo-Q waves / pseudo-infarction pattern in some leads
Risk: If AF develops in WPW, the accessory pathway can conduct 300+ impulses/minute to ventricles, causing ventricular fibrillation and sudden death. Never use AV nodal blockers (adenosine, verapamil, diltiazem) in WPW+AF.
8. Hypertrophic Cardiomyopathy (HCM)
What it is: Genetic disorder causing asymmetric LV hypertrophy (often septal), with diastolic dysfunction and LVOT obstruction.
ECG Changes:
- Left ventricular hypertrophy (LVH) - tall R waves in V5-V6, deep S in V1-V2 (Sokolow-Lyon: S V1 + R V5 ≥35 mm)
- Deep, narrow ("dagger") Q waves in lateral and inferior leads - due to septal hypertrophy (NOT infarction Q waves)
- Giant T wave inversions in lateral precordial leads
- Left axis deviation
- ST depression in multiple leads
- Apical variant HCM: massive T wave inversions in V3-V5 ("giant negative T waves")
Harrison's: Abnormal Q waves were once considered markers of transmural MI, but they occur in HCM due to septal depolarization abnormalities.
9. Pulmonary Embolism (PE)
What it is: Obstruction of pulmonary arterial system causing acute right heart strain.
ECG Changes:
- Sinus tachycardia - most common finding (40% of cases)
- S1Q3T3 pattern - deep S wave in lead I, Q wave in lead III, T-wave inversion in lead III (seen in ~20%, classic but not sensitive)
- Right bundle branch block (complete or incomplete) - due to acute RV pressure overload
- Right axis deviation
- T wave inversions in V1-V4 (right ventricular strain)
- Atrial fibrillation or flutter
- ECG may be normal in up to 30% of PE cases
From Tintinalli's: "ECG findings most commonly include sinus tachycardia and atrial fibrillation."
From Fuster's Heart: "ECG findings in acute PE are generally nonspecific and include T-wave changes, ST-segment abnormalities, incomplete or complete right bundle-branch block, right axis deviation."
10. Left Ventricular Hypertrophy (LVH)
What it is: Thickening of the left ventricular wall due to chronic pressure or volume overload (hypertension, aortic stenosis, HCM).
ECG Changes:
- Voltage criteria:
- Sokolow-Lyon: S in V1 + R in V5 or V6 ≥35 mm
- Cornell: R in aVL + S in V3 ≥28 mm (men), ≥20 mm (women)
- Left axis deviation (more negative than -30°)
- ST depression + T wave inversion in lateral leads (I, aVL, V5-V6) - "strain pattern" or "LV strain" - indicates significant hypertrophy
- Prolonged QRS duration (sometimes)
- Left atrial enlargement (P wave >120 ms, bifid in lead II, biphasic in V1)
Hypertensive patients may also develop:
- Q-T prolongation
- Bundle branch blocks
Summary Table
| Condition | Rate | Rhythm | P Wave | PR | QRS | ST-T Changes |
|---|---|---|---|---|---|---|
| STEMI | Variable | Regular | Normal | Normal | Normal/Q | ST elevation + Q waves |
| NSTEMI/UA | Variable | Regular | Normal | Normal | Normal | ST depression, T inversion |
| Atrial Fibrillation | 100-180 | Irregular | Absent (f waves) | None | Narrow | Variable |
| Pericarditis | Variable | Regular | Normal | Depressed | Normal | Diffuse concave ST elevation |
| LBBB | Variable | Regular | Normal | Normal | Wide (≥120) | Discordant ST-T |
| 3rd Degree AVB | Slow (~40) | Regular | Regular, faster | No relation | Wide | Variable |
| WPW | Variable | Regular | Normal | Short (<120ms) | Wide + delta | Discordant |
| HCM | Variable | Regular | Normal | Normal | LVH + Q | Deep Q, giant T inversion |
| Pulmonary Embolism | Tachy | Regular | Normal | Normal | RBBB ± | S1Q3T3, T inv V1-V4 |
| LVH | Variable | Regular | LAE ± | Normal | Tall voltage | Strain pattern |
Important Clinical Note: ECG must always be interpreted in the clinical context. A normal ECG does not rule out acute MI (occurs in ~6% of cases), and non-specific ST changes can be seen in many conditions. Serial ECGs and troponin levels are required in any patient with suspected ACS. - Harrison's 22E
Sources: Harrison's Principles of Internal Medicine 22E, Tintinalli's Emergency Medicine, Fuster and Hurst's The Heart 15th Ed., Braunwald's Heart Disease; ECG images from LITFL ECG Library and Harrison's 22E.
This is a shared conversation. Sign in to Orris to start your own chat.